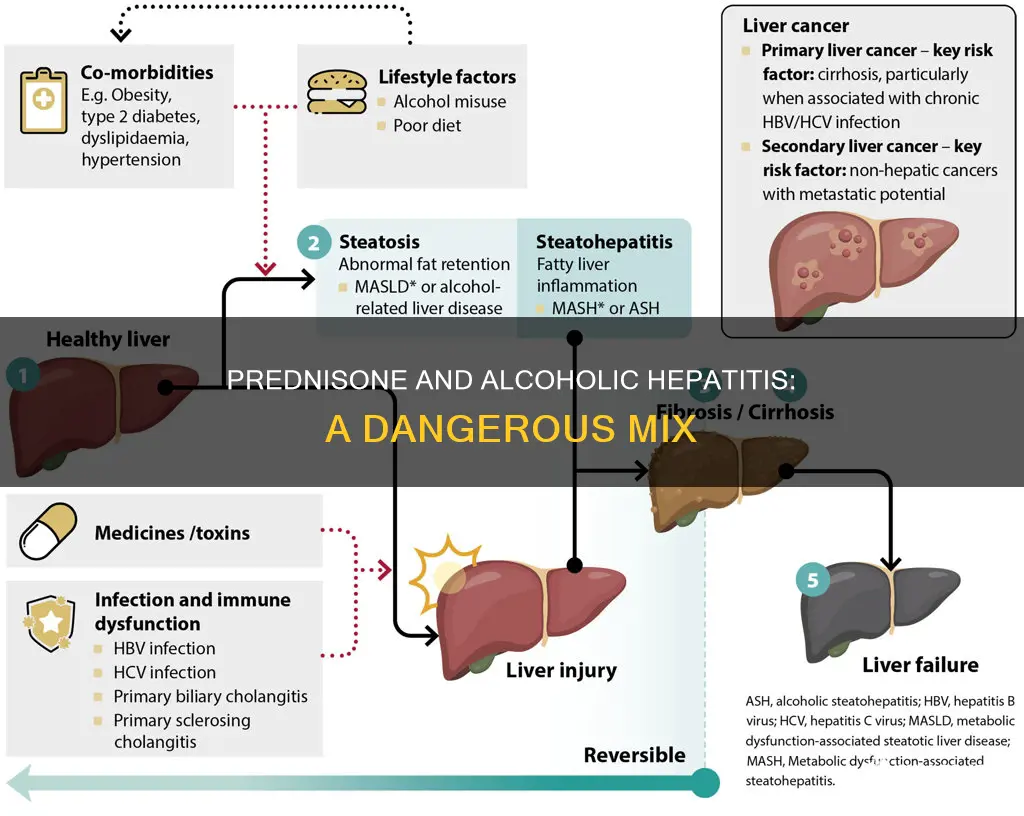
Alcoholic hepatitis is a clinical syndrome characterized by jaundice and liver impairment that occurs in patients with a history of heavy and prolonged alcohol use. The short-term mortality rate for severe alcoholic hepatitis is high, estimated to be between 30% and 50%. While corticosteroids are the recommended pharmaceutical therapy for severe alcoholic hepatitis, there is controversy over the relationship between corticosteroids, liver function, infection, and mortality. Prednisolone, a type of corticosteroid, has been found to increase the risk of serious infections and appears to increase the risk of infection even after treatment has ended. Prednisone, another type of corticosteroid, is not given for alcoholic hepatitis because it requires conversion within the liver to its active form, prednisolone, and serum prednisolone levels are higher after the administration of prednisolone compared to prednisone in patients with liver dysfunction.
Explore related products






What You'll Learn
- Prednisolone is preferred over prednisone as it doesn't require hepatic metabolism
- Corticosteroids are the only recommended pharmaceutical therapy for severe alcoholic hepatitis
- Prednisolone may reduce 28-day mortality but shows no improvement at 90 days or 1 year
- Pentoxifylline has not improved survival rates in patients with alcoholic hepatitis
- Infliximab has shown promise in small pilot studies, but larger trials are needed
![]()
Prednisolone is preferred over prednisone as it doesn't require hepatic metabolism
Alcoholic hepatitis is a clinical syndrome characterised by jaundice and liver impairment that occurs in patients with a history of heavy and prolonged alcohol use. The short-term mortality rate among patients with severe disease is over 30%.
Prednisolone is a synthetic glucocorticoid that exerts anti-inflammatory and immunosuppressive effects by modulating immune activity and reducing inflammation. It is the active metabolite of prednisone, which is also a synthetic glucocorticoid. Prednisone is converted into prednisolone in the liver.
Prednisolone and pentoxifylline are both recommended for the treatment of severe alcoholic hepatitis. In a multicentre, double-blind, randomised trial, patients with a clinical diagnosis of alcoholic hepatitis and severe disease were randomly assigned to one of four groups: a group that received a pentoxifylline-matched placebo and a prednisolone-matched placebo, a group that received prednisolone and a pentoxifylline-matched placebo, a group that received pentoxifylline and a prednisolone-matched placebo, and a group that received both prednisolone and pentoxifylline. The primary endpoint was mortality at 28 days. The results showed that prednisolone was associated with a short-term reduction in mortality, with a 28-day mortality rate of 20% among those treated with prednisolone compared to 34% among those who received a placebo.
Prednisolone is preferred over prednisone for the treatment of alcoholic hepatitis because it does not require hepatic metabolism. While prednisone is converted into prednisolone in the liver, prednisolone is already in its active form and does not need to be metabolised by the liver. This is particularly important in patients with alcoholic hepatitis, who may have liver impairment. By avoiding hepatic metabolism, prednisolone can exert its therapeutic effects without further burdening the liver.
Additionally, prednisolone may be safer for patients with hepatic impairment due to the altered pharmacokinetics of prednisone in these individuals. In patients with cirrhosis, corticosteroid biotransformation is decreased, leading to increased half-life and bioavailability of prednisone. This can result in higher and more prolonged exposure to the drug, potentially increasing the risk of adverse effects. By bypassing hepatic metabolism, prednisolone may offer a more predictable and controlled therapeutic effect in patients with compromised liver function.
Acetone vs Methyl Alcohol: Boiling Point Mystery Solved!
You may want to see also
Explore related products





![]()
Corticosteroids are the only recommended pharmaceutical therapy for severe alcoholic hepatitis
Alcoholic hepatitis is a clinical syndrome characterised by jaundice and liver impairment that occurs in patients with a history of heavy and prolonged alcohol use. The short-term mortality rate among patients with severe disease is over 30%. The condition is conventionally defined by Maddrey's discriminant function, with a value of 32 or higher indicating severe alcoholic hepatitis.
Several studies have been conducted to evaluate the efficacy of corticosteroids in treating alcoholic hepatitis. A meta-analysis of 11 randomised controlled trials found that corticosteroid treatment significantly decreased the risk of death within 28 days compared to controls or pentoxifylline. Another study showed that prednisolone was associated with a short-term reduction in mortality, but this benefit was not apparent after two years.
Other treatments for alcoholic hepatitis have been investigated, including pentoxifylline, infliximab, anabolic steroids, insulin and glucagon, and vitamin E. However, none of these have shown significant benefits in reducing mortality or improving liver function.
In conclusion, while corticosteroids are the only recommended pharmaceutical therapy for severe alcoholic hepatitis, their use is associated with risks and the lack of long-term benefits highlights the need for new therapeutic strategies.
The Many Forms of C4H10O
You may want to see also
Explore related products






![]()
Prednisolone may reduce 28-day mortality but shows no improvement at 90 days or 1 year
Alcoholic hepatitis (AH) is a clinical syndrome that presents with jaundice and liver failure in patients with a history of prolonged and heavy alcohol use. The condition is associated with high mortality, with short-term mortality exceeding 30%.
Prednisolone and pentoxifylline are recommended for the treatment of severe alcoholic hepatitis, but there is uncertainty about their effectiveness. Prednisolone decreases autoimmune reactions by suppressing components of the immune system, and it does not need to undergo hepatic metabolism, which may make it preferable to other glucocorticoids like prednisone.
The STOPAH trial, a UK multi-centre, double-blind, randomised trial, investigated the effect of prednisolone and/or pentoxifylline on mortality in patients with severe AH. The trial found that while prednisolone was associated with a reduction in 28-day mortality, this reduction did not reach statistical significance, and there was no improvement in outcomes at 90 days or 1 year.
The results of the STOPAH trial suggest that the administration of 40 mg of prednisolone daily for 1 month may have a beneficial effect on short-term mortality but does not impact medium or long-term outcomes in patients with alcoholic hepatitis. Serious infections occurred in 13% of patients treated with prednisolone, compared to 7% in those who did not receive it.
While prednisolone may offer a potential benefit in reducing short-term mortality, the lack of improvement beyond 28 days and the increased risk of infection are important considerations in the treatment of alcoholic hepatitis. Further well-designed controlled trials are necessary to resolve the controversy and determine the most effective approaches to managing this challenging condition.
Quick Tips: Sober Up from Alcohol Before Bed
You may want to see also
Explore related products






![]()
Pentoxifylline has not improved survival rates in patients with alcoholic hepatitis
Alcoholic hepatitis is a clinical syndrome characterised by jaundice and liver impairment that occurs in patients with a history of heavy and prolonged alcohol use. The short-term mortality rate among patients with severe disease is over 30%, with a 28-day mortality rate of approximately 35%. Several treatments have been evaluated, but only two drugs, prednisolone and pentoxifylline, are recommended for severe alcoholic hepatitis. However, uncertainty about their benefits persists.
Pentoxifylline is an inhibitor of tumour necrosis factor (TNF) synthesis, which has been found to be elevated in patients with acute alcoholic hepatitis. It is also believed to act by inhibiting the synthesis of the pro-inflammatory cytokine tumour necrosis factor alpha (TNF-α) and improving renal function in patients with hepatorenal syndrome.
Several studies have been conducted to evaluate the effectiveness of pentoxifylline in treating alcoholic hepatitis. One early pilot study suggested that pentoxifylline improved short-term survival in patients with severe acute alcoholic hepatitis. This study was a double-blind, placebo-controlled trial involving 101 patients, where 49 received pentoxifylline and 52 received a placebo. The results showed a lower mortality rate in the pentoxifylline group (24.5%) compared to the placebo group (46.1%).
However, subsequent larger studies and meta-analyses have failed to demonstrate a significant benefit of pentoxifylline on survival rates in patients with alcoholic hepatitis. One randomised controlled trial, the COPE trial, specifically evaluated the combination of corticosteroids and pentoxifylline and found that this combination was not better than corticosteroids alone for improving survival. Another randomised controlled trial involving 1,200 patients with severe alcoholic hepatitis, the STOPAH trial, also found no improvement in short-term survival with pentoxifylline.
In conclusion, while early pilot studies suggested that pentoxifylline may improve short-term survival in patients with severe acute alcoholic hepatitis, larger and more robust studies have failed to confirm these findings. Therefore, it cannot be concluded that pentoxifylline improves survival rates in patients with alcoholic hepatitis. Further well-designed controlled clinical trials are necessary to resolve the controversy and establish the efficacy of different treatments for this condition.
Alcohol Calorie Count: Gram-Wise Breakdown
You may want to see also
Explore related products






![]()
Infliximab has shown promise in small pilot studies, but larger trials are needed
Alcoholic hepatitis (AH) is a clinical syndrome with high mortality that develops in people with a history of prolonged and heavy alcohol use. It is often described as alcohol-related cholestatic liver failure, and is characterised by jaundice and liver failure. Corticosteroids are the only recommended pharmaceutical therapy for severe alcoholic hepatitis. Prednisolone, a type of corticosteroid, is often recommended for the treatment of severe alcoholic hepatitis, but uncertainty about its benefits persists.
Infliximab, a chimeric monoclonal antibody directed against tumor necrosis factor-alpha (TNF-alpha), has been used successfully in immunologically mediated inflammatory diseases, such as Crohn's disease and rheumatoid arthritis. It has also been proven to be effective in the treatment of granulomatous diseases, including sarcoidosis.
In two small pilot studies on subjects with alcoholic hepatitis, infliximab improved MDF scores, serum bilirubin and C-reactive protein (CRP) levels, and patient survival. However, a subsequent randomised, double-blind, controlled trial of 36 subjects with severe alcoholic hepatitis failed to confirm these findings. The trial was discontinued due to the high rate of infections and mortality in the infliximab group.
While infliximab has shown promise in small pilot studies, larger trials are needed to confirm its efficacy and safety in the treatment of alcoholic hepatitis. The NOR-DRUM study, for example, is a randomised, controlled, parallel-group, phase IV study that aims to assess the effectiveness of therapeutic drug monitoring (TDM) in patients receiving infliximab for a range of immune-mediated inflammatory diseases.
Alcohol in Moderation: Longevity's Elixir?
You may want to see also
Frequently asked questions
Prednisone is a glucocorticoid that requires hepatic metabolism, which is why it is not recommended for alcoholic hepatitis. Instead, prednisolone is preferred as it does not require hepatic metabolism and can suppress key components of the immune system.
Alcoholic hepatitis is a clinical syndrome with high mortality, and the recommended treatment includes alcohol withdrawal, bed rest, and a high-calorie and protein-restricted diet. Corticosteroids are the only recommended pharmaceutical therapy for severe alcoholic hepatitis.
Alcoholic hepatitis is characterised by jaundice, ascites, liver failure, hepatomegaly, abdominal tenderness, fever, anorexia, nausea, and vomiting.































