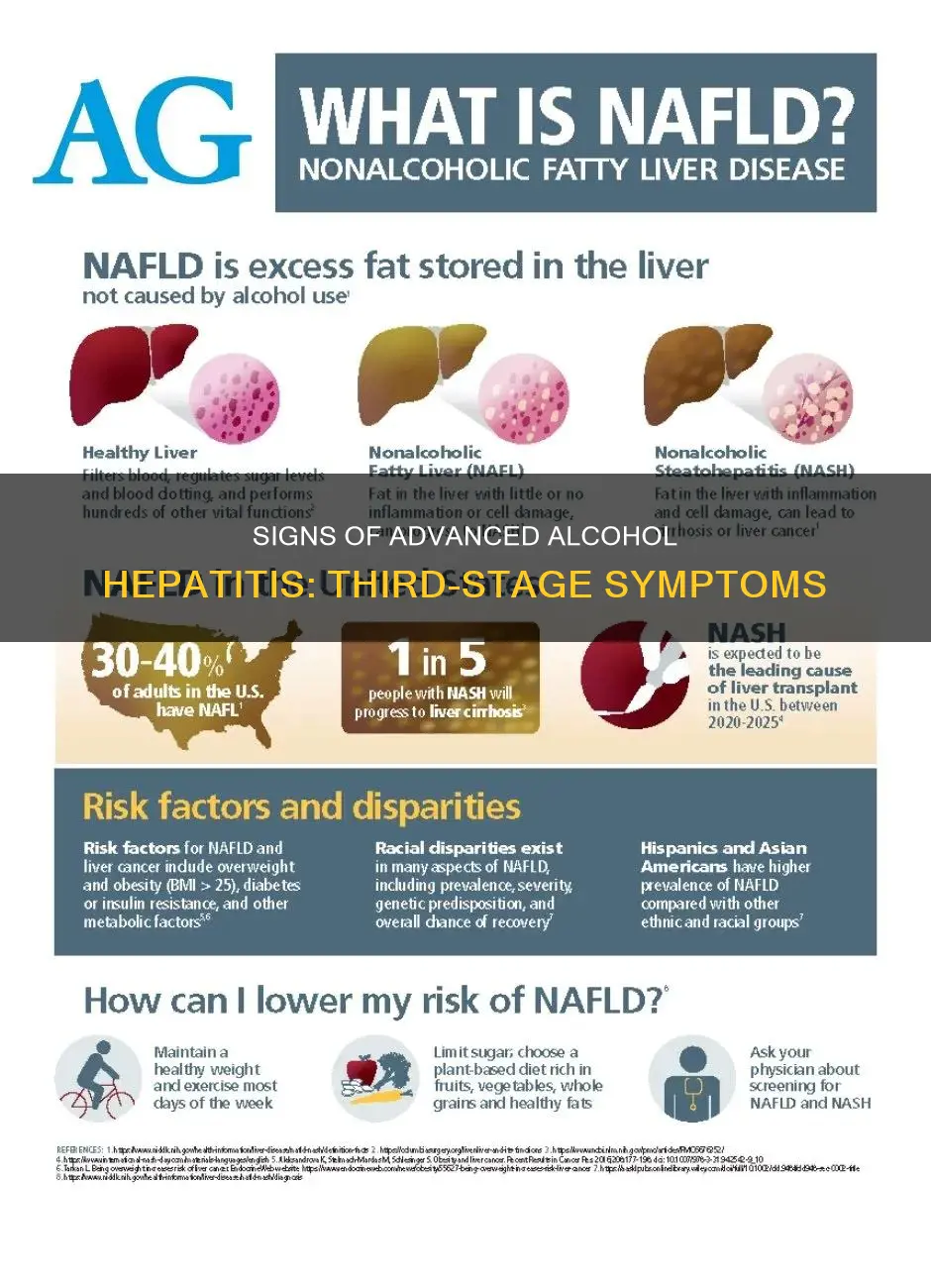
Alcoholic hepatitis is a condition caused by inflammation of the liver due to heavy alcohol consumption. While mild alcoholic hepatitis can be reversed by abstaining from alcohol, severe cases can lead to a 30% to 50% mortality rate within 30 days. The presence of jaundice and hepatic encephalopathy indicates a poorer outcome. One of the factors indicating the presence of third-stage alcohol hepatitis is decreased production of blood clotting factors.
| Characteristics | Values |
|---|---|
| Mechanism of Alcohol-induced Liver Injury | Translocation of endotoxins in the form of lipopolysaccharides (LPS) from the intestines into the hepatocytes |
| Binding of LPS in Hepatic Kupffer Cells | Release of reactive oxygen species (ROS) |
| Binding of ROS | Release of cytokines such as tumor necrosis factor-alpha (TNF alpha), interleukin-8, monocyte chemotactic protein 1 (MCP-1), and platelet-derived growth factor (PDGF) |
| Outcome of Binding of ROS | Accumulation of neutrophils, macrophages, and systemic clinical features of alcohol injury |
| Susceptibility to Alcoholic Liver Disease | Specific intestinal dysbiosis |
| Treatment | Patient education about the health risks of alcohol |
| MDF greater than 32 | 30-day mortality of 30% to 50% |
| MDF greater than 32 | 40% of patients die within 6 months |
| Indicators of Poorer Outcome | Jaundice and hepatic encephalopathy at the time of presentation |
| Cause of Alcoholic Hepatitis | Inflammation of the liver from alcohol use |
| Risk Factors | Heavy drinking over years, genetic differences, family history of alcohol use disorder or liver disease, sex differences |
Explore related products
![Prime Screen [25 Pack] EtG Alcohol Urine Test - at Home Rapid Testing Dip Card Kit - 80 Hour Low Cut-Off 300 ng/mL - WETG-114](https://m.media-amazon.com/images/I/51MNffSFwAL._AC_UL320_.jpg)
![ETG Alcohol Urine Test Strips | at Home ETG Test with 80 Hour Detection Window | Easy to Use Strips Deliver 5 Minute Results | Reliable Home Drug and Alcohol Screening Kit - [25 Pack] – 12 PANEL NOW](https://m.media-amazon.com/images/I/41IwM3Vyu7L._AC_UL320_.jpg)

$18.99

![Prime Screen Multi-Panel Urine Test - Testing for THC, Nicotine (COT), Alcohol Test (EtG) -[5 Pack]](https://m.media-amazon.com/images/I/71UdBzNsk8L._AC_UL320_.jpg)

What You'll Learn
![]()
Jaundice
In the context of alcohol hepatitis, jaundice is a significant symptom, indicating a poorer outcome for patients. Alcohol hepatitis is a severe syndrome related to alcoholic liver disease, and it is characterised by rapid-onset jaundice, along with other symptoms such as malaise, tender hepatomegaly, and subtle features of systemic inflammatory response. The diagnosis of alcoholic hepatitis is primarily clinical and must include acute-onset jaundice, specific laboratory abnormalities, and a history of long-term heavy alcohol consumption.
The presence of jaundice in patients with alcoholic hepatitis indicates more advanced liver damage and potential multi-organ failure. Jaundice is often accompanied by other symptoms, such as fever, tachycardia, tachypnea, hepatomegaly, and leukocytosis with neutrophilia. The combination of jaundice and these additional symptoms can help healthcare professionals diagnose alcoholic hepatitis and determine the severity of the disease.
The treatment for alcoholic hepatitis aims to address both the acute symptoms and the underlying cause. This includes supportive care, such as alcohol cessation and nutritional support, and, in some cases, pharmacological treatment for alcohol use disorder. Close monitoring for inflammation and organ failure is crucial, as alcoholic hepatitis can lead to significant morbidity and mortality, especially when accompanied by jaundice.
While jaundice is a key indicator of liver damage and hepatitis, it is important to note that not all patients with hepatitis will exhibit jaundice. However, when present, jaundice is a serious symptom that requires medical attention and comprehensive management of alcoholic hepatitis to improve patient outcomes.
Famous People Living with Fetal Alcohol Syndrome
You may want to see also
Explore related products
![ETG Alcohol Urine Test Strips, High Sensitivity | Cut-Off, 80 Hour Detection Window, Rapid 2-Minute Results for Home/Workplace/Rehab Testing [8 Pack]](https://m.media-amazon.com/images/I/61aUeQBtEEL._AC_UL320_.jpg)

![ETG Alcohol Urine Test Strips- at Home Testing Dip Card Kit - 80 Hours Suitable Cut Off 500 ng/mL - [12 Pack]](https://m.media-amazon.com/images/I/51IIU1-YsiL._AC_UL320_.jpg)



![]()
Hepatic encephalopathy
The symptoms of hepatic encephalopathy can vary in severity and may affect mental status, personality, and motor functions. The mildest form of hepatic encephalopathy may manifest as forgetfulness, mild confusion, irritability, and an inverted sleep-wake pattern. More severe symptoms include lethargy, personality changes, worsened confusion, and, in the most advanced stage, coma and seizures.
The West Haven Criteria is the most common grading system used to assess the severity of hepatic encephalopathy, ranging from stage 0 (minimal symptoms) to stage 4 (coma). Neuroimaging techniques such as CT scans and MRI may be used to detect abnormalities in the brain, although they are not always effective in diagnosing hepatic encephalopathy.
Elevated serum ammonia levels are a common feature of hepatic encephalopathy, occurring in 90% of cases. Liver transplantation is a treatment option for patients with end-stage liver disease, and it has been shown to improve cognitive function and correct excessive ammonia levels. Additionally, liver-assist devices, or "artificial livers," can be used to remove toxins from the blood and improve encephalopathy symptoms.
Underage Drinking: Asking for Alcohol, Legal or Not?
You may want to see also
Explore related products





![]()
Steatosis
The second stage of alcoholic liver disease is inflammation of the liver cells, which can lead to alcoholic hepatitis if alcohol consumption continues. This inflammation damages the liver tissue, a condition known as steatohepatitis. The outcome of alcoholic hepatitis depends on the severity of the damage. Alcohol abstinence, nutritional support, and treatment of infection can help manage alcoholic hepatitis. However, more severe cases can lead to liver failure.
The final stage of alcoholic liver disease is alcoholic cirrhosis, where extensive scar tissue replaces healthy liver tissue. This stage of liver damage is irreversible and leads to complications such as portal hypertension. While steatosis and steatohepatitis lesions may be reversible after alcohol cessation, up to 20% of patients with steatosis may still progress to cirrhosis.
Selling Alcohol from Home: Is It Legal?
You may want to see also
Explore related products






![]()
Hepatocyte ballooning
The underlying mechanisms of hepatocyte ballooning involve increased endoplasmic reticulum stress and dysfunction, oxidative stress, and abnormalities of the cytoskeleton. The endoplasmic reticulum is responsible for protein synthesis and lipid metabolism, and its dysfunction can lead to the accumulation of fat droplets within the hepatocytes. This accumulation of fat droplets is a common finding in hepatocyte ballooning, and it is believed that the abnormal disposition of these fat droplets, rather than the total fat content, contributes to the pathogenesis of NASH. Additionally, the close association of ballooning with the formation of Mallory-Denk bodies has been observed, which are potential indicators of preneoplastic changes.
The presence of hepatocyte ballooning can be challenging to assess and interpret, even for expert liver pathologists. It can be confused with cellular oedema and microvesicular steatosis, and there is significant inter-observer variability. However, the use of artificial intelligence in detection and interpretation may provide new possibilities for future diagnosis and treatment.
In terms of treatment, hepatocyte ballooning has been associated with the activation of the sonic hedgehog pathway. This pathway is involved in cell proliferation, survival, and differentiation, and its activation may play a role in the development of liver disease. Additionally, caspase 9, an enzyme involved in the apoptotic pathway, is diminished in ballooned hepatocytes, suggesting that these cells may not be on the path to cellular death but rather have a functional role.
While the specific mention of hepatocyte ballooning in the context of third-stage alcohol hepatitis was not explicit in the search results, the accumulation of fat in hepatocytes is recognised as the initial pathological change in alcoholic liver disease. This accumulation of fat in hepatocytes is a key feature of hepatocyte ballooning, as discussed. Therefore, it can be inferred that hepatocyte ballooning is indicative of the presence of alcoholic liver disease, including third-stage alcohol hepatitis.
Alcohol That Won't Give You Away: Breath-Friendly Booze
You may want to see also
Explore related products





![]()
Infiltration of neutrophils
Alcohol-related liver disease is a major cause of liver disease-associated mortality. Alcohol-related hepatitis (AH) is an acute inflammatory form of alcohol-related liver disease. The presence of AH is associated with increased numbers of circulating and hepatic neutrophils.
Neutrophils are regarded as important participants that affect the process of liver injury and repair. Neutrophil dysfunction leads to infection susceptibility and increased mortality in advanced liver diseases. The degree of neutrophil infiltration is related to the recovery from acute alcoholic hepatitis and is related to 90-day mortality in patients with alcoholic hepatitis. Therefore, the balance of neutrophils between the antibacterial and anti-inflammatory processes needs to be carefully considered in patients with alcoholic liver disease.
Several chemokines, including CXCL1, CXCL2, and CXCL8, promote neutrophil recruitment. Activated Kupffer cells can directly influence neutrophil recruitment through the secretion of CXCL2, which binds to the C-X-C motif chemokine receptor 2 (CXCR2) on neutrophils. Cytokines produced by activated Kupffer cells can also promote neutrophil recruitment indirectly through stimulation of other cell types. For example, interleukin (IL)-1 and IL-6 activate T helper 17 cells, prompting the release of IL-17, which stimulates hepatic stellate cell production.
TLR2 and TLR9 contribute to alcohol-mediated liver injury through the induction of CXCL1 and neutrophil infiltration. In a murine model of AH, CXCL1 production by hepatocytes and hepatic stellate cells was upregulated, even when Kupffer cells were depleted using clodronate. Tlr2 and Tlr9 knockout mice exhibited reduced hepatic CXCL1 protein, reduced serum CXCL1, and reduced neutrophil infiltration compared with wild-type mice.
In a viral hepatitis model induced by lymphocytic choriomeningitis virus infection, deletion of neutrophils increased the viral load, aggravated the T-cell response, and increased liver injury, while IL-33 treatment contributed to reducing liver inflammation by promoting the aggregation and immunosuppressive phenotype transformation of neutrophils within the liver. Increased infiltration of neutrophils into liver tissue is also exacerbated by endogenous IL-33 deficiency. These data indicate that IL-33 might be a target for reducing neutrophil infiltration in hepatitis, and IL-33 targeting therapy might benefit the outcome of viral hepatitis.
Tequila Allergy Mystery: Why Am I Allergic Only to Tequila?
You may want to see also
Frequently asked questions
Symptoms of alcohol-induced hepatitis include inflammation of the liver, tenderness or soreness in the upper right abdomen, jaundice, fever, tachycardia, tachypnea, hepatomegaly, leukocytosis with neutrophilia, and an AST:ALT elevation greater than 1.5:1.
Alcohol-induced hepatitis is caused by heavy, long-term alcohol consumption. Alcohol acts as a toxin in the liver, overloading it with fat and toxins to process. When the liver can no longer keep up, toxins and fat build up and begin to injure the liver.
Treatment of alcohol-induced hepatitis involves patient education about the health risks of alcohol and quitting drinking to prevent further liver damage. Mild alcoholic hepatitis can be reversed with the cessation of alcohol consumption. A diet consisting of 100 g/day of protein is recommended, supplemented with multivitamins including folate and thiamine.