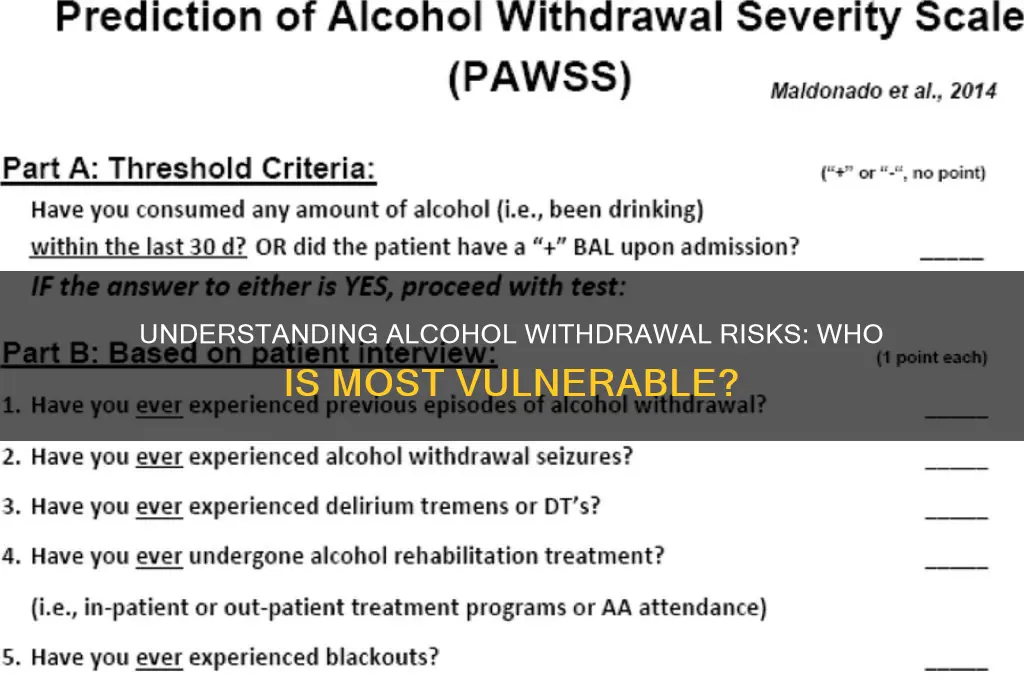
Alcohol withdrawal is a serious and potentially life-threatening condition that occurs when individuals who have been drinking heavily for weeks, months, or years suddenly stop or significantly reduce their alcohol intake. Those at highest risk for alcohol withdrawal include chronic heavy drinkers, individuals with a history of alcohol dependence, and people who have previously experienced withdrawal symptoms. Additional risk factors include concurrent medical conditions, older age, and a higher level of alcohol consumption. It is crucial for healthcare providers to identify and monitor these at-risk individuals, as prompt recognition and management of withdrawal symptoms can prevent severe complications such as seizures, delirium tremens, and even death.
Explore related products


$12.68 $24.95




What You'll Learn
![]()
Heavy drinkers with long-term alcohol use history
Heavy drinkers with a long-term alcohol use history face a heightened risk of severe alcohol withdrawal symptoms, a condition that demands careful attention and management. These individuals, often defined as consuming more than 15 drinks per week for men or 8 drinks per week for women over several years, have adapted their bodies to the constant presence of alcohol. When they abruptly stop or significantly reduce intake, their central nervous system, which has been suppressed by alcohol, becomes hyperactive, leading to withdrawal. This physiological rebound can manifest within hours to days after the last drink, with symptoms ranging from mild anxiety and tremors to life-threatening seizures or delirium tremens (DTs). Understanding this risk is the first step in addressing the unique challenges faced by this group.
Consider the case of a 45-year-old man who has been drinking a 12-pack of beer daily for two decades. His body has developed a tolerance, requiring increasing amounts to achieve the same effect. If he suddenly quits, his brain, now dependent on alcohol to maintain equilibrium, will struggle to function without it. Within 6–24 hours, he may experience shaking, sweating, and nausea. By 48–72 hours, he could face hallucinations or seizures. Without medical intervention, the risk of DTs—characterized by confusion, fever, and agitation—peaks around 48–96 hours, with a mortality rate of up to 15% if untreated. This example underscores the critical need for supervised detoxification for long-term heavy drinkers.
For those in this category, tapering alcohol intake under medical guidance is often safer than quitting cold turkey. A structured reduction plan, overseen by a healthcare professional, can minimize withdrawal risks. For instance, a patient might start by cutting daily consumption by 10–20%, gradually decreasing over weeks or months. Medications like benzodiazepines (e.g., diazepam or lorazepam) are frequently used to manage withdrawal symptoms, as they act on the same brain receptors as alcohol, preventing overactivity. However, self-tapering without medical advice is risky, as it requires precise dosing and monitoring to avoid complications.
Practical tips for heavy drinkers seeking to reduce their risk include keeping a drinking diary to track consumption, setting realistic reduction goals, and seeking support from friends, family, or support groups like Alcoholics Anonymous. Nutritional support is also vital, as long-term alcohol use often leads to deficiencies in thiamine, magnesium, and other essential nutrients, which can exacerbate withdrawal symptoms. Rehydration and a balanced diet can aid the body’s recovery during detoxification.
In conclusion, heavy drinkers with a long-term alcohol use history are a distinct at-risk group for severe withdrawal. Their prolonged exposure to alcohol creates a physiological dependence that requires careful, often medical, management to safely navigate withdrawal. By understanding the risks, seeking professional guidance, and adopting practical strategies, individuals in this category can mitigate dangers and take the first steps toward recovery. Ignoring these risks can lead to dire consequences, but with the right approach, a safer path forward is possible.
Effective Interventions for Managing Alcohol Withdrawal Symptoms Safely
You may want to see also
Explore related products






![]()
Individuals with previous withdrawal symptoms or seizures
Individuals with a history of alcohol withdrawal symptoms or seizures are at significantly higher risk for severe complications during future withdrawal episodes. This group represents a critical subset of those vulnerable to alcohol withdrawal, as their bodies have already demonstrated a heightened sensitivity to the absence of alcohol. The presence of previous withdrawal symptoms, such as tremors, anxiety, or insomnia, serves as a red flag, indicating that the central nervous system has adapted to chronic alcohol exposure and struggles to function without it. Similarly, a history of seizures during withdrawal is a grave warning sign, as it suggests a severe dysregulation of brain activity that can recur with even greater intensity in subsequent episodes.
Consider the case of a 45-year-old man with a decade-long history of heavy drinking, defined as more than 15 drinks per week. After a previous attempt to quit cold turkey, he experienced severe withdrawal symptoms, including hallucinations and grand mal seizures. This individual is now at a substantially elevated risk for complications if he attempts to stop drinking again without medical supervision. His brain, having adapted to the depressant effects of alcohol, is prone to rebound excitability when alcohol is removed, increasing the likelihood of life-threatening seizures or delirium tremens (DTs), a severe form of withdrawal characterized by confusion, fever, and agitation.
For those in this high-risk category, a structured, medically supervised detoxification is essential. Tapering alcohol intake under professional guidance can reduce the risk of seizures and other severe symptoms. For example, a benzodiazepine like diazepam may be prescribed to manage withdrawal symptoms, with dosages adjusted based on the severity of previous episodes. A typical regimen might start with 10 mg every 6 hours, titrated upward as needed to control symptoms. This approach must be individualized, as factors such as age, liver function, and the duration of alcohol dependence influence the safety and efficacy of treatment.
Practical tips for individuals with a history of withdrawal complications include avoiding abrupt cessation of alcohol, maintaining open communication with healthcare providers, and having a support system in place. Family members or caregivers should be educated on the signs of severe withdrawal, such as confusion, fever, or seizures, and know when to seek emergency care. Additionally, integrating long-term treatment strategies, such as counseling, support groups, and medications like naltrexone or acamprosate, can help prevent relapse and reduce the risk of future withdrawal episodes.
In conclusion, individuals with previous withdrawal symptoms or seizures require a proactive, tailored approach to alcohol cessation. Their history serves as both a warning and a guide, highlighting the need for medical intervention and long-term support. By recognizing the unique risks this group faces and implementing evidence-based strategies, healthcare providers and individuals alike can mitigate the dangers of alcohol withdrawal and pave the way for sustained recovery.
Weed vs. Alcohol: Which Burns More Brain Cells?
You may want to see also
Explore related products

$29.99 $29.99

$34 $72




![]()
People with co-occurring mental health disorders
Individuals with co-occurring mental health disorders face a heightened risk of severe alcohol withdrawal due to the complex interplay between their conditions and alcohol dependence. This population often uses alcohol as a form of self-medication to alleviate symptoms of anxiety, depression, or trauma, creating a dangerous cycle of dependency. For example, someone with generalized anxiety disorder might consume alcohol daily to manage persistent worry, only to find themselves physically and psychologically reliant on it over time. The presence of mental health disorders not only increases the likelihood of alcohol misuse but also complicates the withdrawal process, as both conditions exacerbate each other’s symptoms.
Consider the case of a 32-year-old with bipolar disorder who has been drinking heavily to stabilize mood swings. When attempting to quit alcohol, they may experience intensified anxiety, insomnia, or even manic episodes, making withdrawal more challenging. Research shows that individuals with co-occurring disorders are 2–4 times more likely to experience severe withdrawal symptoms, such as seizures or delirium tremens, compared to those without mental health conditions. This heightened risk underscores the need for tailored withdrawal management that addresses both alcohol dependence and underlying psychiatric issues simultaneously.
A critical step in managing alcohol withdrawal for this population is integrating dual diagnosis treatment. This approach involves a combination of medication, psychotherapy, and support groups. For instance, benzodiazepines may be prescribed to manage withdrawal symptoms, but dosages must be carefully monitored to avoid interactions with psychiatric medications. Cognitive-behavioral therapy (CBT) can help individuals develop coping strategies for both mental health symptoms and alcohol cravings. Practical tips include maintaining a consistent sleep schedule, engaging in mindfulness practices, and avoiding triggers like social settings where alcohol is present.
However, caution is necessary when treating this group. Abrupt cessation of alcohol without medical supervision can be life-threatening, particularly for those with conditions like schizophrenia or severe depression, where withdrawal may exacerbate psychosis or suicidal ideation. A gradual tapering approach, overseen by a healthcare professional, is often safer. Additionally, family members or caregivers should be educated on recognizing warning signs of severe withdrawal, such as confusion, fever, or seizures, and know when to seek emergency care.
In conclusion, addressing alcohol withdrawal in individuals with co-occurring mental health disorders requires a nuanced, multidisciplinary strategy. By acknowledging the unique challenges this population faces and implementing evidence-based interventions, healthcare providers can improve outcomes and reduce the risk of relapse. The goal is not just to manage withdrawal but to foster long-term recovery that addresses both addiction and mental health holistically.
Does Certo Detox Really Work for Alcohol? Facts and Myths Explained
You may want to see also
Explore related products






![]()
Those with physical dependence on alcohol
Physical dependence on alcohol is a critical factor in determining who is at risk for alcohol withdrawal. This condition develops when the body adapts to the constant presence of alcohol, requiring increasingly higher amounts to achieve the same effect. For individuals consuming more than four standard drinks per day for men, or three for women, over an extended period, the risk of physical dependence escalates significantly. Once dependent, abruptly reducing or stopping alcohol intake triggers withdrawal symptoms, ranging from mild anxiety to life-threatening seizures.
Consider the progression of physical dependence as a series of stages. Initially, tolerance builds, where the body requires more alcohol to feel its effects. Next, withdrawal symptoms emerge during periods of abstinence, signaling the body’s reliance on alcohol to function. For example, someone who consumes six beers daily for a year may experience tremors, nausea, or insomnia within 6–24 hours of their last drink. These symptoms are the body’s response to the absence of alcohol, which it now mistakenly perceives as essential for maintaining equilibrium.
To mitigate risks, individuals with physical dependence must approach alcohol cessation strategically. Tapering off alcohol under medical supervision is often safer than quitting cold turkey. For instance, reducing daily intake by one standard drink every 48 hours can minimize withdrawal severity. However, this method requires discipline and monitoring, as even slight deviations can lead to rebound symptoms. Medications like benzodiazepines, prescribed by a healthcare provider, can manage withdrawal symptoms by calming the nervous system, but self-medication is strongly discouraged due to the risk of additional dependencies.
Comparatively, those without physical dependence may experience discomfort but rarely face life-threatening complications when stopping alcohol. In contrast, dependent individuals are at heightened risk for severe withdrawal syndromes like delirium tremens (DTs), which occur in 3–5% of cases and include hallucinations, fever, and seizures. Age and overall health further influence risk; older adults or those with pre-existing conditions like liver disease are more vulnerable. Recognizing these distinctions underscores the need for tailored interventions for those with physical dependence.
Practically, anyone suspecting physical dependence should seek professional assessment. Tools like the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) help gauge withdrawal severity, guiding treatment decisions. Support systems, including therapy and peer groups, play a vital role in long-term recovery. For instance, cognitive-behavioral therapy can address underlying triggers for alcohol use, while programs like Alcoholics Anonymous provide community-based accountability. By combining medical oversight with behavioral strategies, individuals can navigate withdrawal safely and reduce the likelihood of relapse.
From Alkanes to Alcohols: Understanding the Formation Process
You may want to see also
Explore related products





![]()
Patients with liver disease or malnutrition
Liver disease and malnutrition form a dangerous alliance that significantly heightens the risk and severity of alcohol withdrawal. The liver, our body's detox powerhouse, breaks down alcohol into less harmful substances. Chronic alcohol abuse, however, scars and inflames the liver, leading to conditions like fatty liver disease, cirrhosis, and hepatitis. A compromised liver struggles to metabolize alcohol efficiently, leaving toxic byproducts to accumulate. This buildup intensifies withdrawal symptoms, making them more severe and potentially life-threatening.
Imagine a clogged drain – water backs up, causing overflow. Similarly, a damaged liver allows alcohol's toxins to "overflow," exacerbating withdrawal's physical and neurological toll.
Malnutrition, often a companion to chronic alcohol use, further fuels this fire. Alcohol interferes with nutrient absorption and utilization, leading to deficiencies in vitamins (especially thiamine, B12, and folate) and minerals like magnesium and potassium. These deficiencies weaken the body's ability to cope with stress, including the stress of withdrawal. Think of it as trying to fight a battle with a depleted arsenal – the body lacks the essential tools to manage the physiological upheaval of withdrawal.
For instance, thiamine deficiency can lead to Wernicke-Korsakoff syndrome, a neurological disorder characterized by confusion, memory loss, and coordination problems, which can be triggered or worsened during withdrawal.
The combination of liver disease and malnutrition creates a perfect storm for severe withdrawal. Symptoms like tremors, anxiety, seizures, and delirium tremens (DTs) become more pronounced and harder to manage. Individuals with these conditions require close medical supervision during withdrawal. Treatment often involves a multi-pronged approach: gradual alcohol tapering under medical guidance, nutritional support through intravenous fluids and supplements, and medications to manage specific symptoms like benzodiazepines for anxiety and seizures.
Early intervention is crucial. Recognizing the signs of liver disease (fatigue, jaundice, abdominal swelling) and malnutrition (weight loss, muscle wasting, weakened immunity) in individuals with alcohol use disorder is vital for preventing complications during withdrawal.
Remember, this is not a journey to be undertaken alone. Seeking professional help from healthcare providers experienced in addiction medicine is essential for safe and effective management of alcohol withdrawal, especially in individuals with liver disease or malnutrition.
Does Corona Beer Contain Alcohol? Unraveling the Truth Behind the Myth
You may want to see also
Frequently asked questions
Individuals who consume alcohol heavily or regularly over an extended period are at risk for alcohol withdrawal. This includes those with alcohol use disorder (AUD) or those who abruptly reduce or stop drinking after prolonged use.
Occasional or moderate drinkers are less likely to experience alcohol withdrawal. Withdrawal typically occurs in individuals who have developed physical dependence due to chronic, heavy alcohol consumption.
Yes, individuals with a history of severe alcohol dependence, prior withdrawal seizures, or co-occurring medical or psychiatric conditions are at higher risk. Older adults and those with poor overall health may also be more vulnerable.
Yes, the risk of alcohol withdrawal increases with the amount and frequency of alcohol consumption. Heavy drinking, defined as 15 drinks or more per week for men and 8 drinks or more per week for women, significantly raises the risk.































