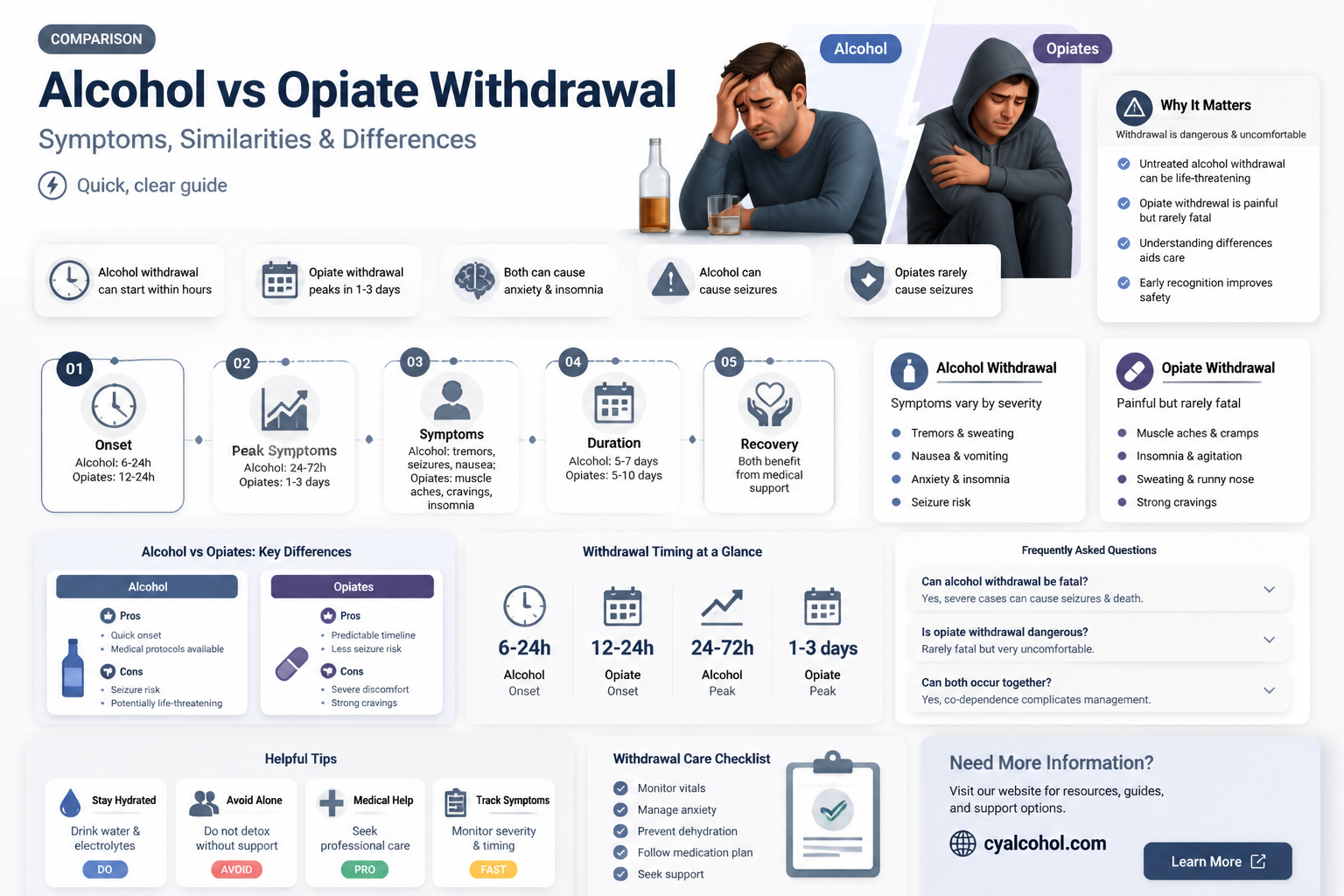
Alcohol and opiate withdrawal systems, while distinct in their underlying mechanisms, share some overlapping symptoms and challenges due to their impact on the central nervous system. Both substances alter brain chemistry, leading to physical and psychological dependence, and abrupt cessation results in withdrawal symptoms that can range from mild to life-threatening. Alcohol withdrawal often involves symptoms like tremors, anxiety, and seizures, primarily due to its effects on GABA and glutamate receptors, whereas opiate withdrawal typically includes symptoms such as muscle aches, nausea, and intense cravings, stemming from disruptions in the brain’s opioid receptor system. Despite these differences, both withdrawal processes can be managed with medical supervision, often involving medications like benzodiazepines for alcohol and methadone or buprenorphine for opiates, alongside supportive care to address shared challenges such as dehydration, insomnia, and psychological distress. Understanding these similarities and differences is crucial for effective treatment and recovery.
Explore related products





What You'll Learn
- Symptom Overlap: Nausea, anxiety, insomnia, and sweating are common in both alcohol and opiate withdrawal
- Timeline Differences: Alcohol withdrawal peaks earlier (24-72 hours) vs. opiates (72 hours)
- Severity Factors: Alcohol withdrawal can be life-threatening (seizures, delirium tremens)
- Treatment Approaches: Medications like benzodiazepines for alcohol, methadone or buprenorphine for opiates
- Psychological Impact: Both cause depression, anxiety, and cravings, but intensity varies
![]()
Symptom Overlap: Nausea, anxiety, insomnia, and sweating are common in both alcohol and opiate withdrawal
Withdrawal from both alcohol and opiates can be a challenging and physically demanding process, often presenting with a range of distressing symptoms. Interestingly, there is a notable overlap in the symptoms experienced during the withdrawal phases of these two substances, particularly when it comes to nausea, anxiety, insomnia, and sweating. These shared symptoms highlight the similarities in the body's response to the absence of these addictive substances.
Nausea and Gastrointestinal Distress: One of the most common symptoms experienced during both alcohol and opiate withdrawal is nausea. This can range from a mild queasy feeling to severe vomiting. The body's gastrointestinal system is highly sensitive during withdrawal, and both substances' absence can lead to similar digestive issues. Opiate withdrawal often includes abdominal cramps and diarrhea, while alcohol withdrawal may cause stomach pain and nausea, sometimes accompanied by vomiting. These symptoms can be extremely uncomfortable and may lead to dehydration, emphasizing the need for medical supervision during detoxification.
Anxiety and Psychological Distress: Anxiety is a significant psychological symptom that individuals undergoing alcohol or opiate withdrawal often face. The absence of these substances can trigger intense feelings of nervousness, restlessness, and even panic attacks. Opiate withdrawal is known to induce severe anxiety, which may be accompanied by paranoia and depression. Similarly, alcohol withdrawal can result in heightened anxiety, agitation, and mood swings. These psychological symptoms can be overwhelming and may require therapeutic interventions and medication to manage effectively.
Insomnia and Sleep Disturbances: Sleep disturbances are prevalent in both withdrawal syndromes. Insomnia, characterized by difficulty falling asleep or staying asleep, is a common complaint. Opiate withdrawal often leads to vivid and unpleasant dreams, making it hard for individuals to achieve restful sleep. Alcohol withdrawal can also disrupt sleep patterns, causing insomnia and, in some cases, night sweats. The body's attempt to regulate itself without the presence of these substances can result in significant sleep challenges, which may persist for several days or weeks.
Sweating and Autonomic Hyperactivity: Excessive sweating, or diaphoresis, is another symptom that overlaps in alcohol and opiate withdrawal. This is often accompanied by increased heart rate, elevated blood pressure, and body temperature dysregulation. Opiate withdrawal may cause cold sweats and goosebumps, a phenomenon known as 'cold turkey.' Alcohol withdrawal can also lead to profuse sweating, especially during the acute phase. These symptoms are part of the body's autonomic response to the absence of the substances, indicating the need for medical management to prevent more severe complications.
The symptom overlap in nausea, anxiety, insomnia, and sweating during alcohol and opiate withdrawal provides insight into the complex nature of substance dependence and the body's reaction to cessation. Understanding these similarities can help healthcare professionals develop comprehensive treatment plans, ensuring that individuals receive the necessary support and medications to manage these challenging symptoms effectively. It also underscores the importance of personalized care, as the severity and duration of these symptoms can vary widely among individuals.
Americans' Alcohol Consumption: How Many Gallons Do They Drink?
You may want to see also
Explore related products






![]()
Timeline Differences: Alcohol withdrawal peaks earlier (24-72 hours) vs. opiates (72 hours)
When comparing the withdrawal timelines of alcohol and opiates, one of the most notable differences is the time it takes for symptoms to peak. Alcohol withdrawal symptoms typically reach their maximum intensity much earlier than those of opiates. For individuals discontinuing alcohol, the peak of withdrawal symptoms generally occurs within 24 to 72 hours after the last drink. This rapid onset is due to the body’s quick adjustment to the absence of alcohol, a central nervous system depressant. During this period, symptoms such as tremors, anxiety, hypertension, and in severe cases, seizures or delirium tremens (DTs), can manifest. The early peak of alcohol withdrawal underscores the urgency of medical supervision during this critical window, as complications like DTs can be life-threatening.
In contrast, opiate withdrawal follows a more prolonged timeline, with symptoms peaking around 72 hours after the last dose. Opiates, such as heroin or prescription painkillers, act on the brain’s reward system and alter its chemistry over time. When opiates are discontinued, the body requires additional time to recalibrate, leading to a slower onset of withdrawal symptoms. Common symptoms include muscle aches, nausea, diarrhea, and intense cravings. While opiate withdrawal is generally less life-threatening than alcohol withdrawal, the prolonged peak period can make it extremely challenging for individuals to manage without support. This extended timeline highlights the importance of gradual tapering or medication-assisted treatment (MAT) to ease the process.
The timeline differences between alcohol and opiate withdrawal have significant implications for treatment approaches. Alcohol withdrawal’s early peak necessitates immediate medical intervention, often involving medications like benzodiazepines to prevent seizures and manage anxiety. Inpatient care is frequently recommended to monitor vital signs and address complications promptly. On the other hand, opiate withdrawal’s delayed peak allows for more flexibility in treatment settings, with options ranging from outpatient programs to MAT using drugs like methadone or buprenorphine. Understanding these timeline differences is crucial for healthcare providers to tailor interventions effectively and improve patient outcomes.
Another critical aspect of these timeline differences is the psychological impact on individuals undergoing withdrawal. The rapid peak of alcohol withdrawal can be overwhelming, often leading to heightened anxiety and fear of complications. This intensity may deter individuals from seeking help or completing treatment. Conversely, the prolonged peak of opiate withdrawal can test an individual’s resolve, as symptoms persist for a longer duration, increasing the risk of relapse. Addressing these psychological challenges requires a combination of counseling, support groups, and, in some cases, dual diagnosis treatment for co-occurring mental health disorders.
In summary, the timeline differences between alcohol and opiate withdrawal—with alcohol peaking earlier (24-72 hours) and opiates peaking around 72 hours—are fundamental to understanding and managing these conditions. These distinctions influence the severity of symptoms, the urgency of medical intervention, and the most effective treatment strategies. By recognizing these differences, healthcare professionals and individuals in recovery can better navigate the challenges of withdrawal and work toward sustainable recovery.
Mastering Alcohol Ink Sealing: Tips for Durable, Vibrant Art Projects
You may want to see also
Explore related products






![]()
Severity Factors: Alcohol withdrawal can be life-threatening (seizures, delirium tremens)
While alcohol and opiate withdrawal share some similarities, such as anxiety, insomnia, and gastrointestinal distress, alcohol withdrawal stands out for its potential severity and life-threatening complications. The most critical factors contributing to the severity of alcohol withdrawal are the risk of seizures and delirium tremens (DTs), which are far less common in opiate withdrawal. These complications arise due to the central nervous system's adaptation to chronic alcohol exposure and its abrupt cessation.
Seizures are a significant severity factor in alcohol withdrawal, typically occurring within 6 to 48 hours after the last drink. Prolonged alcohol use alters the brain's GABA and glutamate systems, leading to hyperexcitability. When alcohol is removed, the imbalance can trigger seizures, which may range from single episodes to recurrent seizures. Unlike opiate withdrawal, which rarely causes seizures, alcohol-related seizures require immediate medical attention, as they can progress to more severe complications like delirium tremens.
Delirium tremens (DTs) is the most severe and life-threatening complication of alcohol withdrawal, occurring in approximately 5% of cases. DTs typically manifest 48 to 96 hours after the last drink and are characterized by sudden and severe confusion, hallucinations, fever, hypertension, and tachycardia. The mortality rate of untreated DTs can be as high as 37%, making it a medical emergency. Opiate withdrawal, in contrast, does not present with DTs, further highlighting the unique dangers of alcohol cessation.
Several factors increase the likelihood of severe alcohol withdrawal, including the duration and amount of alcohol consumption, prior episodes of withdrawal, and the presence of co-occurring medical or psychiatric conditions. Chronic, heavy drinkers are at the highest risk, as their bodies have become profoundly dependent on alcohol to maintain equilibrium. Additionally, individuals with a history of seizures or DTs during previous withdrawal episodes are more likely to experience these complications again, underscoring the need for supervised detoxification.
In summary, while both alcohol and opiate withdrawal involve significant discomfort, alcohol withdrawal is uniquely dangerous due to the risk of seizures and delirium tremens. These complications demand immediate medical intervention, often requiring hospitalization and medications like benzodiazepines to manage symptoms and prevent fatal outcomes. Understanding these severity factors is crucial for distinguishing between the two withdrawal syndromes and ensuring appropriate care for those at risk.
Driving Under the Influence: Legal Alcohol Limits
You may want to see also
Explore related products






![]()
Treatment Approaches: Medications like benzodiazepines for alcohol, methadone or buprenorphine for opiates
While alcohol and opiate withdrawal share some similarities, such as anxiety, insomnia, and gastrointestinal distress, they are distinct processes requiring tailored treatment approaches. This is particularly evident in the use of medications, where benzodiazepines are often employed for alcohol withdrawal, while methadone and buprenorphine are mainstay treatments for opiate withdrawal.
Benzodiazepines for Alcohol Withdrawal:
Benzodiazepines, such as diazepam and lorazepam, are the cornerstone of alcohol withdrawal management. They act on the GABA receptors in the brain, counteracting the excitatory effects of alcohol withdrawal. These medications effectively prevent and treat seizures, delirium tremens (DTs), and severe anxiety associated with alcohol withdrawal. The dosage and duration of benzodiazepine treatment are carefully titrated based on the severity of withdrawal symptoms, with longer-acting agents often preferred for their smoother tapering process.
Methadone and Buprenorphine for Opiate Withdrawal:
Methadone and buprenorphine are opioid agonists used in medication-assisted treatment (MAT) for opiate addiction. Methadone, a full opioid agonist, activates the same receptors as heroin or prescription painkillers, but at a slower and more controlled rate, preventing withdrawal symptoms and cravings. Buprenorphine, a partial opioid agonist, also binds to these receptors but with less intensity, offering a safer profile with lower risk of overdose. Both medications are administered under strict medical supervision, often in specialized clinics, and are combined with counseling and behavioral therapies for comprehensive treatment.
Differences in Treatment Approach:
The choice of medication for alcohol versus opiate withdrawal is based on the distinct neurochemical mechanisms involved. Alcohol withdrawal involves GABA and glutamate systems, while opiate withdrawal primarily affects the mu-opioid receptor system. Benzodiazepines target GABA receptors, whereas methadone and buprenorphine act on opioid receptors. Additionally, the risk profiles differ, with benzodiazepines carrying a risk of dependence and respiratory depression, particularly in those with pre-existing respiratory conditions. Methadone and buprenorphine, while effective, require careful monitoring due to their potential for misuse and overdose, especially when combined with other central nervous system depressants.
Integrated Treatment Considerations:
It is crucial to recognize that individuals may struggle with both alcohol and opiate use disorders, necessitating an integrated treatment approach. In such cases, careful coordination is required to manage potential drug interactions and overlapping withdrawal symptoms. For instance, benzodiazepines should be used cautiously in patients on methadone or buprenorphine due to the additive sedative effects. Clinicians must conduct thorough assessments, including medical history, substance use patterns, and psychiatric comorbidities, to tailor treatment plans that address both conditions effectively.
Long-term Management and Support:
Medication is just one component of a comprehensive treatment strategy for alcohol and opiate use disorders. Behavioral therapies, such as cognitive-behavioral therapy (CBT) and contingency management, play a vital role in helping individuals develop coping skills, address underlying issues, and maintain long-term recovery. Support groups, such as Alcoholics Anonymous (AA) and Narcotics Anonymous (NA), provide peer support and a sense of community, which are essential for sustained abstinence. Regular monitoring, medication adjustments, and ongoing support are critical to managing both alcohol and opiate withdrawal and promoting lasting recovery.
US States With the Highest Legal BAC Limits
You may want to see also
Explore related products






![]()
Psychological Impact: Both cause depression, anxiety, and cravings, but intensity varies
The psychological impact of alcohol and opiate withdrawal shares striking similarities, particularly in the manifestation of depression, anxiety, and cravings. Both substances alter brain chemistry over time, leading to dependence, and when discontinued, the brain struggles to regain balance. Depression is a common symptom in both withdrawal processes, as the absence of the substance disrupts neurotransmitters like dopamine and serotonin, which regulate mood. However, the intensity of depression can differ; opiate withdrawal often induces a more profound and immediate dysphoria due to the rapid rebound of the brain’s opioid receptors, whereas alcohol withdrawal may result in a more prolonged and insidious depressive state, especially in long-term users.
Anxiety is another shared psychological symptom, though its presentation varies between the two withdrawals. In alcohol withdrawal, anxiety often peaks during the acute phase, accompanied by physical symptoms like tremors and palpitations, which can exacerbate psychological distress. Opiate withdrawal, on the other hand, typically features a more generalized and persistent anxiety, often described as restlessness or agitation, which is closely tied to the body’s physical discomfort. The intensity of anxiety in opiate withdrawal may be more pronounced initially but tends to subside faster than in alcohol withdrawal, where psychological anxiety can linger for weeks or months.
Cravings are a central psychological challenge in both withdrawal processes, but their nature and intensity differ. Alcohol cravings often stem from both physical dependence and psychological associations, such as using alcohol to cope with stress or social situations. These cravings can be triggered by environmental cues and may persist long after physical withdrawal symptoms have subsided. Opiate cravings, however, are typically more intense and immediate due to the powerful hold opiates have on the brain’s reward system. The urgency and compulsive nature of opiate cravings can make them particularly challenging to manage, often requiring medication-assisted treatment to alleviate their severity.
The variability in intensity of these psychological symptoms can be attributed to factors such as the duration and severity of substance use, individual differences in brain chemistry, and the presence of co-occurring mental health disorders. For instance, individuals with pre-existing anxiety or depression may experience more severe psychological symptoms during withdrawal. Additionally, the social and environmental context plays a role; alcohol withdrawal may be more psychologically taxing for those deeply embedded in drinking cultures, while opiate withdrawal can be more isolating due to the stigma surrounding opioid use.
Understanding these psychological impacts is crucial for developing effective treatment strategies. While both withdrawals require comprehensive care, the approach may differ based on the intensity and nature of symptoms. For alcohol withdrawal, therapies like cognitive-behavioral therapy (CBT) and support groups can address cravings and depression, while medication may be necessary to manage anxiety. Opiate withdrawal often benefits from a combination of medication-assisted treatment (e.g., methadone or buprenorphine) to reduce cravings and psychological distress, alongside counseling to address underlying issues. Tailoring treatment to the specific psychological challenges of each withdrawal process improves outcomes and supports long-term recovery.
Coping with an Alcoholic Parent: Managing Your Emotions
You may want to see also
Frequently asked questions
While there are some overlapping symptoms, such as anxiety, insomnia, and nausea, the specific symptoms differ. Opiate withdrawal often includes muscle aches, diarrhea, and intense cravings, while alcohol withdrawal can lead to tremors, seizures, and delirium tremens (DTs).
No, the timelines vary. Opiate withdrawal typically begins within 6-12 hours after the last dose, peaks in 24-48 hours, and lasts 5-7 days. Alcohol withdrawal starts 6-24 hours after the last drink, peaks in 24-72 hours, and can last up to a week or more, with DTs occurring 48-72 hours after the last drink.
Both can be dangerous, but alcohol withdrawal is generally considered more life-threatening due to the risk of seizures and DTs. Opiate withdrawal is extremely uncomfortable but rarely fatal without underlying health conditions.
Treatment approaches differ. Alcohol withdrawal often requires medical supervision, medications like benzodiazepines, and hydration. Opiate withdrawal is managed with medications like methadone, buprenorphine, or naltrexone, along with supportive care and therapy.
Yes, individuals who use both substances can experience withdrawal from both simultaneously. This can complicate symptoms and increase health risks, making professional medical supervision essential for safe detoxification.