The question of whether alcohol acts as an antidepressant or a depressant is a nuanced one, as its effects on the brain and body are complex and multifaceted. Initially, alcohol may produce feelings of relaxation and euphoria, leading some to believe it has antidepressant qualities by temporarily alleviating stress or anxiety. However, alcohol is scientifically classified as a central nervous system depressant, meaning it slows down brain activity, impairs cognitive function, and can exacerbate symptoms of depression over time. Chronic alcohol use can disrupt neurotransmitter balance, particularly affecting serotonin and dopamine, which are crucial for mood regulation, ultimately contributing to or worsening depressive disorders. Thus, while alcohol may provide short-term relief, its long-term effects clearly align it with depressant properties rather than serving as a sustainable or healthy antidepressant.
| Characteristics | Values |
|---|---|
| Classification | Alcohol is primarily classified as a central nervous system (CNS) depressant. |
| Immediate Effects | Initially acts as a sedative, reducing inhibitions and inducing relaxation, which may temporarily alleviate symptoms of anxiety or depression. |
| Long-Term Effects | Prolonged use leads to depressant effects, including slowed brain function, impaired judgment, and increased risk of depression and anxiety disorders. |
| Neurochemical Impact | Enhances GABA (inhibitory neurotransmitter) activity and suppresses glutamate, leading to depressant effects. Temporarily increases dopamine, which can create a short-lived mood lift. |
| Antidepressant Misconception | Alcohol is not an antidepressant. While it may provide temporary relief, it exacerbates underlying mental health issues over time. |
| Withdrawal Effects | Cessation after prolonged use can cause rebound anxiety and depression, reinforcing its depressant nature. |
| Health Risks | Associated with dependence, liver damage, cardiovascular issues, and increased suicide risk, particularly in those with depression. |
| Clinical Consensus | Widely recognized as a depressant by medical and scientific communities, with no therapeutic value for treating depression. |
Explore related products






What You'll Learn
![]()
Alcohol’s Immediate Effects on Mood
Consider the biochemical mechanism: alcohol enhances GABA activity, a neurotransmitter that inhibits brain function, while simultaneously suppressing glutamate, responsible for excitation. This dual action explains why small amounts can induce relaxation and confidence, while larger amounts result in slurred speech, impaired judgment, and mood swings. For instance, a 50-kg individual may experience peak euphoria at 1–1.5 drinks, whereas a 90-kg individual might require 2–2.5 drinks to achieve a similar effect. However, both risk depression and irritability if consumption continues unchecked.
Practical tip: monitor your Blood Alcohol Concentration (BAC) to avoid the depressive phase. A BAC of 0.03–0.05% (achieved with 1–2 drinks in an hour) typically maximizes positive mood effects. Use apps or BAC calculators to track intake, especially if mixing drinks. Avoid drinking on an empty stomach, as food slows alcohol absorption and prolongs the initial euphoric phase. For those prone to anxiety or depression, even small amounts can exacerbate underlying symptoms, so moderation is critical.
Comparatively, alcohol’s mood effects differ sharply from prescribed antidepressants, which stabilize neurotransmitters over time. While SSRIs like fluoxetine take weeks to alleviate depression, alcohol provides instant but fleeting relief, often followed by a crash. This contrast highlights why alcohol is not a substitute for therapeutic treatment. Instead, it’s a temporary mood modifier with inherent risks, particularly for individuals under 25, whose brains are still developing, or those with a history of mental health disorders.
In conclusion, alcohol’s immediate mood effects are a double-edged sword. While low doses can mimic antidepressant properties by boosting dopamine and reducing inhibitions, higher doses depress the central nervous system, leading to negative emotional outcomes. Understanding this duality empowers individuals to make informed choices, balancing temporary mood enhancement with long-term health considerations. Always prioritize moderation and awareness of personal limits to avoid the depressive pitfalls of excessive consumption.
Staging an Alcohol Intervention: A Compassionate Guide to Helping Loved Ones
You may want to see also
Explore related products





![]()
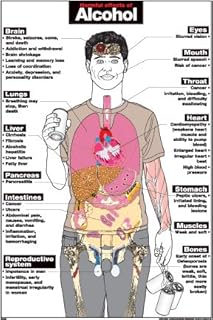
Long-Term Impact on Brain Chemistry
Alcohol's immediate effects might suggest a temporary lift in mood, but its long-term impact on brain chemistry tells a different story. Chronic alcohol use disrupts the delicate balance of neurotransmitters, the brain's chemical messengers. Specifically, it interferes with gamma-aminobutyric acid (GABA), which inhibits brain activity, and glutamate, which excites it. Over time, the brain compensates by reducing GABA receptors and increasing glutamate production, leading to a state of hyperactivity when alcohol is absent. This adaptation explains why long-term users often experience anxiety, irritability, and insomnia during withdrawal—symptoms more akin to a depressant than an antidepressant.
Consider the role of dopamine, the neurotransmitter associated with pleasure and reward. While alcohol initially spikes dopamine levels, chronic use desensitizes the brain’s reward system. This means higher doses are needed to achieve the same effect, a hallmark of tolerance. Over time, the brain produces less dopamine naturally, leaving users feeling flat or depressed when not drinking. For example, a study published in *Neuropsychopharmacology* found that individuals with alcohol use disorder had significantly lower dopamine release in the brain’s reward regions compared to non-users. This biochemical shift underscores alcohol’s depressant nature, as it ultimately diminishes the brain’s ability to experience pleasure without it.
Another critical player in this chemical drama is serotonin, a neurotransmitter linked to mood regulation. Alcohol temporarily increases serotonin release, which can create a fleeting sense of euphoria. However, prolonged exposure depletes serotonin levels, contributing to long-term mood disorders. Research in *Addiction Biology* highlights that chronic alcohol consumption reduces the availability of tryptophan, the amino acid precursor to serotonin, in the brain. This depletion exacerbates symptoms of depression and anxiety, particularly in individuals already predisposed to these conditions. Thus, while alcohol may mimic an antidepressant in the short term, its sustained impact on serotonin pathways reinforces its depressant classification.
Practical steps can mitigate these long-term effects, especially for moderate drinkers. Limiting intake to recommended guidelines—up to one drink per day for women and two for men—can prevent significant disruptions to brain chemistry. Incorporating serotonin-boosting activities like exercise, sunlight exposure, and a diet rich in tryptophan (found in turkey, eggs, and nuts) can also support neurotransmitter balance. For those with a history of heavy use, professional intervention is crucial. Medications like acamprosate, which modulate GABA and glutamate, can help restore equilibrium during recovery. Ultimately, understanding alcohol’s depressant effects on brain chemistry empowers individuals to make informed choices about consumption and seek timely support when needed.
Can You Bring Alcohol to Jones Beach? Rules and Regulations Explained
You may want to see also
Explore related products






![]()
Alcohol vs. Antidepressant Mechanisms
Alcohol's immediate effects often mimic those of an antidepressant, providing a temporary lift in mood and reduction in anxiety. This occurs because alcohol enhances the activity of GABA, a neurotransmitter that inhibits brain activity, leading to relaxation. Simultaneously, it increases dopamine levels, which can induce feelings of pleasure and reward. However, this is a short-lived illusion. While antidepressants work by gradually balancing neurotransmitters like serotonin and norepinephrine over weeks, alcohol disrupts these very systems, leading to long-term imbalances. For instance, chronic alcohol use depletes serotonin, exacerbating depression and anxiety over time. Thus, while alcohol may offer fleeting relief, it fundamentally undermines the brain’s ability to regulate mood effectively.
Consider the dosage and timing differences between alcohol and antidepressants. Antidepressants, such as SSRIs (e.g., fluoxetine), are prescribed in precise doses (typically 20–60 mg daily) and require consistent use for 4–6 weeks to achieve therapeutic effects. Alcohol, on the other hand, is consumed in varying amounts, often without regard for its depressant properties. A single drink may temporarily elevate mood, but repeated use, especially in higher quantities (e.g., 4–5 drinks in one sitting), shifts its role from a pseudo-antidepressant to a depressant, impairing cognitive function and emotional stability. This inconsistency in alcohol consumption not only negates its short-term benefits but also complicates its comparison to the structured, long-term approach of antidepressant therapy.
From a practical standpoint, individuals seeking mood regulation should be cautious about self-medicating with alcohol. For adults over 18, moderate drinking (up to 1 drink per day for women, 2 for men) may seem harmless, but even this can interfere with antidepressant efficacy. For example, combining alcohol with MAOIs (a class of antidepressants) can lead to dangerous spikes in blood pressure. Moreover, alcohol’s depressant effects can counteract the benefits of antidepressants, prolonging recovery. Instead, evidence-based strategies like cognitive-behavioral therapy (CBT) or mindfulness practices offer safer, more sustainable alternatives. These methods address the root causes of mood disorders without the risks associated with alcohol.
A comparative analysis reveals that while alcohol and antidepressants both influence neurotransmitter systems, their mechanisms and outcomes diverge sharply. Antidepressants target specific pathways to restore emotional balance, often requiring professional oversight and patience. Alcohol, in contrast, provides immediate but superficial relief while disrupting the very systems it temporarily enhances. For those under 25, whose brains are still developing, alcohol’s neurotoxic effects can be particularly harmful, increasing the risk of long-term mental health issues. Understanding these distinctions is crucial for making informed decisions about managing mood disorders, emphasizing the need for professional guidance over self-medication.
Vaccination and Alcohol: Should You Avoid Drinking Post-Shot?
You may want to see also
Explore related products





![]()
Depressant Classification Explained
Alcohol's classification as a depressant often surprises those who associate it with social lubrication and temporary euphoria. This paradox stems from a misunderstanding of how depressants function in the brain. Depressants, including alcohol, act primarily on the central nervous system (CNS), slowing down neural activity. This deceleration manifests as reduced inhibitions, sedation, and impaired coordination—hallmarks of alcohol intoxication. While small doses (typically one drink for women, two for men within an hour) might create a stimulating effect due to the release of dopamine, this is a secondary response. The primary mechanism remains depressant, as evidenced by its ability to suppress anxiety, induce sleepiness, and impair cognitive function at higher doses.
Understanding dosage is crucial when dissecting alcohol's depressant nature. The line between stimulation and depression is thin and highly individualized. Factors like body weight, tolerance, and metabolism dictate how quickly and intensely the depressant effects take hold. For instance, a 120-pound individual consuming three standard drinks in two hours will likely experience pronounced depressant symptoms—slurred speech, slowed reaction times, and emotional lability. In contrast, the same dosage might produce milder effects in someone with a higher tolerance. The key takeaway: alcohol’s depressant classification is not negated by its initial stimulating effects; it’s a matter of dosage and individual physiology.
The depressant classification also explains alcohol’s risks, particularly when mixed with other CNS depressants like benzodiazepines or opioids. Combining these substances amplifies their effects, increasing the risk of respiratory depression, coma, or death. For example, mixing alcohol with Xanax (a benzodiazepine) can lead to dangerous over-sedation, even at doses considered safe when taken alone. This synergy underscores the importance of recognizing alcohol’s depressant nature in medical and recreational contexts. Healthcare providers often advise against such combinations, especially for individuals over 65, whose metabolisms may be slower and more susceptible to adverse effects.
Finally, the depressant classification has implications for mental health. While alcohol may temporarily alleviate symptoms of anxiety or depression by slowing neural activity, this relief is short-lived and counterproductive. Chronic use disrupts neurotransmitter balance, exacerbating the very conditions it seems to soothe. For instance, prolonged alcohol consumption depletes serotonin and dopamine, leading to increased anxiety and depressive episodes. This cycle highlights the critical difference between a substance’s immediate effects and its long-term impact—a distinction often overlooked in discussions about alcohol’s role as a depressant.
High Alcohol Intake and Breast Cysts: Unraveling the Connection
You may want to see also
Explore related products






![]()
Risks of Self-Medicating with Alcohol
Alcohol's dual nature as both a central nervous system depressant and a temporary mood elevator often leads individuals to self-medicate for anxiety, depression, or stress. While a drink might offer fleeting relief, this practice carries significant risks that outweigh any perceived benefits.
Alcohol's depressant effects, which slow brain activity and induce relaxation, can initially mask symptoms of anxiety or depression. However, this relief is short-lived. As the body metabolizes alcohol, withdrawal symptoms like increased anxiety, irritability, and insomnia emerge, creating a vicious cycle of dependence. A 2019 study published in the *Journal of Addiction Medicine* found that individuals who self-medicated with alcohol were more likely to experience worsening depression and anxiety over time compared to those who sought professional treatment.
For example, consider a 30-year-old professional experiencing work-related stress. They might turn to a glass of wine after work to unwind. Initially, the alcohol may dull their worries, but over time, they find themselves needing more drinks to achieve the same effect. This escalation can lead to alcohol use disorder (AUD), characterized by cravings, loss of control over drinking, and negative consequences on personal and professional life. The National Institute on Alcohol Abuse and Alcoholism defines low-risk drinking as up to 4 drinks per day for men and 3 for women, but even within these limits, self-medication can lead to psychological dependence.
The risks extend beyond mental health. Chronic alcohol use, even in moderate amounts, can damage the liver, heart, and brain. It increases the risk of cancers, including liver, breast, and esophageal cancer. Furthermore, alcohol interacts negatively with many medications, including antidepressants and anti-anxiety drugs, potentially amplifying their sedative effects or reducing their efficacy. For instance, combining alcohol with benzodiazepines like Xanax can lead to respiratory depression, a life-threatening condition.
Breaking the cycle of self-medication requires addressing the underlying issues driving alcohol use. Cognitive-behavioral therapy (CBT) and mindfulness-based interventions have proven effective in managing anxiety and depression without relying on substances. Support groups, such as Alcoholics Anonymous, provide a community for those struggling with dependence. Practical steps include setting clear limits on drinking (e.g., no more than 2 drinks per occasion), keeping a journal to track drinking patterns and triggers, and seeking professional help when self-regulation fails.
In conclusion, while alcohol may temporarily alleviate emotional pain, its long-term consequences make it a dangerous substitute for proper mental health treatment. Recognizing the risks and seeking evidence-based solutions is crucial for breaking free from the cycle of self-medication and achieving lasting well-being.
Exploring Havasu Falls: Do Visitors Search for Alcohol Nearby?
You may want to see also
Frequently asked questions
No, alcohol is not an antidepressant. While it may temporarily reduce feelings of anxiety or sadness due to its sedative effects, it does not treat depression and can worsen symptoms over time.
Yes, alcohol is a central nervous system depressant. It slows down brain activity, leading to reduced inhibitions, impaired coordination, and sedation.
Alcohol may provide temporary mood elevation due to its effects on neurotransmitters like dopamine, but this is short-lived and can lead to dependence, withdrawal, and long-term mood disorders.
Alcohol’s initial euphoric effects are due to its impact on the brain’s reward system, but its primary action is to depress the central nervous system, leading to slowed reactions, drowsiness, and impaired judgment.
No, alcohol should never be used as a substitute for antidepressant medication. It can interfere with the effectiveness of medications, worsen depression, and increase the risk of addiction and other health problems.