The term Fetal Alcohol Syndrome (Fetal Alcohol Syndrome) was first introduced in 1973 by Dr. Paul Lemoine, a French pediatrician, and his colleagues. They published a study describing a pattern of birth defects, including distinctive facial features, growth deficiencies, and cognitive impairments, in children born to mothers who consumed alcohol during pregnancy. This groundbreaking research shed light on the harmful effects of prenatal alcohol exposure, leading to increased awareness and further investigations into the condition. The identification of Fetal Alcohol Syndrome marked a significant milestone in understanding the impact of maternal alcohol use on fetal development, paving the way for improved prevention strategies, diagnostic criteria, and support for affected individuals and their families.
| Characteristics | Values |
|---|---|
| Term Introduction | The term "Fetal Alcohol Syndrome" (FAS) was first introduced in 1973. |
| Researchers | Dr. Paul Lemoine and colleagues in France initially described the condition, but it gained widespread recognition after Dr. Kenneth Jones and Dr. David W. Smith in the United States published their findings in 1973. |
| Initial Publication | The term was formally introduced in the The Lancet journal in 1973. |
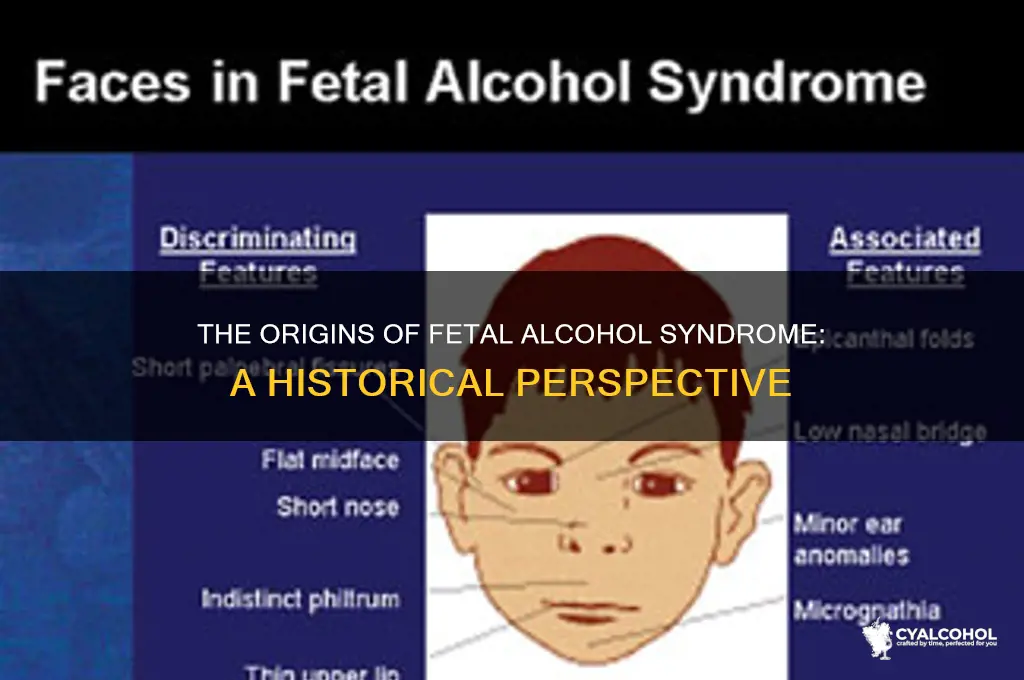
| Key Characteristics Identified | Growth deficiency, facial abnormalities (e.g., smooth philtrum, thin upper lip, small palpebral fissures), and central nervous system dysfunction. |
| Context | The term was coined after observing consistent patterns of congenital anomalies in children born to mothers who consumed alcohol during pregnancy. |
| Impact | The introduction of the term led to increased awareness of the risks of prenatal alcohol exposure and the development of diagnostic criteria for FAS. |
Explore related products






What You'll Learn
![]()
Historical Context of FAS Diagnosis
The term "Fetal Alcohol Syndrome" (FAS) was first introduced in the medical literature in 1973 by Dr. Paul Lemestre and his colleagues at the University of Washington. Their groundbreaking research identified a pattern of birth defects and developmental issues in children born to mothers who consumed alcohol during pregnancy. This discovery marked the beginning of a new era in understanding the impact of maternal alcohol use on fetal development. Prior to this, while there were anecdotal reports and suspicions about the harmful effects of alcohol on pregnancy, there was no formal medical recognition or diagnostic criteria for the condition. The introduction of the term FAS provided a framework for clinicians to identify and address the specific consequences of prenatal alcohol exposure.
The historical context of FAS diagnosis is deeply rooted in the evolving understanding of teratogens—substances that can cause developmental malformations in a fetus. In the mid-20th century, the thalidomide tragedy of the 1950s and 1960s heightened awareness of the potential dangers of maternal exposure to certain substances during pregnancy. This tragedy, which resulted in thousands of children born with severe limb deformities, spurred research into other possible teratogens, including alcohol. By the late 1960s, animal studies had begun to demonstrate the harmful effects of alcohol on fetal development, laying the groundwork for human studies that would eventually lead to the identification of FAS.
The initial description of FAS by Lemestre and his team focused on a cluster of physical abnormalities, including facial dysmorphology (such as a smooth philtrum, thin upper lip, and small palpebral fissures), growth deficiencies, and central nervous system dysfunction. These findings were based on observations of eight children whose mothers had consumed significant amounts of alcohol during pregnancy. The publication of this research in *The Lancet* in 1973 brought international attention to the issue and prompted further investigation into the prevalence and long-term effects of prenatal alcohol exposure. This early work established the foundation for diagnostic criteria that would be refined in subsequent decades.
Throughout the 1980s and 1990s, research on FAS expanded to include a broader understanding of the spectrum of disorders caused by prenatal alcohol exposure, now collectively referred to as Fetal Alcohol Spectrum Disorders (FASD). Scientists and clinicians began to recognize that not all affected individuals exhibited the full range of FAS characteristics, leading to the identification of related conditions such as partial fetal alcohol syndrome (pFAS) and alcohol-related neurodevelopmental disorder (ARND). This period also saw increased efforts to develop standardized diagnostic guidelines, culminating in the publication of criteria by the Institute of Medicine in 1996. These guidelines emphasized the importance of confirming maternal alcohol use, identifying characteristic facial features, assessing growth deficits, and evaluating neurodevelopmental impairments.
The historical context of FAS diagnosis reflects broader societal shifts in attitudes toward alcohol use during pregnancy and the responsibilities of public health systems. Initially, there was resistance and stigma surrounding the idea that maternal behavior could directly harm fetal development. However, as evidence mounted, public health campaigns began to educate women about the risks of drinking during pregnancy. The introduction and evolution of the FAS diagnosis have played a critical role in shaping policies, prevention strategies, and support services for affected individuals and their families. Today, FASD is recognized as a leading preventable cause of developmental disabilities, underscoring the enduring significance of its historical origins in 1973.
FAS Babies: Beyond Alcoholic Mothers – Unraveling the Truth
You may want to see also
Explore related products


$16.18 $21.99




![]()
Dr. Paul Lemen's Role in FAS
The term Fetal Alcohol Syndrome (FAS) was officially introduced in 1973 by Dr. Kenneth Jones and his colleagues at the University of Washington School of Medicine. However, the groundwork for understanding the effects of alcohol on fetal development was laid by earlier researchers, including Dr. Paul Lemen, whose contributions were instrumental in shaping the field. Dr. Lemen, a pioneering pediatrician and dysmorphologist, played a crucial role in identifying and characterizing the physical and developmental abnormalities associated with prenatal alcohol exposure. His work in the 1960s and early 1970s provided critical insights that directly influenced the formal recognition of FAS as a distinct medical condition.
In addition to his clinical observations, Dr. Lemen collaborated with researchers and clinicians to document and analyze cases of children with similar characteristics. His work laid the foundation for the diagnostic criteria later used to define FAS. By systematically linking specific physical and developmental features to prenatal alcohol exposure, Dr. Lemen helped establish the causal relationship between maternal drinking and fetal harm. His research was pivotal in raising awareness among medical professionals and the public about the dangers of alcohol consumption during pregnancy, paving the way for the formal introduction of the term FAS in 1973.
Dr. Lemen's contributions extended beyond his scientific discoveries; he was also a vocal advocate for prevention and education. He emphasized the importance of identifying at-risk populations and implementing interventions to reduce alcohol use among pregnant women. His efforts helped shape public health policies and initiatives aimed at preventing FAS. Furthermore, Dr. Lemen's work inspired future research into the broader spectrum of fetal alcohol spectrum disorders (FASD), which encompasses a range of conditions caused by prenatal alcohol exposure. His legacy continues to influence the field, as his early insights remain fundamental to understanding and addressing the impact of alcohol on fetal development.
In summary, while Dr. Kenneth Jones and his team coined the term FAS in 1973, Dr. Paul Lemen's pioneering work was essential in uncovering the condition's origins and characteristics. His clinical observations, research collaborations, and advocacy efforts were instrumental in establishing FAS as a recognized medical diagnosis. Dr. Lemen's role in FAS highlights the importance of early investigators in advancing medical knowledge and underscores his lasting impact on the prevention and treatment of alcohol-related birth defects. His contributions remain a cornerstone in the ongoing fight against FAS and its associated disorders.
Alcohol Abuse: A Predictor of Divorce?
You may want to see also
Explore related products





![]()
First Published Description of FAS
The term "Fetal Alcohol Syndrome" (FAS) was first introduced in the medical literature in 1973 by Dr. Paul Lemoine, a French pediatrician. However, the first published description of the condition, though not yet labeled as FAS, dates back to 1968. This groundbreaking work was conducted by Dr. Paul Lemoine and his colleagues, who observed a pattern of abnormalities in children born to mothers who consumed alcohol during pregnancy. Their findings, published in a French medical journal, *Ouest-Médical*, marked the initial recognition of the deleterious effects of prenatal alcohol exposure on fetal development.
In their 1968 publication, Dr. Lemoine and his team described a group of children who presented with distinctive facial anomalies, growth deficiencies, and developmental delays. These children shared common characteristics, including a smooth philtrum (the groove between the nose and upper lip), thin upper lip, and small palpebral fissures (the openings between the eyelids). The researchers noted that these features were consistently observed in children whose mothers had a history of chronic alcohol consumption during pregnancy. This detailed clinical description laid the foundation for what would later be formally recognized as Fetal Alcohol Syndrome.
The 1968 study by Dr. Lemoine and his colleagues was pivotal because it established a clear link between maternal alcohol use and specific congenital abnormalities in offspring. While the term "Fetal Alcohol Syndrome" was not yet coined, their work highlighted the importance of prenatal alcohol exposure as a teratogen—a substance capable of causing developmental malformations. The researchers also emphasized the need for further investigation into the long-term effects of alcohol on fetal development, recognizing that the observed abnormalities were likely just the tip of the iceberg.
Following Dr. Lemoine's initial publication, the findings gained international attention, particularly after being translated and disseminated in English-language medical literature. This led to increased research and clinical awareness of the condition. By 1973, Dr. Kenneth Jones and his colleagues at the University of Washington formally introduced the term "Fetal Alcohol Syndrome" in the *Lancet* journal, building upon Dr. Lemoine's earlier work. However, it was Dr. Lemoine's 1968 publication that provided the first comprehensive description of the syndrome, making it a cornerstone in the history of FAS research.
In summary, the first published description of what would later be known as Fetal Alcohol Syndrome appeared in 1968, authored by Dr. Paul Lemoine and his team. Their meticulous documentation of facial anomalies, growth deficiencies, and developmental delays in children exposed to alcohol in utero set the stage for the formal recognition of FAS in 1973. This early work not only identified the physical and developmental consequences of prenatal alcohol exposure but also underscored the critical need for public health interventions to prevent alcohol-related harm during pregnancy.
Why No Alcohol Withdrawal Symptoms?
You may want to see also
Explore related products






![]()
Impact of 1973 Research on FAS
The introduction of the term Fetal Alcohol Syndrome (FAS) in 1973 marked a pivotal moment in medical history, significantly altering the understanding and approach to prenatal health. This groundbreaking research, published by Dr. Paul Lemestre and his colleagues, identified a pattern of congenital malformations and developmental issues in children born to mothers who consumed alcohol during pregnancy. The term "Fetal Alcohol Syndrome" was coined to describe this cluster of symptoms, which included distinctive facial anomalies, growth deficiencies, and central nervous system dysfunction. This research not only provided a clear diagnostic framework but also brought global attention to the previously underrecognized risks of prenatal alcohol exposure.
The immediate impact of the 1973 research was a surge in awareness among healthcare professionals, policymakers, and the public. For the first time, there was a medically validated term to describe the adverse effects of alcohol on fetal development. This led to the development of educational campaigns aimed at pregnant women and those planning to conceive, emphasizing the importance of abstaining from alcohol during pregnancy. Medical curricula began to incorporate FAS as a critical topic, ensuring that future generations of healthcare providers would be equipped to identify and manage the condition. The research also spurred the creation of diagnostic criteria, enabling consistent identification and documentation of FAS cases worldwide.
On a scientific level, the 1973 study catalyzed extensive research into the mechanisms by which alcohol affects fetal development. Investigators began exploring how ethanol disrupts cellular processes, impairs organogenesis, and leads to long-term neurobehavioral deficits. This deepened understanding paved the way for further studies on the spectrum of fetal alcohol spectrum disorders (FASD), recognizing that alcohol exposure could result in a range of outcomes beyond the full syndrome. Funding for FAS-related research increased, fostering collaborations across disciplines such as genetics, neuroscience, and public health to address the complexities of the condition.
The societal impact of the 1973 research was profound, influencing policy and legal frameworks related to alcohol consumption during pregnancy. Governments and health organizations issued guidelines recommending abstinence from alcohol for pregnant women, and warning labels began to appear on alcoholic beverages in many countries. Legal cases involving FAS also emerged, with some jurisdictions holding individuals accountable for harm caused by prenatal alcohol exposure. Advocacy groups formed to support affected families and push for greater resources, further embedding FAS into public consciousness and policy agendas.
Finally, the 1973 research had a lasting impact on clinical practice and intervention strategies. Healthcare providers started screening pregnant women for alcohol use more systematically, and interventions such as counseling and support programs were developed to help reduce or eliminate alcohol consumption during pregnancy. Early identification of children with FAS led to the implementation of targeted educational and therapeutic interventions to address developmental delays and behavioral challenges. The research also highlighted the need for long-term support for individuals with FAS, as the effects of the condition persist throughout the lifespan. In summary, the 1973 introduction of the term Fetal Alcohol Syndrome revolutionized the field, driving awareness, research, policy, and clinical practice in ways that continue to shape prenatal care and public health today.
Alcohol Coping: Breaking Free from the Bottle's Shackles
You may want to see also
Explore related products






![]()
FAS Recognition in Medical Literature
The term Fetal Alcohol Syndrome (FAS) was first introduced in 1973 by Dr. Paul Lemoine, a French pediatrician, who published a study describing children with distinct patterns of congenital malformations and developmental issues linked to maternal alcohol consumption. However, it was not until 1973 that the term gained significant recognition in the English-speaking medical literature. Dr. Kenneth Jones and his colleagues at the University of Washington published a landmark article in *The Lancet* titled *"Pattern of Malformation in Offspring of Chronic Alcoholic Mothers,"* which formally introduced the term Fetal Alcohol Syndrome to the international medical community. This publication marked the beginning of widespread acknowledgment of the deleterious effects of prenatal alcohol exposure on fetal development.
Following its introduction, FAS began to appear more frequently in medical literature, with researchers and clinicians working to define its diagnostic criteria. By the late 1970s and early 1980s, key features of FAS were established, including growth deficiency, facial dysmorphology (such as smooth philtrum, thin upper lip, and small palpebral fissures), and central nervous system abnormalities. These criteria were formalized in 1980 by the Institute of Medicine (IOM), which provided a standardized framework for diagnosing FAS. This standardization was crucial for consistent recognition and documentation of the syndrome in medical research and clinical practice.
Throughout the 1980s and 1990s, medical literature expanded to include not only FAS but also the broader spectrum of Fetal Alcohol Spectrum Disorders (FASD), which encompasses conditions like partial fetal alcohol syndrome (pFAS), alcohol-related neurodevelopmental disorder (ARND), and alcohol-related birth defects (ARBD). This expansion reflected a growing understanding that prenatal alcohol exposure could result in a range of physical, cognitive, and behavioral impairments, even in the absence of the full FAS phenotype. Research during this period also emphasized the importance of early recognition and intervention to mitigate the long-term consequences of FASD.
In the 21st century, FAS recognition in medical literature has continued to evolve, with advancements in diagnostic tools, such as neuroimaging and genetic testing, aiding in the identification of affected individuals. Additionally, there has been a shift toward preventive strategies, including public health campaigns to educate women about the risks of alcohol consumption during pregnancy. Medical journals now frequently highlight the global prevalence of FASD, its economic and social impact, and the need for multidisciplinary approaches to care. Despite these advancements, challenges remain in diagnosing FAS, particularly in cases with subtle or atypical presentations, underscoring the ongoing need for research and awareness in medical literature.
In conclusion, the recognition of Fetal Alcohol Syndrome in medical literature has progressed significantly since its introduction in 1973. From its initial description to the development of diagnostic criteria and the expansion to FASD, the medical community has made substantial strides in understanding and addressing the effects of prenatal alcohol exposure. Continued research, education, and clinical vigilance are essential to further improve the identification, management, and prevention of FAS and its related disorders.
Alcohol: Pandemic Coping Mechanism or Crutch?
You may want to see also
Frequently asked questions
The term Fetal Alcohol Syndrome (FAS) was first introduced in 1973 by Dr. Kenneth Lyons Jones and Dr. David W. Smith.
The identification and naming of Fetal Alcohol Syndrome were based on observations of a pattern of birth defects and developmental issues in children born to mothers who consumed alcohol during pregnancy.
Dr. Kenneth Lyons Jones and Dr. David W. Smith, pediatric dysmorphologists at the University of Washington, were the researchers who coined the term Fetal Alcohol Syndrome.
The introduction of the term Fetal Alcohol Syndrome in 1973 raised awareness about the harmful effects of prenatal alcohol exposure and established it as a recognized medical condition, leading to further research and prevention efforts.




























