Alcoholic hepatitis is a type of alcoholic liver disease (ALD) that is often caused by excessive alcohol consumption. ALD patients frequently experience malnutrition and deficiencies in vitamins and trace elements, such as zinc, vitamin D, vitamin K, and vitamin B complex, including niacin. Protein deficiency is also common in patients with alcoholic hepatitis, as they may have inadequate protein intake or altered protein metabolism due to liver damage. Nutritional therapy and lifestyle modifications are crucial in managing alcoholic hepatitis and improving liver function, as well as reducing the risk of complications and mortality associated with the disease.
| Characteristics | Values |
|---|---|
| Protein deficiency | Patients with alcoholic hepatitis often have inadequate protein intake |
| Niacin deficiency | Niacin has hepatotoxic potential |
| Zinc deficiency | Linked with reduced fatty acid beta-oxidation, impaired autophagy, and hepatocyte apoptosis |
| Folic acid deficiency | Folic acid deficiency increases alcohol-related injury through activation of CYP 2E1 and increased endoplasmic reticulum stress |
| Thiamine deficiency | Affects 80% of patients with alcohol use disorder |
| Vitamin D deficiency | Very common in patients with chronic liver disease |
| Vitamin K deficiency | Vitamin K deficiency supports liver injury |
Explore related products






What You'll Learn
![]()
Malnutrition is common in alcoholic liver disease
Malnutrition is a common occurrence in alcoholic liver disease (ALD). It is associated with high rates of complications and mortality. Patients with alcoholic liver disease often have inadequate protein intake and may have nutritionally imbalanced fat intake, with excess omega-6 and low omega-3. Diets are also often deficient in micronutrients such as zinc, thiamine, niacin, pyridoxine, folate, and magnesium.
The etiology of malnutrition in ALD patients is complex and includes inadequate dietary intake, abnormal absorption and digestion, increased skeletal and visceral protein catabolism, and abnormal interactions between ethanol and lipid metabolism. Alcohol is a major source of empty calories, and patients with alcoholic liver disease often consume a diet inadequate in protein, and loss of muscle mass is common.
Malnutrition in ALD can also be due to isolated micronutrient deficiency, such as zinc deficiency. Patients with severe alcoholic hepatitis and cirrhosis have the most severe nutritional deficiencies, indicating that advanced disease is associated with more severe malnutrition. Micronutrient depletion is common in alcoholic liver disease, and each deficiency produces specific sequelae. All cirrhotic patients should be screened at baseline for deficiencies of micronutrients and supplemented as needed.
Protein-calorie malnutrition is also common in ALD. A 1986 study of 352 hospitalized veterans with alcoholic liver disease found increased 30-day mortality in patients with severe protein-calorie malnutrition, with mortality rates of 52% and 2% for those with severe and mild malnutrition, respectively. The study also found that as the severity of protein-calorie malnutrition increased, so did the severity of alcoholic liver disease, ascites, and hepatic encephalopathy.
Nutritional therapy is an important part of managing alcoholic liver disease and can improve nutritional status, liver function, and decrease the risk for liver-related complications and mortality. Nutritional support for malnourished patients improves the outcome of hospitalization, surgery, and transplantation and reduces the complications of liver disease and the length of hospital stay.
Calories in Alcohol: 5 Grams Equals How Much?
You may want to see also
Explore related products





![]()
Alcohol is a source of empty calories
Alcoholic beverages primarily consist of water, pure alcohol (ethanol), and variable amounts of sugars and carbohydrates. Alcohol has almost the same amount of calories as fat, with a pint of lager containing roughly the same amount of calories as a standard slice of pizza. However, unlike food, alcoholic drinks provide empty calories, meaning they have no nutritional value because they are consumed in addition to the calories your body needs.
Alcoholic drinks are usually additional to the calories consumed in the rest of one's diet, and the body does not digest the calories from alcohol efficiently. While the body can store many nutrients, protein, carbohydrates, and fat, it needs to prioritise getting rid of alcohol, which is toxic, and this interrupts other processes like absorbing nutrients and processing fat. This can lead to malnutrition, which is a common finding in alcohol use disorders and is associated with the prognosis of patients with alcoholic liver disease (ALD).
Malnutrition in ALD patients is multifactorial and complex and includes inadequate dietary intake, abnormal absorption and digestion, increased skeletal and visceral protein catabolism, and abnormal interactions between ethanol and lipid metabolism. Patients with severe alcoholic hepatitis (AH) and cirrhosis have the most severe nutritional deficiencies, indicating that advanced disease is associated with more severe malnutrition. Nutritional therapy is important in the management of ascites and hepatic encephalopathy as liver failure progresses.
Studies have shown that virtually 100% of patients with AH have some degree of malnutrition, which is generally defined by a state of inadequate protein and/or calorie intake, resulting in sarcopenia. Patients with AH often consume a diet inadequate in protein, and loss of muscle mass is common in AH. They also frequently show deficiencies in vitamins and trace elements, increasing the likelihood of anemia and altered cognitive status.
To avoid the extra calories from alcohol, it is recommended to stick to low-risk drinking guidelines, such as no more than 14 units of alcohol a week for both men and women, with several drink-free days and no bingeing.
IR Spectroscopy: Detecting Alcohols and Amines
You may want to see also
Explore related products





![]()
Protein-calorie malnutrition increases mortality
Malnutrition is a common complication of alcoholic liver disease (ALD) and alcohol-associated hepatitis (AH). It is associated with the prognosis of patients with alcoholic liver disease (ALD). Protein-calorie malnutrition is a frequent complication of ALD, and its severity correlates with the severity of the disease.
Protein-calorie malnutrition is associated with increased 30-day mortality in patients with severe alcoholic hepatitis. A 1986 study found that patients with severe protein calorie malnutrition had a mortality rate of 52% compared to 2% in those with mild malnutrition. The study also found that as the severity of protein calorie malnutrition increased, so did the severity of alcoholic hepatitis, along with the presence of ascites and hepatic encephalopathy.
Low daily calorie intake is associated with higher mortality, while a higher intake of ≥65 g/d of lipids and ≥77.6 g/d of protein is associated with improved 6-month survival. A multicenter study by Cabré and colleagues (2000) found that enteral nutrition in severe alcoholic hepatitis patients resulted in significantly lower one-year mortality compared to a glucocorticoid group, mainly due to fewer infectious complications.
Malnutrition in patients with AH is often due to inadequate protein and/or calorie intake, leading to sarcopenia, which is the loss of skeletal muscle mass. This can be caused by anorexia/nausea, high intake of empty calories, complications of severe liver disease, and unpalatable or incorrect diets. Alcohol itself is a major source of empty calories, providing little to no macronutrients or micronutrients. Patients with AH often have nutritionally imbalanced fat intake, with excess omega-6 and low omega-3 intake.
Understanding Hepatitis: Alcoholic vs. Toxic Hepatitis
You may want to see also
Explore related products






![]()
Zinc deficiency impacts liver function
Malnutrition is a common complication of alcoholic liver disease (ALD). Patients with severe alcohol-associated hepatitis (AH) and cirrhosis have the most severe nutritional deficiencies, indicating that advanced disease is associated with more severe malnutrition. Nutritional deficiencies in ALD patients are multifactorial and complex and include inadequate dietary intake, abnormal absorption and digestion, and abnormal interactions between ethanol and lipid metabolism.
Zinc is an essential trace element that plays a fundamental role in cellular metabolism. It is integrally involved in the normal life cycle and has many important regulatory, catalytic, and defensive functions. Zinc acts as an active centre or cofactor for more than 300 enzymes, including critical zinc transcription factors, and is essential for DNA synthesis, RNA transcription, cell growth, and protein synthesis. It is also critical to a large number of structural proteins and transcription factors.
Zinc deficiency has been observed in many types of liver disease, including ALD and viral liver disease. This deficiency can manifest in various ways, such as skin lesions, poor wound healing, altered mental status, or altered immune function. In the context of liver disease, zinc deficiency may alter hepatocyte functions and immune responses in inflammatory liver diseases. Specifically, zinc deficiency has been linked to reduced fatty acid beta-oxidation, impaired autophagy, hepatocyte apoptosis, lipid peroxidation, reduced tissue necrosis factor-alpha production, and increased circulating endotoxin.
Zinc supplementation has been shown to improve liver function in patients with ALD and hepatitis C. It can block or attenuate experimental ALD through multiple processes, including stabilising gut barrier function, decreasing endotoxemia, reducing pro-inflammatory cytokine production, decreasing oxidative stress, and attenuating apoptotic hepatocyte death. Additionally, zinc supplementation has been found to improve steatosis, hepatocyte necrosis, and markers of fibrosis.
LGBTQ+ Alcohol Abuse: A Community at Risk?
You may want to see also
Explore related products






![]()
Thiamine deficiency affects 80% of patients with alcohol use disorder
Thiamine (vitamin B1) deficiency is a common issue for people who drink excessive amounts of alcohol. Indeed, up to 80% of people with an addiction to alcohol develop a thiamine deficiency. Thiamine is an essential vitamin that the body uses to convert food into energy, particularly in the brain. Heavy alcohol use causes inflammation of the stomach lining and digestive tract, reducing the body's ability to absorb vitamins. This inflammation interferes with the absorption and retention of thiamine in the small intestine and liver.
The early stages of thiamine deficiency often go undiagnosed, as the initial signs—decreased appetite, constipation, and fatigue—are non-specific. If left untreated, a thiamine deficiency can lead to serious health conditions, including beriberi and Wernicke-Korsakoff syndrome (WKS). WKS is a brain and memory disorder that requires immediate treatment. It happens due to a severe lack of thiamine, which causes damage to the brain.
Wernicke's encephalopathy, a component of WKS, is an acute disorder characterised by confusion, incoordinated gait, and abnormal eye movements. The brains of patients with this disorder show lesions in the diencephalon, cerebellum, and brain stem. Other structures, such as the hippocampus and basal forebrain, may also be damaged. It is thought that alcohol-induced thiamine deficiency is responsible for the anterograde amnesia and damage to the diencephalon.
To treat thiamine deficiency, it is essential to stop alcohol consumption, eat a nutritious diet, and take vitamin B1 supplements. However, diet and supplements alone are not effective if heavy alcohol use continues, as alcohol will block the absorption of thiamine.
Alcohol Addiction in the US: A Concerning Number
You may want to see also
Frequently asked questions
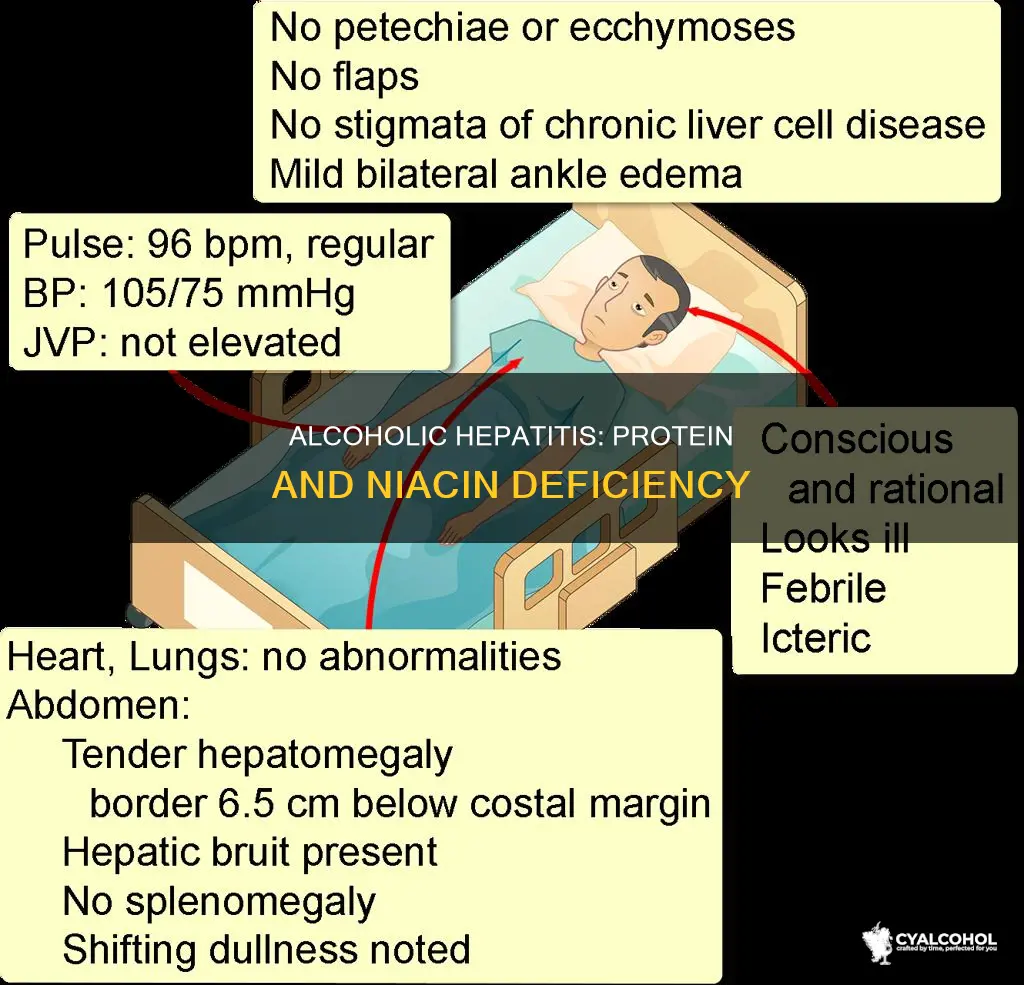
Alcoholic hepatitis is a severe syndrome of alcoholic liver disease (ALD) and is characterised by the rapid onset of jaundice, malaise, tender hepatomegaly, and subtle features of systemic inflammatory response.
Excessive alcohol consumption can result in alcoholic hepatitis. Alcohol abuse leads to fat accumulation in the liver, suppressing gluconeogenesis, inhibiting fatty acid beta-oxidation, and promoting fatty acid and triglyceride synthesis.
Alcoholic hepatitis is often accompanied by malnutrition, which can lead to deficiencies in vitamins and minerals. This includes vitamin A, B, D, K, and zinc deficiencies. Symptoms of vitamin B3 (niacin) deficiency include pellagra with dermatitis, dementia, diarrhoea, and alcoholic pellagra encephalopathy with hallucinations, insomnia, tremors, impaired coordination, incontinence, and seizures. Protein deficiency is also common in patients with alcoholic hepatitis.
Nutritional support is critical in treating alcoholic hepatitis to improve liver function and decrease the risk of liver-related complications and mortality. A recommended diet for alcoholic hepatitis includes 20-30 kcal/kg/day and 1.0-1.5 g/kg/day of protein, with 20-25% protein, 50-60% carbohydrate, and 15-20% total energy from lipids with low saturated fatty acid intake.
Alcoholic hepatitis can lead to severe liver damage (cirrhosis) and malnutrition, including protein-energy malnutrition and sarcopenia. Patients with severe alcoholic hepatitis have a 30% to 50% 30-day mortality rate, and 40% die within six months of onset.