Alcoholic cirrhosis, a chronic liver disease, is caused by heavy alcohol consumption, which results in the replacement of healthy liver tissue with scar tissue. This condition can lead to impaired memory and concentration, increasing the risk of falls. Patients with alcoholic cirrhosis often experience comorbidities, with the most common being hepatitis C, hepatitis B, and chronic pancreatitis. Hepatitis C is another leading cause of cirrhosis, and when combined with alcohol abuse, it can accelerate the progression of the disease. Other comorbidities associated with alcoholic cirrhosis include jaundice, hepatic encephalopathy, variceal bleeding, hepatocellular carcinoma, and decompensated cirrhosis. Decompensated cirrhosis can be triggered by factors such as infection, diet, constipation, dehydration, and increased alcohol intake. It is important to note that alcoholic cirrhosis is typically diagnosed through medical history, drinking history, and specific tests that confirm liver damage and rule out other conditions.
| Characteristics | Values |
|---|---|
| Comorbidities | Small bowel bacterial overgrowth, chronic pancreatitis, gallstone formation, impaired memory, concentration, and increased risk for falls |
| Diagnosis | Medical history, drinking history, blood tests, liver biopsy, CT scan, liver function tests, physical examination |
| Treatment | Lactulose, lifestyle changes (diet, exercise, limit salt), alcohol abstinence, liver transplant |
Explore related products






What You'll Learn
![]()
Hepatic encephalopathy
The liver is responsible for removing harmful toxins, such as ammonia, from the blood. When the liver is severely damaged, it can no longer perform this function effectively. This results in the buildup of toxins in the blood, which can eventually reach the brain. The toxins can cause brain cells to swell and interfere with the normal signalling between brain cells, leading to mental and physical health issues.
The symptoms of HE can be subtle and gradual, making it challenging to diagnose in its early stages. It is often a family member or friend who spots the first signs, which can include flapping hands or poor coordination. HE can be mistaken for dementia or depression. The severity of HE is typically assessed using the West Haven system, grading it from 0 to 4, with grade 0 being minimal HE and grade 1 involving subtle confusion or mood changes.
The management of HE focuses on supportive care and ammonia-lowering therapy. Common medications used include disaccharides such as lactulose and lactitol, which help to reduce blood ammonia levels. Rifaximin, an antibiotic, is also prescribed.
It is important for patients with HE to carry an alert card or medical bracelet to ensure that medical professionals are aware of their condition in case of an emergency. Additionally, lifestyle changes, such as maintaining a healthy diet and regular exercise, can help manage the condition.
Alcoholic Parent, Guilty Son: Navigating Complex Emotions
You may want to see also
Explore related products






![]()
Hepatocellular carcinoma
Alcoholic liver cirrhosis is a chronic condition that develops over time, where healthy liver tissue is replaced by scar tissue. This is caused by liver swelling due to heavy alcohol consumption. Alcoholic cirrhosis is the most advanced form of liver disease linked to alcohol consumption, and it can lead to other serious complications.
One such comorbidity is hepatocellular carcinoma (HCC), which is a form of liver cancer. HCC is the most common type of primary liver cancer, and its incidence has been increasing in recent decades. Almost 90% of HCC cases develop in conjunction with underlying chronic liver disease, usually in an advanced state, and accompanied by severe liver fibrosis and cirrhosis. The risk of developing HCC increases with alcohol consumption, and alcohol abuse can increase the risk of HCC by two to four times compared to those who abstain.
Several risk factors for HCC have been identified in patients with alcoholic cirrhosis. These include older age, male sex, severity of compensated cirrhosis, and sustained activity of liver disease. In addition, coinfections such as hepatitis B and C viruses (HBV/HCV) and hepatitis B and D viruses (HBV/HDV) can further elevate the risk of HCC. The presence of both age (>55 years) and a low platelet count (<125,000) are also strong indicators of a higher risk of developing HCC within the next 5 years.
The mortality rate of HCC associated with cirrhosis is rising in some developed countries. HCC is now the leading cause of liver-related deaths in patients with compensated cirrhosis. The highest incidence of HCC in cirrhosis patients is associated with hepatitis C virus (HCV) infection, followed by hereditary hemochromatosis. The 5-year cumulative risk of HCC in alcoholic cirrhotics without HCV or hepatitis B virus (HBV) infection is 8%.
Further research is being conducted to refine the stratification of patients with alcoholic cirrhosis into different HCC risk categories. This involves combining genetic variants, changes in serum or plasma biomarkers, and clinical data. These advancements will help optimise screening, preventive measures, and early diagnosis for this challenging patient population.
Treating Sobriety: Navigating the Highs and Lows
You may want to see also
Explore related products

$29.29





![]()
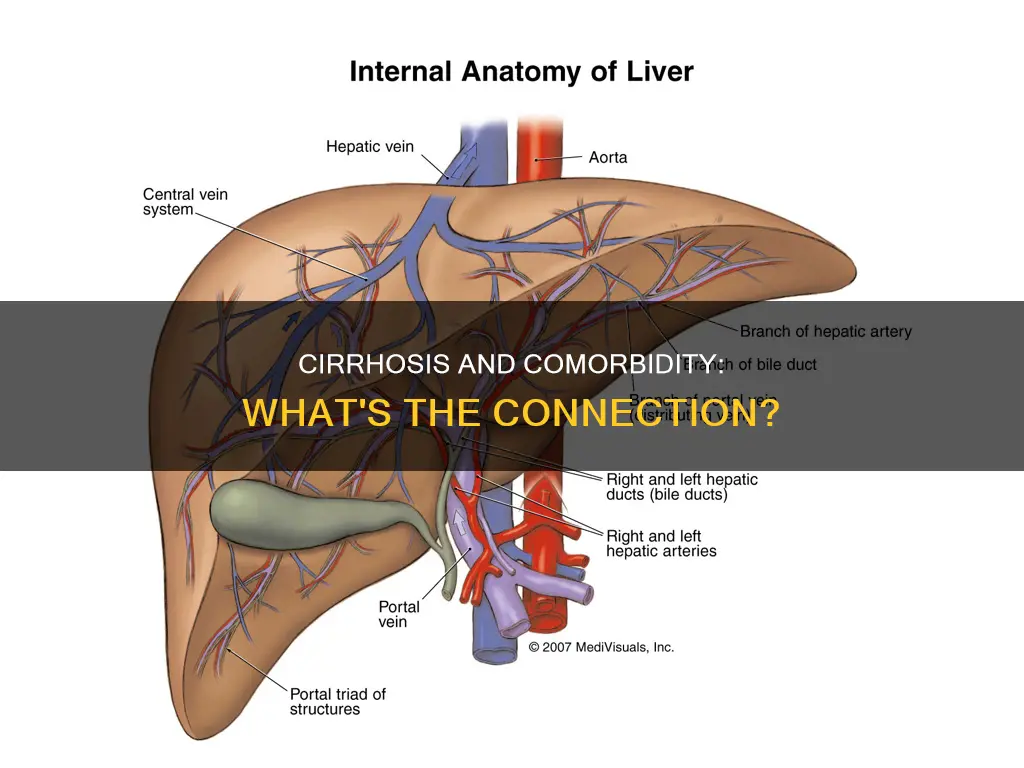
Hepatic vein fibrosis
The development of hepatic fibrosis is triggered by chronic liver injury, especially when accompanied by inflammation. This persistent inflammation, often associated with hepatitis, stimulates repair cells to deposit collagen continuously. The excess collagen stiffens the tissue, and without a signal to stop the process, more collagen is deposited, leading to fibrosis.
Fibrosis can develop rapidly in cases of mechanical biliary obstruction. It is initiated by the activation of hepatic perivascular stellate cells (Ito cells), which store fat. These cells, along with adjacent cells, proliferate and transform into contractile cells called myofibroblasts. Myofibroblasts produce excessive amounts of an abnormal matrix, consisting of collagen, other glycoproteins, and matricellular proteins. This process contributes to increased portal vein resistance and reduced blood supply to the liver, leading to hepatocellular dysfunction and portal hypertension.
Fibrosis typically does not cause symptoms in its early stages, and many people may not be diagnosed until they develop cirrhosis. However, once fibrosis progresses, it can lead to symptoms such as jaundice, variceal bleeding, ascites, and portosystemic encephalopathy. Diagnosis of fibrosis is based on blood tests, imaging techniques, and occasionally liver biopsy. Treatment focuses on correcting the underlying condition when possible. Early detection is crucial, as fibrosis can be reversed if treated promptly, preventing the development of cirrhosis and liver cancer.
Melrose Wakefield: Alcohol Detox Inpatient Care
You may want to see also
Explore related products






![]()
Alcohol misuse
Alcohol-related cirrhosis can progress through several stages, beginning with fatty liver disease and potentially advancing to alcohol-related hepatitis before reaching the stage of alcohol-related cirrhosis. However, it is important to note that not all patients with alcohol-related cirrhosis will have previously experienced alcohol-related hepatitis. The progression of the disease is influenced by various factors, including the amount of alcohol consumed and individual differences in susceptibility.
The treatment for alcohol-related cirrhosis aims to slow down the buildup of scar tissue and prevent further liver damage. Lifestyle changes, including alcohol abstinence, are crucial in managing the disease. Medical treatments, such as lactulose, may be prescribed to improve symptoms and energy levels. In severe cases where the liver fails, a liver transplant may be necessary.
It is important to note that alcohol misuse can lead to other health complications beyond cirrhosis. Alcoholic liver disease, for example, can progress to hepatitis and eventually cirrhosis if left untreated. Therefore, early intervention and management of alcohol misuse are essential to prevent the development of these comorbidities and improve patient outcomes.
Alcohol at Weddings: Who Gets to Drink?
You may want to see also
Explore related products






![]()
Hepatitis
Alcoholic hepatitis is a clinical syndrome characterised by acute-onset jaundice and liver enzyme abnormalities resulting from long-term heavy alcohol use. It is a precursor to alcoholic cirrhosis, with 10% to 20% of patients with alcoholic hepatitis progressing to cirrhosis annually. Alcoholic hepatitis is diagnosed primarily through clinical observation, with a liver biopsy only required in uncertain cases. The classical histological features of alcoholic hepatitis include steatosis, hepatocellular ballooning, cholestasis, chicken-wire fibrosis, and cirrhosis in severely ill patients.
The risk of developing alcoholic hepatitis increases with the amount and duration of alcohol consumption. A typical diagnosis is between the ages of 40 and 60, with a history of consuming more than 100 grams of alcohol per day for a decade. The risk for cirrhosis increases exponentially with consumption over one drink per day, and drinking daily outside of meals further increases the risk.
The treatment for alcoholic hepatitis primarily consists of supportive care, including alcohol cessation and nutritional support. Abstinence from alcohol is the most important treatment, with patients who quit alcohol having a normal life expectancy. Corticosteroids, such as prednisolone, are recommended for severe alcoholic hepatitis to reduce inflammation. However, long-term benefits are questionable, and patients on steroids are prone to infections.
Protein-calorie malnutrition is a common comorbidity of alcoholic hepatitis due to decreased nutritional intake, gut absorption issues, and catabolic metabolism. Nutritional support is crucial, and dietitian consultation should be considered. Inpatient management may involve a structured alcohol withdrawal protocol, such as the Clinical Institute Withdrawal Assessment for Alcohol Revised, to guide benzodiazepine dosing and prevent withdrawal symptoms.
Spicy Food and Alcoholism: A Surprising Link
You may want to see also
Frequently asked questions
Alcoholic cirrhosis is a chronic liver disease caused by long-term alcohol consumption. It is characterised by the replacement of healthy liver tissue with scar tissue, which can lead to liver failure.
Patients with alcoholic cirrhosis often develop kidney problems, gastrointestinal bleeding, fluid in the belly, confusion, liver cancer, and severe infections. They are also at an increased risk of small bowel bacterial overgrowth and chronic pancreatitis.
Doctors diagnose alcoholic cirrhosis by taking a medical history, discussing drinking history, and running tests. These tests may include blood tests, liver biopsies, ultrasounds, and CT scans.