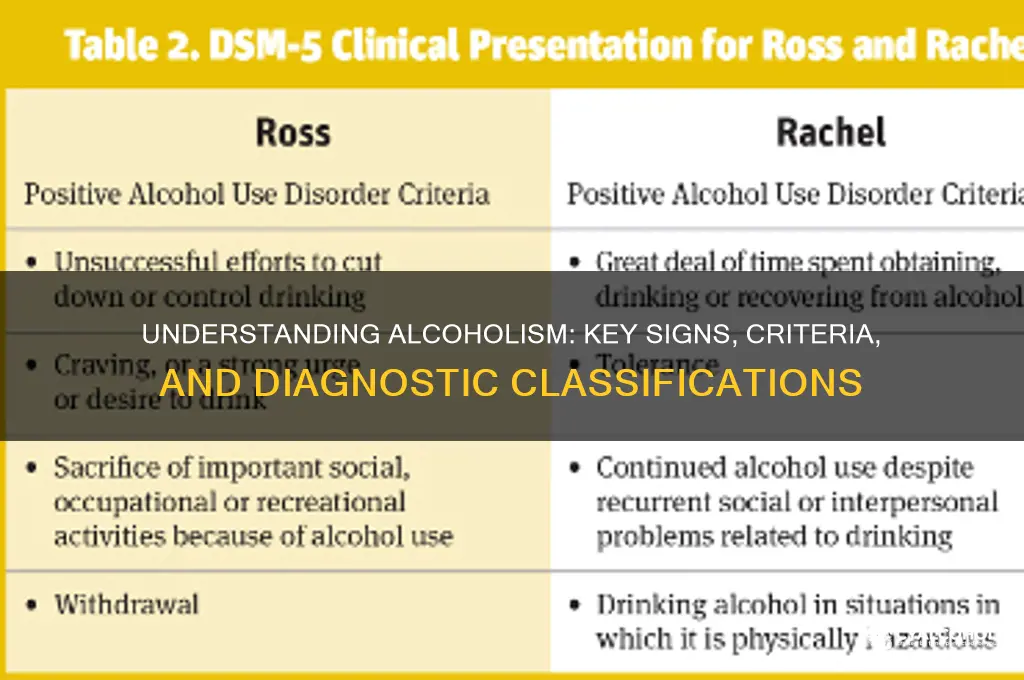
Alcoholism, also known as alcohol use disorder (AUD), is a chronic and often progressive condition characterized by an individual's inability to control or stop alcohol consumption despite adverse consequences. It is classified as a medical disorder by organizations like the American Psychiatric Association and the World Health Organization. Key indicators include a strong craving for alcohol, continued use despite physical, mental, or social harm, and the development of tolerance and withdrawal symptoms. Diagnosis typically involves assessing patterns of drinking, the impact on daily life, and the presence of physical or psychological dependence. Understanding what classifies as alcoholism is crucial for early intervention and effective treatment, as it distinguishes problematic drinking from moderate or social alcohol consumption.
| Characteristics | Values |
|---|---|
| Craving | A strong need or urge to drink alcohol. |
| Loss of Control | Inability to stop drinking once started, despite intentions to do so. |
| Physical Dependence | Withdrawal symptoms (e.g., nausea, sweating, shaking) when not drinking. |
| Tolerance | Needing more alcohol over time to achieve the same effect. |
| Neglecting Responsibilities | Failing to fulfill obligations at work, school, or home due to drinking. |
| Continued Use Despite Problems | Drinking despite knowing it causes physical, social, or interpersonal issues. |
| Time Spent Drinking | Spending a significant amount of time drinking or recovering from alcohol use. |
| Reduced Social/Recreational Activities | Giving up or reducing activities once enjoyed due to alcohol use. |
| Risky Behavior | Engaging in dangerous activities (e.g., driving) while under the influence. |
| Failed Attempts to Quit | Repeated unsuccessful efforts to cut down or stop drinking. |
| Diagnosis Criteria (DSM-5) | Meeting 2 or more of the above criteria within a 12-month period. |
Explore related products






What You'll Learn
- Frequency of Drinking: How often alcohol is consumed to be classified as alcoholism
- Quantity Consumed: Amount of alcohol intake that defines alcoholic behavior
- Dependence Signs: Physical or psychological reliance on alcohol as a key indicator
- Negative Consequences: Continued drinking despite harmful personal, social, or health impacts
- Withdrawal Symptoms: Experiencing withdrawal effects when alcohol consumption is reduced or stopped
![]()
Frequency of Drinking: How often alcohol is consumed to be classified as alcoholism
The frequency of alcohol consumption is a critical factor in determining whether an individual’s drinking habits cross the line into alcoholism. While occasional drinking may not raise red flags, consistent and excessive consumption patterns often signal a deeper issue. For instance, the National Institute on Alcohol Abuse and Alcoholism (NIAAA) defines heavy drinking as consuming 4 or more drinks on any day for men, or 3 or more for women. When this behavior occurs 5 or more days in a month, it significantly increases the risk of alcohol use disorder (AUD). Tracking how often one drinks at this level is essential, as it can serve as an early warning sign of dependency.
Analyzing drinking frequency requires more than just counting days; it involves understanding the context and intent behind each drinking session. For example, someone who drinks heavily every weekend may not drink daily, but the binge-drinking pattern still poses serious health risks. The World Health Organization (WHO) highlights that binge drinking, defined as consuming 60 grams or more of pure alcohol on at least one occasion weekly, is a strong predictor of AUD. This distinction underscores that alcoholism isn’t solely about daily drinking—it’s about the intensity and regularity of consumption, even if it’s confined to specific periods.
From a practical standpoint, monitoring drinking frequency can be a proactive step toward identifying potential issues. Keep a drinking diary to log not just the quantity but also the circumstances surrounding each drink. Are you drinking to cope with stress, celebrate, or out of habit? Patterns like drinking alone, hiding consumption, or feeling unable to stop once you’ve started are red flags. For younger adults, especially those aged 18–25, even occasional heavy drinking can disrupt brain development and increase long-term risks. Tools like smartphone apps or journals can help track frequency and provide clarity on whether professional intervention is needed.
Comparatively, societal norms often blur the line between social drinking and problematic behavior. In cultures where daily wine with dinner is common, for instance, frequency alone may not indicate alcoholism. However, when drinking escalates beyond cultural norms—such as transitioning from one glass to multiple bottles nightly—it becomes a concern. The key is to assess whether the frequency of drinking interferes with daily life, relationships, or health. Unlike casual drinkers who can take days or weeks off without issue, individuals with AUD often experience cravings or withdrawal symptoms when they attempt to cut back, highlighting the importance of frequency as a diagnostic marker.
Ultimately, the frequency of alcohol consumption is a nuanced indicator of alcoholism, requiring careful observation and self-awareness. While there’s no one-size-fits-all threshold, consistent heavy drinking—whether daily or in concentrated periods—warrants attention. Combining frequency data with other factors like quantity, motivation, and impact on life provides a clearer picture. If you or someone you know drinks heavily multiple times a week, consider it a call to action: seek assessment from a healthcare professional, explore support groups, or implement harm-reduction strategies. Addressing frequency early can prevent the progression to severe AUD and pave the way for healthier habits.
Breathalyzers: Beating the Test After Drinking Alcohol
You may want to see also
Explore related products






![]()
Quantity Consumed: Amount of alcohol intake that defines alcoholic behavior
Alcohol consumption patterns vary widely, but the line between moderate drinking and alcoholism is often drawn by the quantity and frequency of intake. According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA), heavy alcohol use is defined as consuming 4 or more drinks on any day for men, or 3 or more for women. While occasional heavy drinking doesn’t automatically classify someone as an alcoholic, consistent patterns at or above these levels are a red flag. For context, a "standard drink" is 14 grams of pure alcohol—equivalent to 12 ounces of beer (5% ABV), 5 ounces of wine (12% ABV), or 1.5 ounces of distilled spirits (40% ABV). Tracking intake against these benchmarks is the first step in identifying problematic behavior.
Consider the cumulative effect of alcohol consumption over time. The NIAAA also defines at-risk drinking as exceeding weekly limits: more than 14 drinks per week for men and 7 for women. These thresholds are not arbitrary; they are based on research linking higher volumes to increased health risks, including liver disease, cardiovascular problems, and dependency. For example, a man who consumes 5 drinks daily surpasses the weekly limit in just three days, while a woman reaches her threshold in two. Such patterns often precede alcoholism, as the body develops tolerance, requiring more alcohol to achieve the same effect—a hallmark of addiction.
Age and context matter when evaluating quantity. Young adults (ages 18–25) are more likely to engage in binge drinking, defined as 5 or more drinks for men and 4 or more for women in about 2 hours. While not all binge drinkers are alcoholics, this behavior significantly raises the risk of developing alcohol use disorder (AUD) later in life. Conversely, older adults may face unique risks due to metabolism changes and medication interactions, making even moderate drinking (e.g., 1–2 drinks daily) potentially harmful. Tailoring intake guidelines to age and health status is essential for prevention.
Practical tips can help individuals assess and manage their consumption. Keep a drinking diary to log the number of drinks per day and week, comparing totals to recommended limits. Set clear boundaries, such as limiting drinks to 2 per day for men and 1 for women, and incorporating alcohol-free days. For those concerned about their intake, gradual reduction is more sustainable than abrupt cessation. For instance, cutting back by one drink daily can lower dependency risk over time. If self-regulation fails, seeking professional guidance is critical, as untreated heavy drinking often progresses to alcoholism.
The takeaway is clear: quantity consumed is a measurable, actionable indicator of alcoholic behavior. While definitions vary, exceeding established thresholds—whether daily, weekly, or in binge patterns—signals danger. Awareness of these benchmarks, combined with self-monitoring and proactive adjustments, can prevent the slide into addiction. Alcoholism is not solely defined by quantity, but excessive intake is its most visible and modifiable marker.
Wisconsin's Alcohol Distilling: Legal or Not?
You may want to see also
Explore related products



$10 $10



![]()
Dependence Signs: Physical or psychological reliance on alcohol as a key indicator
Alcoholism, clinically referred to as alcohol use disorder (AUD), is often marked by a profound dependence on alcohol, manifesting in both physical and psychological realms. One of the most telling signs is the body’s physical reliance on alcohol to function. For instance, individuals with AUD may experience withdrawal symptoms such as tremors, nausea, sweating, or even seizures when they attempt to stop drinking. These symptoms typically emerge within 6 to 24 hours after the last drink and can persist for days. A key indicator is the need to consume alcohol to alleviate these symptoms, creating a vicious cycle of dependence. For example, someone who requires a morning drink to steady their hands or calm their nerves is likely exhibiting physical dependence.
Psychological reliance on alcohol is equally critical, though often more subtle. It involves an emotional or mental craving for alcohol that overrides rational decision-making. Individuals may find themselves preoccupied with thoughts of drinking, planning their day around alcohol, or feeling anxious when access to it is uncertain. This psychological grip can lead to behaviors like hiding alcohol, lying about consumption, or neglecting responsibilities. For instance, a person might skip a family event because they cannot drink there or prioritize a bar visit over a work deadline. Such patterns reveal how deeply alcohol has embedded itself in their coping mechanisms and daily routines.
Distinguishing between physical and psychological dependence is crucial for understanding the severity of AUD. Physical dependence often requires medical intervention, such as detox programs, to manage withdrawal safely. Psychological dependence, on the other hand, may benefit from therapy, support groups, or behavioral interventions. For example, cognitive-behavioral therapy (CBT) can help individuals reframe their relationship with alcohol, while medications like naltrexone or acamprosate can reduce cravings. Combining both approaches is often the most effective strategy for long-term recovery.
Practical tips for identifying dependence include monitoring drinking patterns and noting any inability to cut back despite repeated attempts. Keep a journal to track consumption, withdrawal symptoms, and emotional triggers. If you notice a compulsive need to drink—whether to avoid physical discomfort or to cope with stress—seek professional help. Early intervention can prevent the progression of AUD. For instance, limiting alcohol intake to moderate levels (up to one drink per day for women and two for men) can reduce the risk of developing dependence. However, for those already struggling, abstinence may be the safest path.
In summary, dependence signs—whether physical or psychological—are red flags that should not be ignored. Physical reliance often manifests through withdrawal symptoms, while psychological dependence reveals itself through obsessive thoughts and behaviors centered around alcohol. Addressing these signs requires tailored strategies, from medical detox to therapeutic interventions. By recognizing these indicators early and taking proactive steps, individuals can reclaim control over their lives and break free from the chains of alcoholism.
Alcohol-Related Hives: What You Need to Know
You may want to see also
Explore related products




![]()
Negative Consequences: Continued drinking despite harmful personal, social, or health impacts
One of the most glaring red flags of alcoholism is the inability to stop drinking despite clear and mounting negative consequences. This isn’t about occasional overindulgence followed by regret; it’s a persistent pattern where alcohol takes precedence over personal well-being, relationships, and even physical health. For instance, someone might continue drinking heavily despite repeated blackouts, liver function tests showing elevated enzymes (above 50 U/L for ALT/AST), or a doctor’s warning about early cirrhosis. The World Health Organization notes that alcohol-related liver disease is a leading cause of alcohol-attributable deaths globally, yet many individuals ignore these alarms, prioritizing the temporary escape alcohol provides over long-term survival.
Consider the social toll: alcoholism often fractures relationships, yet the affected individual remains unable to curb their drinking. A spouse might threaten divorce after discovering hidden bottles or unpaid bills, or a friend might sever ties after being humiliated by drunken behavior at a public event. Despite these losses, the person with alcoholism may rationalize their actions ("They don’t understand me") or shift blame ("It’s their fault for overreacting"), all while continuing to drink. This denial mechanism, often fueled by cognitive dissonance, allows the behavior to persist even as the social support network crumbles.
Health impacts are equally stark, yet frequently overlooked until irreversible damage occurs. Chronic heavy drinking (defined as 15 drinks or more per week for men, 8 or more for women) increases the risk of hypertension, cardiovascular disease, and certain cancers, including liver, breast, and esophageal cancer. For example, a 45-year-old man with a 20-year drinking history might experience atrial fibrillation or pancreatitis but still refuse to cut back, dismissing symptoms as "temporary" or self-medicating with more alcohol. The National Institute on Alcohol Abuse and Alcoholism emphasizes that even moderate drinkers who escalate to heavy use face a 3-fold increased risk of alcohol-related emergencies, yet behavioral change remains elusive.
Breaking this cycle requires more than willpower; it demands structured intervention. Cognitive-behavioral therapy (CBT) can help individuals identify triggers and develop coping strategies, while medications like naltrexone or disulfiram can reduce cravings or induce aversive reactions to alcohol. Support groups such as Alcoholics Anonymous provide accountability, though only 20-30% of attendees achieve long-term sobriety, underscoring the need for personalized treatment plans. Practical steps include setting small, measurable goals (e.g., reducing daily intake by 2 drinks weekly) and leveraging digital tools like sobriety apps that track progress and offer motivational reminders.
Ultimately, the hallmark of alcoholism isn’t just drinking excessively—it’s the refusal to stop despite undeniable harm. This behavior isn’t a moral failing but a symptom of a complex disorder rooted in biology, psychology, and environment. Recognizing the signs early, such as drinking to cope with stress or hiding consumption from loved ones, can prevent escalation. For those already entangled, acknowledging the problem is the first step; seeking professional help is the next. The path to recovery is arduous, but with the right resources, it’s possible to reclaim a life overshadowed by alcohol’s grip.
Muscle Twitching and Alcohol Withdrawal: Understanding the Connection
You may want to see also
![]()
Withdrawal Symptoms: Experiencing withdrawal effects when alcohol consumption is reduced or stopped
Withdrawal symptoms are the body's physical and emotional response to the abrupt cessation or reduction of alcohol intake after prolonged and excessive use. These symptoms can range from mild to severe, depending on the individual's level of dependence, duration of alcohol use, and overall health. For instance, a person who consumes more than 14 drinks per week (for men) or 7 drinks per week (for women) over several years is at a higher risk of experiencing withdrawal symptoms when they attempt to quit or cut back.
Recognizing the Signs: What to Look For
Withdrawal symptoms typically begin within 6 to 24 hours after the last drink and can peak between 24 to 72 hours. Mild symptoms include anxiety, tremors, insomnia, and nausea. More severe cases may involve hallucinations, seizures, or delirium tremens (DTs), a life-threatening condition characterized by confusion, rapid heartbeat, and fever. For example, a 45-year-old man who has been drinking a bottle of whiskey daily for a decade might experience DTs if he stops abruptly without medical supervision. Recognizing these signs early is crucial, as untreated severe withdrawal can be fatal.
Managing Withdrawal: Practical Steps and Cautions
If you or someone you know is experiencing withdrawal, gradual reduction under medical supervision is often safer than quitting cold turkey. Medications like benzodiazepines can help manage symptoms, but they should only be used under a doctor’s guidance. For mild cases, staying hydrated, eating balanced meals, and engaging in light physical activity can ease discomfort. However, never attempt to manage severe withdrawal at home—seek immediate medical attention if symptoms like seizures or severe confusion occur. For instance, a 30-year-old woman with a history of moderate drinking (3–4 drinks daily) might manage her withdrawal with outpatient support, while a 50-year-old man with a heavier drinking habit would likely require inpatient care.
The Role of Professional Support: Why It’s Essential
Professional treatment programs offer a structured environment to address both physical and psychological aspects of withdrawal. Detox centers provide medical monitoring, therapy, and medications to ensure safety and comfort. For example, a study published in the *Journal of Addiction Medicine* found that individuals who underwent medically supervised detox had a 50% higher success rate in maintaining sobriety compared to those who attempted to quit on their own. Support groups like Alcoholics Anonymous (AA) can also provide ongoing encouragement and accountability, reducing the risk of relapse.
Long-Term Takeaway: Withdrawal as a Turning Point
Experiencing withdrawal is often a stark reminder of the body’s dependence on alcohol, but it can also serve as a critical turning point toward recovery. By understanding the risks and seeking appropriate help, individuals can navigate this challenging phase safely. For instance, a 28-year-old college graduate who binge drinks on weekends might use withdrawal symptoms as a wake-up call to reassess their relationship with alcohol. Ultimately, withdrawal is not just a physical hurdle but an opportunity to reclaim control and pursue a healthier, alcohol-free life.
Excessive Alcohol's Impact: How Drinking Harms Your Heart Health
You may want to see also
Frequently asked questions
Alcoholism, also known as alcohol use disorder (AUD), is classified as a chronic and often relapsing condition characterized by an impaired ability to stop or control alcohol use despite adverse social, occupational, or health consequences. It is diagnosed based on criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
There is no fixed number of drinks per day that universally classifies someone as an alcoholic. However, heavy drinking is defined as consuming 4 or more drinks on any day for men, or 3 or more for women. Consistent heavy drinking or an inability to stop despite negative consequences may indicate alcoholism.
Yes, someone can be classified as an alcoholic even if they only drink on weekends. Binge drinking (5 or more drinks for men, 4 or more for women in about 2 hours) or an inability to control alcohol intake during those times, coupled with negative consequences, can still meet the criteria for alcoholism.
Signs of alcoholism include an inability to limit drinking, spending a lot of time drinking or recovering from its effects, cravings, neglecting responsibilities, continued drinking despite relationship or health problems, tolerance (needing more to feel the same effect), and withdrawal symptoms when not drinking.



















