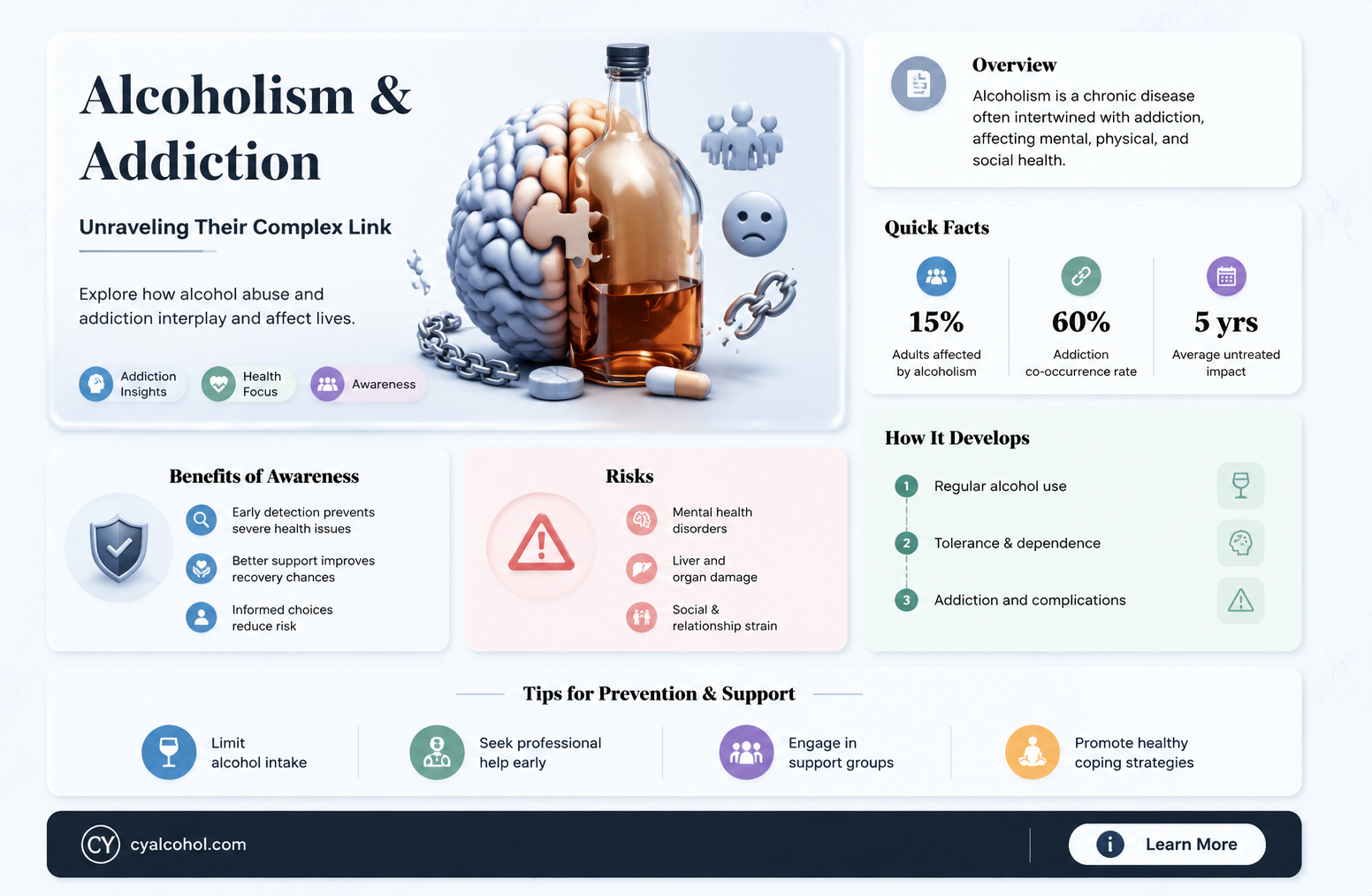
The question of whether alcoholics are addicts is a nuanced and critical one, as it intersects with both medical and societal definitions of addiction. Alcoholism, clinically referred to as alcohol use disorder (AUD), is characterized by an inability to control or stop drinking despite adverse consequences, which aligns closely with the broader criteria for addiction. Addiction, as defined by the American Psychiatric Association, involves compulsive substance use, loss of control, and negative consequences, all of which are hallmark features of severe AUD. While not all individuals who consume alcohol develop addiction, those diagnosed with alcoholism exhibit behaviors and neurological changes consistent with addictive disorders, such as altered brain chemistry and cravings. Recognizing alcoholics as addicts underscores the need for comprehensive treatment approaches, including therapy, medication, and support systems, to address the complex interplay of biological, psychological, and social factors driving their condition.
| Characteristics | Values |
|---|---|
| Definition | Alcoholics are individuals with Alcohol Use Disorder (AUD), a chronic relapsing brain disorder characterized by compulsive alcohol use, loss of control over intake, and negative emotional state when not using. |
| Addiction Classification | Yes, alcoholism is classified as an addiction by major health organizations (e.g., WHO, NIH, DSM-5). It shares core features with other substance use disorders. |
| Brain Changes | Chronic alcohol use alters brain chemistry, particularly dopamine and GABA systems, leading to cravings and dependence. |
| Tolerance | Alcoholics develop tolerance, requiring more alcohol to achieve the same effect over time. |
| Withdrawal Symptoms | Physical and psychological withdrawal symptoms (e.g., tremors, anxiety, seizures) occur when alcohol use is reduced or stopped. |
| Loss of Control | Inability to limit alcohol consumption despite negative consequences. |
| Neglect of Responsibilities | Prioritizing alcohol over work, relationships, and personal obligations. |
| Continued Use Despite Harm | Persistent alcohol use despite physical, mental, or social harm. |
| Time Spent on Alcohol | Excessive time spent drinking, recovering from drinking, or obtaining alcohol. |
| Failed Attempts to Quit | Repeated unsuccessful efforts to cut down or quit alcohol use. |
| Cravings | Strong, persistent desire or urge to consume alcohol. |
| Social and Behavioral Impact | Alcohol use leads to social isolation, legal problems, and risky behaviors. |
| Genetic Predisposition | Genetic factors contribute to 40-60% of AUD risk. |
| Environmental Factors | Stress, peer influence, and availability of alcohol increase risk. |
| Treatment Options | Includes detoxification, therapy (e.g., CBT), medications (e.g., naltrexone, disulfiram), and support groups (e.g., AA). |
| Relapse Rates | Relapse rates for AUD are similar to other chronic diseases (40-60%), emphasizing the need for ongoing management. |
Explore related products


$9.33 $14.95




What You'll Learn
- Biological Basis: Genetic predisposition and brain chemistry changes in alcoholics vs. other addicts
- Behavioral Patterns: Compulsive drinking behaviors compared to drug addiction cycles
- Withdrawal Symptoms: Physical and psychological withdrawal similarities between alcohol and drugs
- Treatment Approaches: Overlapping therapies for alcoholism and substance addiction
- Social Stigma: Societal perceptions of alcoholics versus other types of addicts
![]()
Biological Basis: Genetic predisposition and brain chemistry changes in alcoholics vs. other addicts
Alcoholism and addiction share a complex biological foundation, but the interplay of genetics and brain chemistry in alcoholics differs subtly yet significantly from other substance use disorders. Research indicates that genetic predisposition plays a substantial role in alcoholism, with heritability estimates ranging from 40% to 60%. Specific genes, such as those involved in alcohol metabolism (e.g., *ADH1B* and *ALDH2*), influence how the body processes alcohol, affecting an individual’s risk. For instance, variants of *ADH1B* that accelerate the conversion of alcohol to acetaldehyde, a toxic byproduct, can deter heavy drinking by causing unpleasant symptoms like flushing and nausea. However, in those without such protective variants, the absence of these deterrents may increase susceptibility to alcoholism.
Brain chemistry changes in alcoholics are both a cause and consequence of prolonged drinking. Chronic alcohol exposure alters neurotransmitter systems, particularly gamma-aminobutyric acid (GABA) and glutamate, which regulate inhibition and excitation in the brain. Over time, the brain compensates for alcohol’s depressant effects by reducing GABA receptors and increasing glutamate activity, leading to tolerance and withdrawal symptoms. This neuroadaptation is similar to other addictions but differs in specificity: while opioid addiction primarily affects the dopamine reward pathway, alcoholism involves a broader disruption of stress and emotional regulation systems, such as the hypothalamic-pituitary-adrenal (HPA) axis. This distinction explains why alcoholics often experience heightened anxiety and dysphoria during withdrawal, compared to the more pronounced physical symptoms seen in opioid withdrawal.
Comparatively, other addicts exhibit similar but not identical brain chemistry changes. For example, stimulant users (e.g., cocaine or methamphetamine) experience profound alterations in dopamine signaling, leading to impaired reward processing and compulsive drug-seeking behavior. In contrast, alcoholics show more pronounced changes in the brain’s stress systems, which may contribute to their higher relapse rates when exposed to stressors. A study published in *Neuropsychopharmacology* found that alcoholics had a 30% higher cortisol response to stress compared to non-alcoholics, highlighting the unique role of stress dysregulation in alcohol addiction.
Practical implications of these biological differences are significant. Treatment approaches must account for the distinct genetic and neurochemical profiles of alcoholics. For instance, medications like naltrexone, which blocks opioid receptors to reduce cravings, have shown efficacy in alcoholics by modulating the brain’s reward system. However, its effectiveness varies based on genetic factors, such as the presence of the *OPRM1* A118G variant, which influences response to treatment. Similarly, behavioral therapies that address stress management, such as mindfulness-based interventions, may be particularly beneficial for alcoholics due to their heightened stress reactivity.
In summary, while alcoholics and other addicts share a common biological framework of addiction, the genetic predisposition and brain chemistry changes in alcoholics are uniquely tailored to the properties of alcohol and its effects on the body. Understanding these distinctions is crucial for developing targeted interventions that address the specific vulnerabilities of alcoholics, ultimately improving treatment outcomes and reducing relapse rates.
Alcohol and Antihistamines: A Risky Mix or Safe Combination?
You may want to see also
Explore related products






![]()
Behavioral Patterns: Compulsive drinking behaviors compared to drug addiction cycles
Alcoholics and drug addicts often exhibit strikingly similar behavioral patterns, rooted in compulsive actions driven by a need to consume their substance of choice. Both groups experience a loss of control, prioritizing their substance over responsibilities, relationships, and health. For alcoholics, this might manifest as repeated binge drinking episodes—defined by the National Institute on Alcohol Abuse and Alcoholism as consuming 5 or more drinks for men, or 4 or more for women, in about 2 hours. Drug addicts, similarly, may engage in escalating doses or frequency of use, often surpassing intended limits despite adverse consequences. This compulsivity stems from a hijacked brain reward system, where the substance becomes the primary source of dopamine release, overshadowing natural rewards like food or social interaction.
Consider the cycle of use and withdrawal. Alcoholics frequently experience intense cravings, followed by consumption that temporarily alleviates anxiety or stress, only to be met with guilt, physical discomfort, or blackouts. This mirrors the drug addiction cycle, where users chase the initial euphoria, endure the comedown, and face withdrawal symptoms that reinforce the need to use again. For instance, opioid addicts may experience severe withdrawal symptoms like muscle aches, nausea, and insomnia within 6-12 hours of last use, driving them back to the drug. Alcohol withdrawal, though different, can be equally dangerous, with symptoms like seizures or delirium tremens emerging 48-72 hours after cessation, often necessitating medical intervention. Both cycles create a self-perpetuating loop, making cessation without professional help exceedingly difficult.
A key distinction lies in the social perception and accessibility of alcohol versus drugs. Alcohol is legally and culturally normalized in many societies, making compulsive drinking behaviors harder to identify and address. For example, a person consuming 6-8 drinks daily might be dismissed as a "heavy drinker" rather than an addict, delaying intervention. In contrast, drug use often carries a stigma that, while harmful in its own right, can sometimes prompt earlier recognition of addiction. However, this normalization of alcohol can lead to higher rates of long-term, undetected addiction, increasing risks like liver disease, which affects 15-20% of heavy drinkers after a decade of excessive consumption. Drug addiction, meanwhile, may present more immediate risks, such as overdose, but both substances demand tailored treatment approaches.
To break these cycles, understanding the behavioral patterns is crucial. For alcoholics, setting clear limits—such as no more than 1 drink per day for women and 2 for men, as per dietary guidelines—can be a starting point, though complete abstinence is often necessary for severe cases. Drug addicts may benefit from harm reduction strategies, like methadone maintenance for opioid addiction, which reduces cravings and withdrawal symptoms. Both groups require behavioral therapies, such as Cognitive Behavioral Therapy (CBT), to address underlying triggers and develop coping mechanisms. Support groups like AA or NA provide community and accountability, though success rates vary widely, with studies showing long-term sobriety rates around 20-30% for both alcoholics and drug addicts. Recognizing these patterns early and intervening with evidence-based methods can significantly improve outcomes, regardless of the substance involved.
Does Alcohol Lighten Periods? Unraveling Myths and Facts About Menstruation
You may want to see also
Explore related products






![]()
Withdrawal Symptoms: Physical and psychological withdrawal similarities between alcohol and drugs
Alcohol and drugs, when abused, leave a trail of withdrawal symptoms that blur the lines between physical and psychological distress. Both substances, when abruptly ceased, trigger a cascade of reactions as the body and mind struggle to regain equilibrium. This phenomenon underscores the addictive nature of alcohol, often categorizing alcoholics as addicts akin to drug users. The similarities in withdrawal symptoms highlight the shared neurochemical pathways disrupted by these substances, particularly those involving dopamine, serotonin, and GABA.
Physically, withdrawal from both alcohol and drugs can manifest in alarming ways. Alcohol withdrawal, for instance, may include tremors, sweating, and nausea, often peaking within 24 to 72 hours after the last drink. Similarly, opioid withdrawal presents with muscle aches, diarrhea, and dilated pupils, typically beginning 8 to 12 hours after the last dose. Both scenarios can escalate to life-threatening conditions like seizures or delirium tremens, requiring immediate medical intervention. The severity often correlates with the duration and intensity of substance use, emphasizing the importance of supervised detoxification.
Psychologically, the withdrawal parallels are equally striking. Anxiety, irritability, and insomnia are common across both alcohol and drug cessation. These symptoms stem from the brain’s attempt to recalibrate neurotransmitter levels, often resulting in mood swings and cognitive fog. For example, long-term alcoholics and chronic benzodiazepine users may experience protracted withdrawal, where psychological symptoms like depression and anxiety persist for months. Such overlap suggests that the brain’s reward system, hijacked by both substances, demands time and support to heal.
Addressing these withdrawal symptoms requires a dual approach. Medically, tapering doses under professional guidance can mitigate physical risks, while medications like benzodiazepines (for alcohol) or methadone (for opioids) ease the transition. Psychologically, therapy and support groups provide coping mechanisms for emotional turmoil. Practical tips include maintaining hydration, adopting a balanced diet, and engaging in mindfulness practices to alleviate stress. Recognizing these similarities not only validates the classification of alcoholics as addicts but also underscores the need for holistic treatment strategies.
In conclusion, the physical and psychological withdrawal symptoms of alcohol and drugs share profound similarities, rooted in their impact on the brain and body. Understanding these parallels is crucial for effective treatment, emphasizing that alcoholics, like drug addicts, require comprehensive care to navigate the challenges of recovery. Whether through medical intervention, psychological support, or lifestyle adjustments, addressing withdrawal holistically can pave the way for lasting sobriety.
Unveiling Alcohol's Origins: The Surprising Ingredients of Ancient Brews
You may want to see also
Explore related products


$14.87 $15.99


![]()
Treatment Approaches: Overlapping therapies for alcoholism and substance addiction
Alcoholism and substance addiction often share underlying psychological and physiological mechanisms, making overlapping treatment approaches not only common but highly effective. Therapies like Cognitive Behavioral Therapy (CBT) are cornerstone interventions for both conditions. CBT helps individuals identify and modify destructive thought patterns and behaviors, replacing them with healthier coping strategies. For instance, a 30-year-old with a decade-long alcohol dependency might work with a therapist to recognize triggers, such as stress or social pressure, and develop alternative responses, like mindfulness exercises or physical activity. Studies show that CBT reduces relapse rates by up to 50% in both alcoholics and drug addicts when combined with other treatments.
Pharmacotherapy further bridges the gap between alcoholism and substance addiction treatment. Medications like naltrexone, originally approved for opioid addiction, are now widely used to treat alcohol dependence by blocking the euphoric effects of alcohol. Similarly, acamprosate helps restore the brain’s chemical balance disrupted by chronic alcohol use, reducing cravings. For opioid addiction, methadone and buprenorphine are prescribed to stabilize patients and reduce withdrawal symptoms. These medications often require precise dosing—for example, buprenorphine is typically started at 4–8 mg daily and adjusted based on response. Combining these drugs with behavioral therapies enhances their efficacy, addressing both the physical and psychological aspects of addiction.
Holistic therapies, such as mindfulness-based relapse prevention (MBRP), offer another layer of overlapping treatment. MBRP teaches individuals to observe cravings without reacting to them, fostering greater self-awareness and emotional regulation. A 45-year-old recovering from both alcohol and cocaine addiction might practice daily meditation and breathing exercises to manage stress, a common trigger for relapse. Research indicates that MBRP reduces relapse rates by 30–40% across substance use disorders. This approach is particularly valuable for dual diagnoses, where individuals struggle with both addiction and mental health disorders like anxiety or depression.
Group therapy and 12-step programs, such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA), provide communal support that transcends specific substances. These programs emphasize shared experiences, accountability, and a structured path to recovery. While AA focuses on alcohol, its principles—like admitting powerlessness over addiction and seeking a higher power—apply equally to drug addiction. Many treatment centers integrate these programs into their curricula, offering weekly meetings and sponsorship opportunities. Practical tips for maximizing their benefits include attending meetings consistently, actively participating in discussions, and finding a sponsor within the first month of engagement.
Finally, family therapy plays a critical role in treating both alcoholism and substance addiction by addressing relational dynamics that contribute to or exacerbate addictive behaviors. For example, a therapist might work with a 25-year-old heroin addict and their parents to improve communication, set boundaries, and rebuild trust. This approach not only supports the individual’s recovery but also equips family members with tools to cope with the challenges of addiction. Studies show that involving family in treatment increases long-term sobriety rates by 20–30%. Practical steps include scheduling regular family sessions, setting clear expectations, and encouraging open dialogue about recovery progress and setbacks.
The State of Ethyl Alcohol at Room Temperature
You may want to see also
Explore related products






![]()
Social Stigma: Societal perceptions of alcoholics versus other types of addicts
Alcoholics and addicts often face societal judgment, but the stigma attached to alcoholism differs significantly from that of other addictions. Consider the cultural normalization of alcohol: it’s a staple at celebrations, business meetings, and social gatherings. A person drinking a glass of wine at dinner is rarely questioned, whereas someone using prescription opioids, even as directed, may be met with suspicion. This double standard highlights how society views alcoholics as more "functional" or "acceptable" compared to other addicts, despite the severity of alcohol-related harm. For instance, alcohol contributes to over 3 million deaths annually worldwide, yet it remains a socially sanctioned substance.
To understand this disparity, examine the language used to describe alcoholics versus other addicts. Terms like "wine mom" or "beer enthusiast" often carry a lighthearted tone, minimizing the seriousness of alcohol dependence. In contrast, labels such as "junkie" or "crackhead" are laden with moral judgment and dehumanization. This linguistic nuance reflects societal attitudes: alcoholics are seen as struggling with a bad habit, while other addicts are perceived as morally flawed. A practical tip for challenging this stigma is to replace judgmental language with neutral terms like "person with a substance use disorder," regardless of the substance involved.
The legal and institutional treatment of alcoholics versus other addicts further illustrates this stigma. Alcohol is legal and regulated, with age restrictions (e.g., 21 in the U.S.), whereas drugs like heroin or methamphetamine are criminalized. This legal framework reinforces the idea that alcohol use is a matter of personal choice, while other addictions are criminal acts. For example, a person arrested for public intoxication might receive a fine or mandatory treatment, but someone caught with illicit drugs could face years in prison. This disparity perpetuates the notion that alcoholics are more deserving of empathy and support, while other addicts are seen as threats to society.
Finally, societal perceptions of recovery differ drastically between alcoholics and other addicts. Alcoholics Anonymous (AA) and similar programs are widely recognized and respected, with recovery stories often celebrated in media. In contrast, recovery from other addictions is frequently met with skepticism or disbelief. For instance, a former alcoholic might be praised for their "willpower," while a recovering opioid user may be viewed as untrustworthy, even years into sobriety. To combat this, advocate for equal recognition of all recovery journeys and challenge the notion that some addictions are more "valid" than others. This shift in perspective is essential for dismantling the stigma that divides addicts along arbitrary lines.
Alcohol Dependence: Are You an Alcoholic?
You may want to see also
Frequently asked questions
Yes, alcoholics are considered addicts because they have a physical and psychological dependence on alcohol, which is a hallmark of addiction.
Typically, alcoholics struggle to control their drinking due to the addictive nature of alcohol, which affects the brain’s reward system and decision-making processes.
Alcoholism is a form of addiction specifically tied to alcohol. It falls under the broader category of substance use disorders.
Yes, alcoholics can experience severe withdrawal symptoms, such as tremors, anxiety, and seizures, similar to those seen in other substance addictions.
It’s rare, as alcoholism inherently involves dependence and compulsive behavior, which are key signs of addiction. However, the severity of symptoms can vary.