Alcohol and surgery are a dangerous combination. Drinking alcohol before surgery can lead to several health complications, including increased bleeding, interference with anesthesia, delayed recovery, and even death. Alcohol can affect the functioning of the liver, which processes both alcohol and anesthesia, meaning doctors may need to adjust the dosage of anesthesia. This can affect the efficacy and safety of anesthesia during surgery. Alcohol also increases the risk of aspiration, where a person may vomit the contents of their stomach, which could then travel to the lungs. This can be fatal. For people with alcohol use disorder, surgery can be a trigger for a relapse, as the stress and pain associated with surgery may make alcohol seem appealing. Given these risks, it is important for patients to disclose their alcohol consumption to their healthcare team so that doctors can help them withdraw safely and minimize the risks of complications during surgery.
| Characteristics | Values |
|---|---|
| Effect on anaesthesia | Alcohol can affect how the body responds to anaesthesia, causing breathing problems and other complications during surgery. |
| Effect on bleeding | Alcohol increases the risk of postoperative bleeding and can delay healing. |
| Effect on recovery | Alcohol can prolong recovery time, increase the risk of infection, and cause liver, pancreas, and nervous system problems. |
| Effect on judgement | Alcohol can impair judgement and increase the likelihood of making poor decisions about postoperative care. |
| Withdrawal | Alcohol withdrawal symptoms can increase the risk of complications during surgery and recovery. |
| Dosage adjustment | Anaesthesiologists may need to adjust the dosage of anaesthesia if the patient has alcohol in their system or is a chronic alcohol user. |
| Hospital stay | Patients who consume alcohol may require more monitoring and care during their recovery, prolonging their hospital stay. |
| Relapse risk | Surgery can be a trigger for relapse for people with alcohol use disorder due to the associated stress and pain. |
Explore related products






What You'll Learn
- Alcohol use increases the risk of postoperative bleeding, infection, and poor immune response
- Anaesthesia and alcohol both affect the liver, heart rate, and blood circulation
- Alcohol can cause psychomotor impairment, impacting informed consent
- Alcohol withdrawal syndrome can cause severe complications and increase the risk of relapse
- Alcohol can delay gastric emptying, increasing the risk of pulmonary aspiration
![]()
Alcohol use increases the risk of postoperative bleeding, infection, and poor immune response
Alcohol can cause bleeding by slowing the clotting process, which can delay the healing of surgical wounds. It can also increase the risk of infection in the surgical site, respiratory system, or urinary tract. A poor immune response to infection can lead to sepsis and septic shock, which can be life-threatening. Alcohol can also cause problems with the liver, pancreas, and nervous system, which can make it harder to recover from surgery.
Chronic alcohol ingestion has been shown to deplete pulmonary glutathione, reducing surfactant production and altering epithelial cell permeability. This may explain the increased susceptibility to acute lung injury in alcohol abusers, especially after thoracic surgery. Underlying cardiac disease can also limit the ability to meet the increased metabolic requirement after major surgery, and arrhythmias and acute coronary syndrome are more common post-operation.
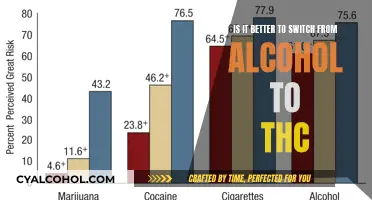
The risk of postoperative complications increases with alcohol consumption. Studies have shown that at an intake of more than 2 to 3 alcoholic units per day, the complication rate increases by about 50%. This rate increases by 300% for patients drinking more than 5 units per day. Typical complications include infections, cardiopulmonary issues, and bleeding.
Alcohol can also cause psychomotor impairment, making it difficult to obtain informed consent for surgery. Patients suffering from chronic alcohol misuse may present with acute deterioration and require intensive care. Recovery may also be complicated by alcohol withdrawal, with symptoms such as confusion, aggression, and psychomotor impairment.
Alcoholism and Section 8: A Disqualifying Factor?
You may want to see also
Explore related products






![]()
Anaesthesia and alcohol both affect the liver, heart rate, and blood circulation
Alcohol and anaesthesia both affect the liver, heart rate, and blood circulation. Anaesthesia involves powerful drugs that suppress functions such as breathing, heart rate, and blood circulation. Alcohol affects the same body systems. As both substances are metabolized in the liver, the organ may not be able to keep up, leading to potential overload. This can be particularly dangerous for those with liver disease.
Chronic alcohol misuse can lead to an increased dosage requirement for general anaesthetic agents. This is due to enzyme induction and the development of cross-tolerance. Additionally, elevated blood ethanol concentration can increase sensitivity to other drugs, impacting the effectiveness of anaesthesia.
The interaction between alcohol and anaesthesia can have several adverse effects. Both can cause nausea and vomiting, increasing the risk of aspiration, which can be fatal. Alcohol misuse can also lead to electrolyte disturbances, glucose abnormalities, and impaired cardiac function, all of which can increase the risk of cardiac events during surgery, especially for those with pre-existing heart problems.
Alcohol misuse can also cause psychomotor impairment, confusion, aggression, and acute confusion or delirium post-surgery. This can complicate the recovery process, especially if there are alcohol-related complications during the procedure. Therefore, it is generally recommended to abstain from alcohol for at least two weeks after surgery.
Alcoholic Cirrhosis: A More Sinister Threat?
You may want to see also
Explore related products
$80.15 $249.99





![]()
Alcohol can cause psychomotor impairment, impacting informed consent
Alcohol consumption before surgery can cause several complications, including an increased risk of postoperative bleeding, infection, and acute confusion or delirium. It is therefore recommended that patients refrain from drinking alcohol for at least 48 hours before surgery. However, this may not be feasible for chronic alcoholics, and special considerations may need to be made.
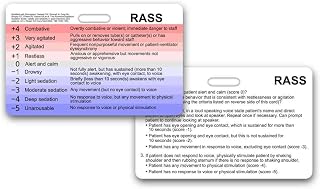
Alcohol can cause psychomotor impairment, which can impact a patient's ability to give informed consent for surgery. Even in the absence of a depressed conscious level, alcohol consumption can produce psychomotor impairment equivalent to commonly used sedation regimens. This means that the patient may need to be treated as if they lack the capacity to make an informed choice. Confusion, aggression, and impaired judgment can put the patient and others at risk.
The effects of alcohol on psychomotor performance have been studied in both heavy binge social drinkers and drinkers with and without alcohol use disorder (AUD). These studies have found that alcohol impairs performance on various tasks, including motor coordination, reaction time, and information processing. The specific effects can vary depending on individual differences, such as the amount of alcohol consumed, the rate of consumption, recent food intake, and the individual's size and weight.
In the context of surgery, if a patient is intoxicated, the anesthesiologist may need to adjust the dosage of anesthesia. This can be challenging, especially if the patient has underlying cardiac issues. Additionally, the presence of alcohol in the system can increase the risk of aspiration (inhaling vomit), which can be potentially fatal.
Overall, alcohol can significantly impact a patient's ability to give informed consent due to psychomotor impairment, confusion, and impaired judgment. It is crucial to consider these factors when obtaining consent for surgery, especially in the case of chronic alcohol misuse, to ensure the patient's safety and well-being.
BTMS-25: Comedogenic Concern or Clear Skin?
You may want to see also
Explore related products






![]()
Alcohol withdrawal syndrome can cause severe complications and increase the risk of relapse
Alcohol withdrawal syndrome (AWS) is a range of symptoms that can occur when a person stops or significantly reduces alcohol intake after long-term use. AWS typically affects people with alcohol use disorder (AUD), which is the most common substance use disorder in the United States. While most cases of AWS are mild, severe presentations can lead to life-threatening complications and an increased risk of relapse.
The severity of AWS symptoms can vary greatly, ranging from minor symptoms such as insomnia, tremulousness, and mild anxiety to severe complications such as withdrawal seizures, delirium tremens, and alcohol hallucinosis. The risk of relapse is also heightened during AWS, as individuals may experience intense cravings and a decreased ability to control their drinking.
The symptoms of AWS typically begin within six to 24 hours of stopping or significantly decreasing heavy, long-term alcohol use. Mild symptoms may appear within the first six to 12 hours, including headache, mild anxiety, and insomnia. Within 24 hours, hallucinations may occur, depending on the severity of withdrawal. Between 24 to 72 hours after the last drink, symptoms typically peak for most individuals with mild to moderate withdrawal and begin to resolve. However, for those with severe or complicated withdrawal, the risk of seizures is highest during this time frame. Delirium tremens may also appear from 48 to 72 hours after the last drink.
The treatment of AWS involves managing withdrawal symptoms and preventing complications. Healthcare providers use a physical exam, symptoms, alcohol use history, and medical history to diagnose AWS. Blood tests and an EKG (electrocardiogram) may also be recommended to check for health complications associated with alcohol use disorder, such as dehydration, electrolyte imbalances, liver function issues, heart issues, and gastrointestinal bleeding.
The Clinical Institute Withdrawal Assessment of Alcohol Scale, Revised (CIWA-Ar) is a useful tool for monitoring the effectiveness of treatment regimens and guiding the administration of medication. Benzodiazepines are the agents of choice for pharmacological treatment, administered on a fixed or symptom-triggered schedule. Carbamazepine is an alternative for mild to moderate AWS. Additionally, beta-blockers, clonidine, and phenytoin may be used as adjuncts to benzodiazepines in treating AWS complications.
ETG and Peth: FDA-Approved Alcohol Biomarkers?
You may want to see also
Explore related products






![]()
Alcohol can delay gastric emptying, increasing the risk of pulmonary aspiration
Alcohol can have a detrimental impact on the body's systems, including the heart, lungs, liver, pancreas, and nervous system. It can also increase the risk of postoperative bleeding, infection, and acute confusion or delirium. These complications can prolong the recovery process and, in some cases, lead to life-threatening conditions such as sepsis and septic shock.
When it comes to surgery, it is essential to consider the effects of alcohol on gastric emptying and the subsequent risk of pulmonary aspiration. Pulmonary aspiration is a serious complication that can occur during the perioperative period, affecting about 1 in every 2,000–3,000 surgeries. It is caused by the inhalation of gastric or oropharyngeal contents into the larynx and lower respiratory tract, which can lead to a wide range of clinical sequelae and, in some cases, even death.
Alcohol consumption can delay gastric emptying, which increases the risk of pulmonary aspiration. This delay in gastric emptying means that the stomach takes longer to empty its contents, leading to a higher risk of aspiration during anesthesia. In fact, a hangover can significantly impair gastric emptying, and patients who have consumed excessive amounts of alcohol the night before surgery have been observed to have aspirations intraop. Therefore, it is standard protocol to recommend abstinence from alcohol for a certain period before surgery, usually 48 hours, to reduce the risk of complications.
The risk of pulmonary aspiration is not limited to the presence of solid food in the stomach but also extends to liquids. While the aspiration of clear liquids is often clinically insignificant, it can still pose a risk, especially when combined with alcohol consumption. Alcohol affects the body's ability to manage the aspiration process, increasing the likelihood of negative outcomes. Therefore, it is crucial for patients to adhere to preoperative fasting guidelines and for anesthesiologists to carefully monitor patients and adjust dosages as needed.
In conclusion, alcohol can delay gastric emptying, which increases the risk of pulmonary aspiration during surgery. This delay can have serious consequences, including increased susceptibility to acute lung injury, especially after thoracic surgery. The anesthesiologist plays a crucial role in managing this risk by considering the patient's alcohol consumption, adjusting anesthesia dosages, and ensuring proper pre-operative assessment and preparation.
Alcohol-Free Planet Hollywood: Costa Rica's Dry Resort
You may want to see also
Frequently asked questions
No, it is not common protocol to sedate alcoholics before surgery anesthesia. However, it is important to disclose recent alcohol consumption to the surgeon or another healthcare professional involved in the surgery. This is because alcohol can affect how the body responds to anesthesia and can cause breathing problems or other complications during surgery.
Alcohol can affect the functioning of the liver, which could mean doctors need to adjust the dosage of anesthesia. This could impact the efficacy and safety of anesthesia during surgery.
Drinking alcohol before surgery can cause several health complications, including increased bleeding, interference with anesthesia, delayed recovery, and an increased risk of death.
It is not recommended to have surgery without stopping drinking as it can increase the risk of complications and death. However, a person with a substance use disorder should not attempt to stop using alcohol abruptly before surgery, as this could lead to alcohol withdrawal syndrome.
Alcoholics can speak with a healthcare professional who can prescribe medications and give advice on how to reduce alcohol consumption safely. Doctors may prescribe medications such as benzodiazepines to ease the symptoms of withdrawal.