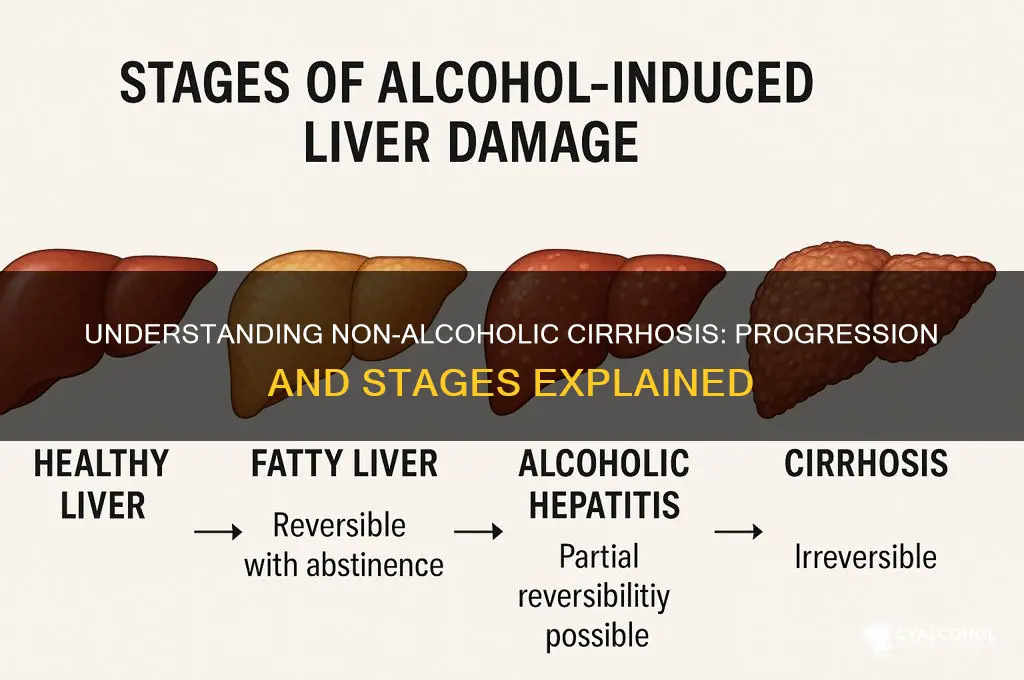
Non-alcoholic cirrhosis, a chronic liver condition, progresses through distinct stages, each marked by increasing severity and irreversible damage to liver tissue. The early stage, often asymptomatic, involves inflammation and mild fibrosis, where the liver begins to scar due to persistent injury from causes like non-alcoholic fatty liver disease (NAFLD). As the condition advances to the second stage, fibrosis worsens, leading to more extensive scarring and impaired liver function. The third stage, known as cirrhosis, is characterized by severe scarring, nodule formation, and significant loss of liver function, often accompanied by complications such as portal hypertension, ascites, and liver failure. Understanding these stages is crucial for early detection, intervention, and management to prevent further deterioration and improve patient outcomes.
| Characteristics | Values |
|---|---|
| Stage 1: Simple Steatosis | - Mild fat accumulation in liver cells. - No significant inflammation or fibrosis. - Often asymptomatic. - Reversible with lifestyle changes. |
| Stage 2: Steatohepatitis (NASH) | - Fat accumulation + inflammation. - Liver cells begin to die. - Mild to moderate fibrosis may develop. - Risk of progression increases. |
| Stage 3: Fibrosis | - Extensive scarring (fibrosis) around liver tissue. - Liver function starts to decline. - Symptoms may include fatigue, weakness, and mild jaundice. - Still potentially reversible with treatment. |
| Stage 4: Cirrhosis | - Severe scarring, leading to liver dysfunction. - Symptoms include ascites, jaundice, bleeding varices, and confusion. - High risk of liver failure, cancer, or death. - Not reversible; management focuses on preventing complications. |
| Progression Factors | Obesity, diabetes, metabolic syndrome, insulin resistance, and genetic predisposition. |
| Diagnosis Methods | Liver biopsy, imaging (ultrasound, MRI), blood tests (liver enzymes, fibrosis markers). |
| Treatment | Lifestyle changes (diet, exercise), medications (e.g., for diabetes, cholesterol), and management of complications. |
Explore related products






What You'll Learn
- Early Stage: Mild fibrosis, often undetected, no symptoms, liver function tests may appear normal
- Progressive Fibrosis: Increasing scar tissue, slight elevation in liver enzymes, possible fatigue or discomfort
- Advanced Fibrosis: Significant scarring, portal hypertension may develop, risk of complications rises
- Compensated Cirrhosis: Liver still functions, symptoms like jaundice or ascites may appear, manageable with care
- Decompensated Cirrhosis: Liver fails, severe complications like bleeding, infections, or hepatic encephalopathy occur
![]()
Early Stage: Mild fibrosis, often undetected, no symptoms, liver function tests may appear normal
In the early stage of non-alcoholic cirrhosis, the liver begins to experience mild fibrosis, a process where healthy liver tissue is gradually replaced by scar tissue. This stage is often undetected because the changes are subtle and do not cause noticeable symptoms. Individuals in this phase typically feel healthy and may not be aware that their liver is undergoing any damage. The absence of symptoms makes early detection challenging, as there is no immediate cause for concern that would prompt medical evaluation.
Mild fibrosis occurs due to prolonged liver inflammation, often caused by conditions like non-alcoholic fatty liver disease (NAFLD) or non-alcoholic steatohepatitis (NASH). At this stage, the liver’s ability to function remains largely intact, and the scarring is minimal. However, if left unaddressed, the fibrosis can progress to more severe stages over time. The liver’s remarkable ability to compensate for damage means it can continue to perform its essential functions despite the early scarring, which further contributes to the lack of detectable symptoms.
Liver function tests, commonly used to assess liver health, may appear normal during this early stage. These tests measure enzymes and proteins in the blood that indicate liver activity, but mild fibrosis often does not elevate these markers significantly. This normal range can give a false sense of security, as it does not reflect the underlying fibrosis. As a result, many individuals remain undiagnosed until the disease progresses to later stages, where symptoms and abnormalities become more apparent.
Despite the lack of symptoms and normal test results, early detection is crucial to prevent further liver damage. Lifestyle modifications, such as adopting a healthy diet, increasing physical activity, and managing weight, can slow or even halt the progression of fibrosis. Regular monitoring by healthcare providers, especially for individuals at risk of NAFLD or NASH, is essential to catch the condition early. Early intervention can significantly improve long-term outcomes and reduce the risk of developing advanced cirrhosis or liver failure.
In summary, the early stage of non-alcoholic cirrhosis is characterized by mild fibrosis that often goes undetected due to the absence of symptoms and normal liver function tests. While the liver remains functional at this stage, the presence of scarring indicates ongoing damage. Awareness, regular medical check-ups, and proactive lifestyle changes are key to managing this stage effectively and preventing further deterioration of liver health.
Exploring Alcoholics Anonymous Presence Across Cities Worldwide
You may want to see also
Explore related products






![]()
Progressive Fibrosis: Increasing scar tissue, slight elevation in liver enzymes, possible fatigue or discomfort
Progressive fibrosis marks a critical stage in the development of non-alcoholic cirrhosis, characterized by the gradual accumulation of scar tissue (fibrosis) in the liver. At this stage, the liver’s ability to function optimally begins to decline as healthy liver tissue is replaced by non-functional scar tissue. This process is often driven by ongoing liver injury, which can result from conditions like non-alcoholic fatty liver disease (NAFLD) or non-alcoholic steatohepatitis (NASH). The increasing fibrosis disrupts the liver’s architecture, impairing its ability to filter toxins, regulate blood composition, and produce essential proteins. While the liver is remarkably resilient and can compensate for some damage, progressive fibrosis signals a worsening condition that requires immediate attention.
One of the key indicators of progressive fibrosis is a slight elevation in liver enzymes, particularly alanine transaminase (ALT) and aspartate transaminase (AST). These enzymes are released into the bloodstream when liver cells are damaged, and their elevated levels serve as a warning sign of ongoing liver injury. Blood tests to monitor these enzymes are crucial for detecting progression, as symptoms at this stage may still be subtle or absent. Patients and healthcare providers must remain vigilant, as persistent enzyme elevation can indicate continued liver damage and the need for intervention to halt or slow the fibrotic process.
Fatigue and discomfort are common symptoms experienced during progressive fibrosis, though they are often nonspecific and may be attributed to other causes. Fatigue can arise from the liver’s reduced ability to metabolize nutrients and toxins efficiently, leading to systemic effects on energy levels. Discomfort, typically felt in the upper right abdomen, may occur due to liver enlargement or inflammation. These symptoms, while not always severe, should not be ignored, as they can signify the liver’s struggle to cope with increasing fibrosis. Recognizing and addressing these signs early is essential to prevent further progression to more advanced stages of liver disease.
Managing progressive fibrosis involves a multifaceted approach aimed at halting the accumulation of scar tissue and addressing the underlying causes of liver injury. Lifestyle modifications, such as adopting a healthy diet, increasing physical activity, and achieving weight loss in cases of obesity, are foundational. These changes can reduce fat accumulation in the liver and decrease inflammation, thereby slowing fibrosis progression. Additionally, managing comorbid conditions like diabetes, hypertension, and dyslipidemia is critical, as these can exacerbate liver damage. Medications targeting specific pathways of liver injury, such as those under investigation for NASH, may also play a role in treatment.
Regular monitoring is essential for individuals with progressive fibrosis to assess disease progression and the effectiveness of interventions. Non-invasive tests, including elastography (e.g., FibroScan) and serum biomarkers, are increasingly used to evaluate fibrosis severity without the need for liver biopsy. These tools allow healthcare providers to track changes in liver stiffness and adjust treatment plans accordingly. Early detection and proactive management during the progressive fibrosis stage can significantly improve outcomes, potentially preventing the development of cirrhosis and its life-threatening complications.
Unveiling White Claw's Alcohol Base: A Comprehensive Guide to Its Ingredients
You may want to see also
Explore related products






![]()
Advanced Fibrosis: Significant scarring, portal hypertension may develop, risk of complications rises
Advanced fibrosis represents a critical stage in the progression of non-alcoholic cirrhosis, characterized by significant scarring of the liver tissue. At this stage, the liver’s ability to function is severely compromised due to extensive fibrosis, which replaces healthy liver cells with non-functional scar tissue. This scarring disrupts the liver’s architecture and impairs its ability to perform essential functions such as detoxification, protein synthesis, and bile production. Patients with advanced fibrosis are at a tipping point where the liver damage is still potentially reversible with aggressive intervention, but without treatment, it can progress to irreversible cirrhosis.
One of the most concerning developments in advanced fibrosis is the onset of portal hypertension, a condition where the blood pressure within the portal vein (which carries blood from the digestive organs to the liver) increases significantly. This occurs because the scarred liver tissue obstructs the normal flow of blood, forcing it to back up and increase pressure in the portal system. Portal hypertension can lead to severe complications, including the formation of varices (enlarged veins) in the esophagus and stomach, which are at risk of rupturing and causing life-threatening bleeding. Additionally, it can result in ascites (fluid accumulation in the abdomen) and hepatic encephalopathy (cognitive impairment due to toxin buildup in the brain).
The risk of complications rises dramatically in advanced fibrosis due to the liver’s diminished capacity to regulate bodily functions. Patients may experience fatigue, weakness, and unexplained weight loss as the liver struggles to meet the body’s metabolic demands. Jaundice (yellowing of the skin and eyes) may also occur due to the liver’s inability to process bilirubin effectively. Furthermore, the immune system becomes compromised, increasing susceptibility to infections. Advanced fibrosis also elevates the risk of hepatocellular carcinoma (liver cancer), as the chronic inflammation and cell turnover create an environment conducive to malignant transformation.
Management of advanced fibrosis focuses on halting disease progression and preventing complications. Lifestyle modifications, such as adopting a low-sodium diet to manage ascites and avoiding alcohol to prevent further liver damage, are essential. Medications may be prescribed to reduce portal hypertension, manage fluid retention, and address specific complications like variceal bleeding. Regular monitoring, including imaging studies and blood tests, is critical to assess liver function and detect early signs of cirrhosis or cancer. In some cases, emerging therapies targeting fibrosis pathways may be considered to slow or reverse scarring.
Early intervention is key in advanced fibrosis, as it represents the last opportunity to prevent irreversible cirrhosis. Patients must work closely with hepatologists to develop a comprehensive treatment plan tailored to their condition. Addressing underlying risk factors, such as obesity, insulin resistance, and metabolic syndrome, is also crucial in slowing disease progression. While advanced fibrosis is a serious condition, timely and aggressive management can significantly improve outcomes and reduce the risk of life-threatening complications.
Understanding BAC: What Constitutes Over the Legal Alcohol Limit?
You may want to see also
Explore related products






![]()
Compensated Cirrhosis: Liver still functions, symptoms like jaundice or ascites may appear, manageable with care
Compensated Cirrhosis represents an early stage of liver damage where the organ, despite scarring, continues to perform its essential functions. This phase is characterized by the liver’s ability to compensate for the fibrosis and nodular regeneration, allowing it to maintain adequate metabolic, synthetic, and detoxification processes. Patients in this stage often remain asymptomatic or experience mild, nonspecific symptoms, making it a critical period for intervention to prevent progression. Early detection through routine liver function tests, imaging, or fibrosis markers can help identify compensated cirrhosis before more severe complications arise.
Symptoms in compensated cirrhosis, when present, are often subtle and may include jaundice, fatigue, or mild abdominal discomfort. Jaundice, characterized by yellowing of the skin and eyes, occurs due to the liver’s reduced ability to process bilirubin, a byproduct of red blood cell breakdown. Ascites, or fluid accumulation in the abdomen, may also appear in some cases, though it is less common in this stage compared to decompensated cirrhosis. Other signs, such as spider angiomas (small blood vessels visible on the skin) or palmar erythema (reddening of the palms), may indicate underlying liver dysfunction. Recognizing these symptoms early is crucial for timely management.
Management of compensated cirrhosis focuses on halting disease progression, treating underlying causes, and preventing complications. Lifestyle modifications, such as adopting a low-sodium diet to prevent fluid retention, avoiding alcohol, and maintaining a healthy weight, are fundamental. Medications may be prescribed to manage specific symptoms or conditions, such as diuretics for mild ascites or beta-blockers to reduce portal hypertension. Regular monitoring, including liver function tests and imaging, is essential to assess disease stability and detect early signs of decompensation. Vaccinations against hepatitis A, B, and pneumococcal infections are also recommended to protect liver health.
Patient education plays a pivotal role in managing compensated cirrhosis, as adherence to treatment plans and lifestyle changes significantly impacts outcomes. Individuals must understand the importance of avoiding hepatotoxic substances, including certain medications and herbal supplements, and the risks associated with untreated cirrhosis. Support from healthcare providers, including hepatologists, dietitians, and counselors, can help patients navigate the challenges of living with a chronic liver condition. Early intervention and proactive care during this stage can delay or even prevent the transition to decompensated cirrhosis, improving long-term prognosis and quality of life.
In summary, compensated cirrhosis is a manageable stage of liver disease where the organ retains sufficient function despite scarring. While symptoms like jaundice or ascites may appear, they are often mild and can be controlled with appropriate care. A multidisciplinary approach, including lifestyle adjustments, medical therapy, and regular monitoring, is key to maintaining liver health and preventing disease progression. Awareness and early intervention are critical to optimizing outcomes for individuals with compensated cirrhosis.
Recovering After Alcohol-Induced Vomiting: Essential Steps for Relief and Recovery
You may want to see also
Explore related products




![]()
Decompensated Cirrhosis: Liver fails, severe complications like bleeding, infections, or hepatic encephalopathy occur
Decompensated cirrhosis represents the most advanced and severe stage of non-alcoholic cirrhosis, where the liver’s function deteriorates to the point of failure. At this stage, the liver can no longer compensate for the damage, leading to life-threatening complications. The hallmark of decompensated cirrhosis is the onset of severe symptoms and complications that significantly impact the patient’s quality of life and survival. These complications arise due to the liver’s inability to perform its critical functions, such as filtering toxins, regulating blood clotting, and producing essential proteins.
One of the most common and dangerous complications of decompensated cirrhosis is bleeding, particularly from esophageal varices. These are enlarged veins in the esophagus that develop as a result of portal hypertension, a condition where blood flow through the liver is obstructed. When these varices rupture, they can cause massive bleeding, which is a medical emergency. Patients may also experience bleeding from other sites, such as the stomach or intestines, due to the liver’s impaired ability to produce clotting factors. Immediate medical intervention, including endoscopic treatments and medications to reduce portal pressure, is often required to manage these bleeding episodes.
Infections are another severe complication in decompensated cirrhosis, as the liver plays a crucial role in immune function. Patients become highly susceptible to bacterial, fungal, and viral infections, particularly spontaneous bacterial peritonitis (SBP), a life-threatening infection of the abdominal fluid. The risk of infections is further exacerbated by the accumulation of fluid in the abdomen (ascites), which provides a breeding ground for pathogens. Prophylactic antibiotics and prompt treatment of infections are essential to prevent complications and reduce mortality in these patients.
Hepatic encephalopathy is a devastating neurological complication of decompensated cirrhosis, occurring when the liver fails to remove toxins like ammonia from the blood. These toxins accumulate in the brain, leading to cognitive impairment, confusion, personality changes, and, in severe cases, coma. Management of hepatic encephalopathy involves reducing toxin production through dietary modifications, medications like lactulose or rifaximin, and addressing underlying triggers such as infections or electrolyte imbalances. Despite treatment, hepatic encephalopathy significantly worsens the prognosis and quality of life for patients with decompensated cirrhosis.
The progression to decompensated cirrhosis necessitates a multidisciplinary approach to care, often involving hepatologists, intensive care specialists, and transplant surgeons. Liver transplantation remains the only curative option for patients with end-stage liver disease, but it is limited by organ availability and the patient’s overall health. Palliative care may also be integrated to address symptoms and improve the patient’s comfort. Early recognition of decompensated cirrhosis and aggressive management of its complications are critical to prolong survival and maintain the best possible quality of life for affected individuals.
Alcohol's Mental Toll: Uncovering the Hidden Dangers of Drinking
You may want to see also
Frequently asked questions
The early stages of non-alcoholic cirrhosis (often referred to as non-alcoholic fatty liver disease, NAFLD) include simple fatty liver (steatosis), where fat accumulates in the liver without significant inflammation or scarring. This stage is usually asymptomatic and often reversible with lifestyle changes.
In the intermediate stages, NAFLD progresses to non-alcoholic steatohepatitis (NASH), where inflammation and liver cell damage occur alongside fat accumulation. This can lead to fibrosis, the formation of scar tissue in the liver, which may still be reversible if detected and managed early.
The advanced stage is characterized by cirrhosis, where extensive scarring replaces healthy liver tissue, leading to liver dysfunction. Symptoms may include jaundice, fluid retention, bleeding varices, and liver failure. At this stage, the damage is often irreversible, and management focuses on preventing complications and liver transplantation if necessary.