The question of why a doctor would list alcohol dependence on paperwork is a significant one, as it touches on both medical accuracy and patient care. When a doctor documents alcohol dependence, it is typically done to ensure a comprehensive medical record, which is crucial for proper treatment planning and continuity of care. This diagnosis may be included in medical notes, insurance claims, or referrals to specialists, serving as a critical indicator of a patient’s health status. Alcohol dependence is a recognized medical condition, and its inclusion in paperwork can facilitate access to specialized treatment programs, support services, and necessary interventions. However, patients may feel stigmatized or concerned about the implications of such a diagnosis, making it essential for healthcare providers to communicate openly and sensitively about the reasoning behind this documentation. Understanding the purpose and potential consequences of this notation can help patients navigate their care more effectively.
Explore related products






What You'll Learn
- Diagnosis Codes: ICD-10 codes for alcohol dependence, e.g., F10.20
- Documentation Requirements: Details needed for accurate medical recordkeeping
- Treatment Plans: Alcohol dependence management strategies in paperwork
- Legal Implications: Consequences of misreporting alcohol dependence on forms
- Insurance Billing: How alcohol dependence affects medical claims processing
![]()
Diagnosis Codes: ICD-10 codes for alcohol dependence, e.g., F10.20
When documenting alcohol dependence on medical paperwork, healthcare providers use standardized diagnosis codes from the International Classification of Diseases, 10th Revision (ICD-10). These codes ensure consistency and accuracy in medical records, billing, and statistical reporting. For alcohol dependence, the primary ICD-10 code is F10.20, which specifically denotes "Alcohol dependence, uncomplicated." This code is used when a patient meets the diagnostic criteria for alcohol dependence without any additional complications, such as withdrawal symptoms or other health issues directly related to alcohol use. It is crucial for clinicians to select the most precise code to reflect the patient's condition accurately.
The ICD-10 coding system provides additional subcategories under F10.2 to capture more nuanced aspects of alcohol dependence. For example, F10.21 is used for "Alcohol dependence with withdrawal," indicating that the patient experiences withdrawal symptoms when alcohol use is reduced or stopped. F10.22 specifies "Alcohol dependence with withdrawal, with perceptual disturbance," which includes hallucinations or other sensory disturbances during withdrawal. F10.23 is for "Alcohol dependence with withdrawal, with convulsions," indicating seizures related to alcohol withdrawal. These codes allow healthcare providers to document the severity and specific manifestations of alcohol dependence, guiding appropriate treatment and management.
In some cases, a patient may have alcohol dependence but not currently be experiencing withdrawal symptoms. For such scenarios, F10.20 remains the appropriate code, as it focuses solely on the dependence itself. It is essential for clinicians to assess the patient thoroughly to determine whether additional codes are necessary to capture complications or comorbid conditions. For instance, if a patient has both alcohol dependence and alcoholic liver disease, the provider would use F10.20 for dependence and K70.0 for alcoholic fatty liver to provide a comprehensive picture of the patient's health status.
Proper use of ICD-10 codes like F10.20 is not only critical for clinical documentation but also for administrative purposes, such as insurance billing and public health reporting. Insurance companies rely on these codes to determine coverage for treatments like detoxification programs, counseling, or medication-assisted therapy. Additionally, accurate coding contributes to epidemiological data, helping public health officials track the prevalence and impact of alcohol dependence in populations. Therefore, healthcare providers must stay updated on ICD-10 guidelines to ensure compliance and effective patient care.
Lastly, it is important to note that the choice of ICD-10 code should align with the patient's current condition at the time of documentation. If a patient transitions from uncomplicated alcohol dependence to a state with withdrawal symptoms, the code should be updated accordingly. Regular reassessment and accurate coding are vital to reflect the dynamic nature of alcohol dependence and to ensure that patients receive the most appropriate interventions. By adhering to these coding practices, healthcare providers can maintain high standards of care and contribute to better health outcomes for individuals with alcohol dependence.
North Carolina's Legal Alcohol Limit Explained
You may want to see also
Explore related products




$23.58 $25.95


![]()
Documentation Requirements: Details needed for accurate medical recordkeeping
When documenting alcohol dependence in medical records, healthcare providers must adhere to specific documentation requirements to ensure accuracy, compliance, and effective patient care. The first critical detail is a clear and precise diagnosis using standardized terminology. Physicians should use the ICD-10 code (International Classification of Diseases, 10th Revision) for alcohol dependence, which is typically F10.20 for alcohol dependence, unspecified. If the patient is in remission, the appropriate code (e.g., F10.20 with a remission specifier) must be included. This ensures consistency and clarity across medical records and billing systems.
The documentation should also include a detailed patient history related to alcohol use. This involves noting the duration, frequency, and quantity of alcohol consumption, as well as any previous attempts to quit or reduce intake. Providers must document the patient’s self-reported information and any observable signs of alcohol dependence, such as withdrawal symptoms, tolerance, or negative impacts on personal, social, or occupational functioning. Including this information provides context for the diagnosis and supports treatment planning.
Another essential component is the assessment of severity and risk factors. Physicians should evaluate the severity of alcohol dependence using validated tools like the Audit-C or CAGE questionnaire and document the results. Risk factors such as family history of substance use disorders, co-occurring mental health conditions, or medical complications (e.g., liver disease) must also be noted. This comprehensive assessment helps in tailoring interventions and monitoring progress over time.
Treatment plans and interventions should be clearly documented as well. This includes any pharmacological treatments (e.g., disulfiram, naltrexone), counseling referrals (e.g., cognitive-behavioral therapy, support groups like AA), and follow-up appointments. Providers must also document patient education efforts, such as discussions about the risks of continued alcohol use and strategies for relapse prevention. This ensures continuity of care and accountability.
Finally, progress notes and outcomes are vital for ongoing documentation. Physicians should regularly update the medical record with the patient’s response to treatment, any changes in alcohol use patterns, and adjustments to the care plan. Documenting relapses, if they occur, along with the steps taken to address them, is equally important. Accurate and timely progress notes not only support patient care but also protect the provider in case of legal or regulatory scrutiny. Adhering to these documentation requirements ensures that medical records are thorough, compliant, and reflective of the patient’s journey toward recovery.
Understanding Legal Alcohol Limits for Safe Driving: What You Need to Know
You may want to see also
Explore related products






![]()
Treatment Plans: Alcohol dependence management strategies in paperwork
When documenting alcohol dependence in medical paperwork, doctors typically outline comprehensive treatment plans that address both the physical and psychological aspects of the condition. These plans are tailored to the individual’s needs, severity of dependence, and any co-occurring disorders. The primary goal is to achieve abstinence, prevent relapse, and improve overall quality of life. Treatment plans often include a combination of pharmacotherapy, behavioral interventions, counseling, and support systems. Documentation is detailed, clear, and structured to ensure continuity of care and compliance with medical standards.
Assessment and Diagnosis: The first step in the paperwork is a thorough assessment of the patient’s alcohol use, including frequency, quantity, and duration of consumption. Doctors use standardized tools like the Alcohol Use Disorders Identification Test (AUDIT) or the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria to diagnose alcohol dependence. This assessment also evaluates medical history, mental health status, and social factors that may contribute to the dependence. The diagnosis is clearly stated in the paperwork, often coded using ICD-10 (International Classification of Diseases, 10th Edition) for billing and record-keeping purposes.
Pharmacotherapy: Treatment plans frequently include medications to manage withdrawal symptoms, reduce cravings, and support long-term sobriety. Commonly prescribed medications are documented, such as disulfiram, naltrexone, or acamprosate. The doctor specifies the dosage, frequency, and duration of the medication, along with potential side effects and monitoring requirements. For example, naltrexone may be prescribed to reduce alcohol cravings, and the paperwork will note the need for regular liver function tests. This section also includes instructions for tapering or discontinuing medications if necessary.
Behavioral and Psychological Interventions: Doctors outline evidence-based therapies to address the psychological aspects of alcohol dependence. Cognitive Behavioral Therapy (CBT), Motivational Interviewing (MI), and contingency management are commonly documented strategies. The paperwork details the frequency and duration of therapy sessions, goals of treatment (e.g., developing coping skills, identifying triggers), and the therapist’s role in the patient’s care. If the patient is enrolled in a structured program like a 12-step group (e.g., Alcoholics Anonymous), this is also noted, emphasizing the importance of ongoing support.
Support Systems and Aftercare: A critical component of the treatment plan is the establishment of a strong support network. Doctors document referrals to support groups, family therapy, or community resources. Aftercare planning is detailed, including follow-up appointments, relapse prevention strategies, and emergency contacts. The paperwork may also include a crisis management plan, outlining steps to take if the patient experiences a relapse or severe withdrawal symptoms. This ensures that the patient has access to immediate help when needed.
Monitoring and Progress Tracking: Regular monitoring is essential to assess the effectiveness of the treatment plan. Doctors document scheduled follow-up visits, lab tests (e.g., liver function, blood alcohol levels), and self-reported progress. The paperwork includes benchmarks for success, such as reduced alcohol consumption or improved mental health symptoms. Adjustments to the treatment plan are made as needed, and these changes are clearly documented to reflect the evolving nature of the patient’s care. This ensures accountability and continuity in managing alcohol dependence.
Intermolecular Forces: Boiling Points of Alcohols vs Aldehydes
You may want to see also
Explore related products






![]()
Legal Implications: Consequences of misreporting alcohol dependence on forms
Misreporting alcohol dependence on medical or legal forms can have severe legal implications for both healthcare providers and patients. When a doctor inaccurately documents a patient’s alcohol dependence, whether by omission, exaggeration, or error, it can lead to a cascade of legal consequences. For healthcare providers, such misreporting may be considered medical malpractice if it results in harm to the patient. For instance, if a patient is incorrectly labeled as alcohol dependent, they may face discrimination in employment, insurance, or legal proceedings, opening the door for lawsuits against the provider. Conversely, failing to document alcohol dependence when it is present could result in inadequate treatment, liability for negligence, and potential harm to the patient, further exposing the provider to legal action.
From a patient’s perspective, misreported alcohol dependence on forms can have far-reaching legal repercussions. In legal contexts, such as custody battles, disability claims, or criminal cases, inaccurate documentation can be used against the individual. For example, if a parent is falsely labeled as alcohol dependent, it could jeopardize their chances of retaining custody of their children. Similarly, in insurance claims, misreporting could lead to denied benefits or increased premiums. In criminal cases, inaccurate documentation might influence sentencing or probation conditions, particularly in DUI or substance-related offenses. These outcomes underscore the importance of accurate reporting to protect the patient’s legal rights and interests.
Healthcare providers must also be aware of the legal obligations imposed by regulatory bodies and laws such as the Health Insurance Portability and Accountability Act (HIPAA) in the United States. Misreporting alcohol dependence could be seen as a breach of patient confidentiality or a violation of ethical standards, leading to investigations, fines, or loss of licensure. Additionally, if the misreporting is intentional or fraudulent, providers may face criminal charges for falsifying medical records. Such actions not only damage the provider’s reputation but also erode trust in the healthcare system, further emphasizing the need for precision and integrity in medical documentation.
For employers and institutions relying on medical forms, misreported alcohol dependence can create legal vulnerabilities. If an employee is incorrectly labeled as alcohol dependent, the employer may face claims of discrimination or wrongful termination if adverse actions are taken based on this misinformation. Similarly, educational institutions or licensing boards may face legal challenges if they deny opportunities to individuals based on inaccurate medical reports. These scenarios highlight the broader legal implications of misreporting, extending beyond the patient-provider relationship to impact various stakeholders.
In conclusion, the legal implications of misreporting alcohol dependence on forms are profound and multifaceted. For healthcare providers, it risks malpractice claims, regulatory penalties, and criminal charges. For patients, it can lead to discrimination, loss of legal rights, and adverse outcomes in personal and legal matters. Institutions relying on such documentation may also face legal challenges if decisions are based on inaccurate information. To mitigate these risks, healthcare providers must ensure accurate, ethical, and transparent documentation, while patients should verify the correctness of their medical records. Awareness of these legal consequences is crucial for all parties involved to uphold integrity and protect rights in medical and legal contexts.
Resisting Alcohol Peer Pressure: Strategies to Confidently Say No
You may want to see also
Explore related products






![]()
Insurance Billing: How alcohol dependence affects medical claims processing
When a doctor documents alcohol dependence on a patient’s medical paperwork, it significantly impacts insurance billing and claims processing. Insurance companies rely on accurate medical coding to determine coverage, and alcohol dependence is typically classified under specific diagnostic codes, such as those in the ICD-10 (International Classification of Diseases, 10th Edition). The most common code for alcohol dependence is F10.20, which indicates alcohol dependence without withdrawal symptoms. Accurate coding is critical because it directly influences whether the claim is approved, denied, or flagged for further review. Incorrect or incomplete documentation can lead to claim rejections, delays in reimbursement, or requests for additional information from the insurer.
The presence of alcohol dependence on medical paperwork often triggers additional scrutiny from insurance providers. Many insurers have specific policies regarding substance use disorders, including alcohol dependence, and may require pre-authorization for certain treatments or medications. For example, if a patient seeks inpatient rehabilitation or counseling services, the insurer may review the claim more closely to ensure the treatment is medically necessary and aligns with their coverage guidelines. This can slow down the claims processing timeline, as insurers may request detailed treatment plans, progress notes, or other supporting documentation from the provider.
Alcohol dependence can also affect the reimbursement rates for medical claims. Some insurers may categorize treatments related to substance use disorders under behavioral health benefits, which often have different coverage limits or copay structures compared to general medical services. Additionally, if the patient’s alcohol dependence is deemed a pre-existing condition, it could impact their eligibility for certain benefits or result in higher out-of-pocket costs. Providers must ensure that the documentation clearly links the treatment to the diagnosed condition to avoid disputes over reimbursement.
Another critical aspect is the potential for insurers to deny claims if they determine the treatment is not directly related to the patient’s alcohol dependence or if the diagnosis is not adequately supported by clinical evidence. For instance, if a patient seeks treatment for a condition exacerbated by alcohol use (e.g., liver disease), the insurer may require proof that the treatment is medically necessary and not solely related to lifestyle choices. This underscores the importance of thorough and precise documentation by the provider, including detailed notes on the patient’s history, assessment, and treatment plan.
Finally, the inclusion of alcohol dependence on medical paperwork can have long-term implications for the patient’s insurance record. Insurers may flag patients with substance use disorders for future claims, potentially affecting their coverage options or premiums. Providers should be transparent with patients about how this documentation may impact their insurance and ensure they understand the potential consequences. By adhering to best practices in coding and documentation, healthcare providers can streamline the claims process, minimize denials, and ensure patients receive the care they need while maximizing insurance reimbursement.
Chilling Truth: Why Alcohol Withdrawals Leave You Feeling So Cold
You may want to see also
Frequently asked questions
It means the doctor has diagnosed the patient with a condition characterized by an inability to control or stop alcohol use despite negative consequences.
A doctor documents alcohol dependence to ensure accurate medical history, guide treatment plans, and comply with legal or insurance requirements.
Yes, it may impact insurance premiums or coverage and could be relevant in certain employment contexts, especially in safety-sensitive roles.
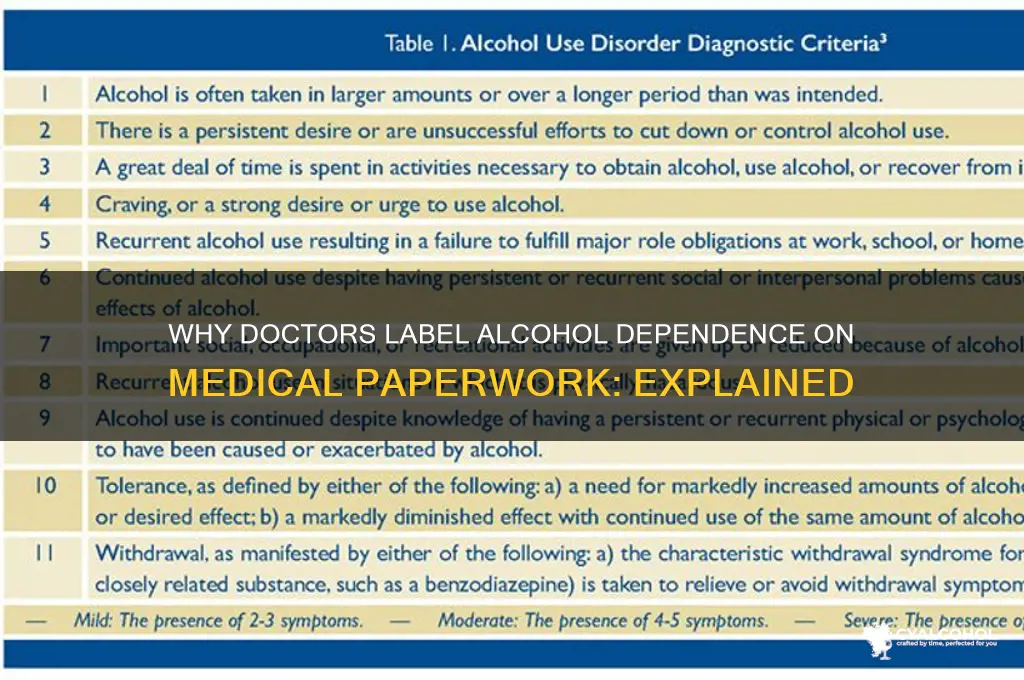
It is diagnosed based on criteria from the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders), including patterns of alcohol use and related impairments.
No, diagnoses cannot be removed from medical records, but patients can request corrections if they believe the diagnosis is inaccurate.






















