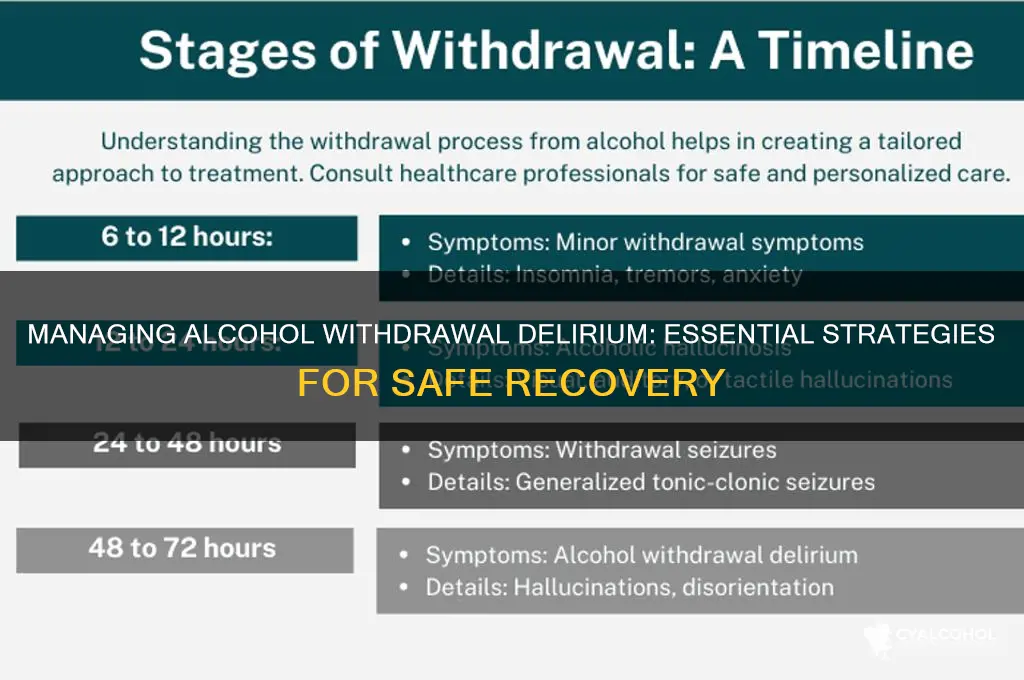
Alcohol withdrawal delirium, also known as delirium tremens (DTs), is a severe and potentially life-threatening complication of alcohol cessation, typically occurring within 48 to 96 hours after the last drink. Characterized by confusion, hallucinations, agitation, and autonomic instability, it requires immediate medical attention and careful management. Effective treatment involves a combination of pharmacotherapy, such as benzodiazepines to control agitation and prevent seizures, and supportive care to address electrolyte imbalances, dehydration, and nutritional deficiencies. Close monitoring in a controlled environment, often an intensive care unit, is essential to mitigate risks and ensure patient safety. Early recognition and intervention are critical to reducing mortality and improving outcomes for individuals experiencing this critical phase of alcohol withdrawal.
| Characteristics | Values |
|---|---|
| Definition | Severe form of alcohol withdrawal characterized by confusion, agitation, and hallucinations. |
| Risk Factors | Chronic heavy alcohol use, previous withdrawal seizures, malnutrition, liver disease. |
| Onset | Typically 48–96 hours after last alcohol consumption, but can occur earlier. |
| Symptoms | Confusion, agitation, hallucinations, fever, tachycardia, hypertension, tremors. |
| Diagnosis | Clinical assessment using tools like CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol, Revised). |
| Immediate Management | Ensure airway, breathing, and circulation (ABCs); monitor vital signs; administer benzodiazepines (e.g., lorazepam or diazepam). |
| Benzodiazepine Protocol | Start with high doses and titrate based on symptoms; consider long-acting agents for prolonged sedation. |
| Supportive Care | IV fluids for hydration, thiamine supplementation, electrolyte correction, and nutritional support. |
| Antipsychotics | Use cautiously (e.g., haloperidol) for severe agitation or hallucinations if benzodiazepines are insufficient. |
| Monitoring | Continuous observation for seizures, arrhythmias, and worsening symptoms; ICU admission if severe. |
| Prevention | Gradual alcohol tapering, early identification of withdrawal symptoms, and pharmacotherapy. |
| Prognosis | Improved with prompt treatment; mortality rate <5% with proper management. |
| Follow-Up | Referral to addiction specialists, counseling, and long-term treatment programs for relapse prevention. |
| Complications | Seizures, aspiration pneumonia, cardiovascular collapse, Wernicke-Korsakoff syndrome. |
| Pharmacological Alternatives | Phenobarbital or propofol in refractory cases, though benzodiazepines remain first-line. |
| Patient Education | Warn about risks of sudden alcohol cessation and importance of medical supervision. |
Explore related products






What You'll Learn
- Medications for Delirium: Use benzodiazepines, antipsychotics, and anticonvulsants to manage symptoms and prevent complications
- Monitoring Vital Signs: Track heart rate, blood pressure, and temperature to detect and address instability
- Hydration and Nutrition: Ensure adequate fluid and nutrient intake to support recovery and prevent dehydration
- Safe Environment: Create a calm, quiet space to minimize stimuli and reduce agitation or confusion
- Psychological Support: Provide reassurance, orientation, and counseling to ease anxiety and confusion during withdrawal
![]()
Medications for Delirium: Use benzodiazepines, antipsychotics, and anticonvulsants to manage symptoms and prevent complications
Alcohol withdrawal delirium, also known as delirium tremens (DTs), is a severe and potentially life-threatening condition characterized by confusion, hallucinations, and seizures. Managing this condition requires a targeted pharmacological approach to alleviate symptoms and prevent complications. Among the most effective medications are benzodiazepines, antipsychotics, and anticonvulsants, each playing a distinct role in stabilizing the patient’s condition.
Benzodiazepines are the cornerstone of treatment for alcohol withdrawal delirium due to their ability to modulate GABA receptors, reducing neuronal excitability. Drugs like diazepam (10–20 mg every 1–2 hours) or lorazepam (2–4 mg every 1–2 hours) are commonly used, with dosages titrated to control symptoms without causing oversedation. The goal is to achieve a state of calm wakefulness, ensuring the patient remains responsive but free from agitation or seizures. It’s critical to monitor vital signs and mental status closely, as benzodiazepines can depress respiratory function, particularly in elderly patients or those with comorbidities.
Antipsychotics, such as haloperidol, are often introduced when benzodiazepines alone fail to control severe agitation or hallucinations. However, their use must be cautious, as they can lower the seizure threshold, potentially exacerbating complications. A typical starting dose of haloperidol is 2.5–5 mg every 4–6 hours, adjusted based on response. Antipsychotics should never be the first-line treatment for alcohol withdrawal delirium but reserved for cases where benzodiazepines are insufficient or contraindicated.
Anticonvulsants like carbamazepine or valproate offer an alternative for patients who cannot tolerate benzodiazepines or as adjunctive therapy. Carbamazepine, for instance, can be initiated at 200 mg every 12 hours and titrated up to 400 mg twice daily, depending on symptom severity. These medications help stabilize neuronal membranes, reducing the risk of seizures. However, they are generally less effective than benzodiazepines for acute symptom control and require careful monitoring for side effects such as dizziness or liver toxicity.
In practice, the choice of medication depends on the patient’s presentation, medical history, and response to initial treatment. A stepwise approach is recommended: start with benzodiazepines, add antipsychotics for refractory symptoms, and consider anticonvulsants in specific cases. Continuous monitoring in an intensive care setting is often necessary, as alcohol withdrawal delirium can rapidly deteriorate. By combining these medications judiciously, clinicians can effectively manage symptoms, prevent complications, and improve patient outcomes.
Alcohol and Acne: Does Drinking Prevent Pimples or Worsen Skin?
You may want to see also
Explore related products



$88.06 $180


![]()
Monitoring Vital Signs: Track heart rate, blood pressure, and temperature to detect and address instability
Alcohol withdrawal delirium, also known as delirium tremens (DTs), is a severe and potentially life-threatening condition characterized by sudden and profound confusion, agitation, and autonomic instability. During this critical phase, the body’s vital signs can fluctuate dramatically, signaling distress and the need for immediate intervention. Monitoring heart rate, blood pressure, and temperature isn’t just a precautionary measure—it’s a lifeline. These parameters provide real-time insights into the patient’s physiological state, allowing healthcare providers to detect early signs of complications such as cardiovascular collapse, hyperthermia, or hypertensive crisis. Without vigilant tracking, these instabilities can escalate rapidly, increasing the risk of organ failure or death.
To effectively monitor vital signs, establish a structured assessment protocol. Measure heart rate every 1–2 hours, as tachycardia (heart rate >100 bpm) is a common early indicator of withdrawal severity. Blood pressure should be checked concurrently, with particular attention to systolic readings above 180 mmHg or diastolic readings above 110 mmHg, which may necessitate antihypertensive therapy. Temperature monitoring is equally critical, as fever (temperature >38°C or 100.4°F) can signify infection or central nervous system irritation, both of which are complications of alcohol withdrawal. Use digital thermometers and automated blood pressure cuffs for accuracy, and document all readings in a dedicated chart to track trends over time.
While monitoring, remain alert for patterns that suggest decompensation. For instance, a rising heart rate coupled with increasing blood pressure may indicate progressing sympathetic overactivity, a hallmark of DTs. Conversely, hypotension (systolic blood pressure <90 mmHg) and bradycardia (heart rate <60 bpm) could signal hypovolemia or impending shock. Temperature spikes, especially when accompanied by diaphoresis or altered mental status, warrant immediate investigation for infection or neurologic compromise. In such cases, administer benzodiazepines (e.g., lorazepam 2–4 mg IV) to mitigate agitation and prevent seizures, while simultaneously addressing the underlying instability.
Practical tips can enhance the efficacy of vital sign monitoring. For agitated patients, consider continuous cardiac monitoring using telemetry to avoid the stress of repeated manual checks. Keep the environment cool and well-ventilated to prevent hyperthermia, and ensure hydration to counteract fluid losses from sweating or fever. For older adults or those with comorbidities, lower thresholds for intervention may be necessary, as they are at higher risk of complications. For example, initiate treatment for hypertension at milder elevations (systolic >160 mmHg) in patients with cardiovascular disease.
In conclusion, monitoring vital signs during alcohol withdrawal delirium is a dynamic and critical process that demands precision, vigilance, and swift action. By systematically tracking heart rate, blood pressure, and temperature, healthcare providers can anticipate and mitigate the life-threatening instabilities associated with DTs. This proactive approach not only stabilizes the patient but also creates a foundation for comprehensive management, including pharmacotherapy, hydration, and psychological support. In the high-stakes arena of alcohol withdrawal, vital sign monitoring isn’t just a task—it’s a cornerstone of survival.
Esters vs. Alcohols: Unraveling Basicity Differences in Organic Chemistry
You may want to see also
Explore related products






![]()
Hydration and Nutrition: Ensure adequate fluid and nutrient intake to support recovery and prevent dehydration
Alcohol withdrawal delirium, or delirium tremens (DTs), is a severe and potentially life-threatening condition that demands meticulous attention to hydration and nutrition. Dehydration and malnutrition are common in individuals undergoing alcohol withdrawal due to poor dietary habits, vomiting, and decreased oral intake. These factors exacerbate the physical and cognitive symptoms of DTs, making hydration and nutrition critical components of management. For instance, even mild dehydration can worsen confusion and disorientation, hallmark symptoms of delirium tremens. Thus, ensuring adequate fluid and nutrient intake is not merely supportive care—it is a cornerstone of stabilizing the patient and preventing complications.
To address dehydration, oral rehydration solutions (ORS) are often the first line of intervention, provided the patient is able to tolerate fluids by mouth. These solutions, containing a balanced mix of electrolytes (sodium, potassium, chloride) and glucose, facilitate rapid rehydration and restore electrolyte imbalances caused by prolonged alcohol use. For adults, aim for 2–3 liters of ORS per day, divided into small, frequent sips to avoid overwhelming the stomach. In cases of severe dehydration or inability to drink, intravenous fluids such as normal saline or lactated Ringer’s solution may be necessary, administered under medical supervision. Monitoring urine output (aiming for pale yellow urine) and vital signs can help gauge hydration status and guide fluid management.
Nutrition plays an equally vital role in supporting recovery during alcohol withdrawal delirium. Chronic alcohol use often leads to deficiencies in essential nutrients, including thiamine (vitamin B1), folate, magnesium, and zinc. Thiamine deficiency, in particular, is a significant concern, as it can lead to Wernicke-Korsakoff syndrome, a neurological disorder characterized by confusion, coordination problems, and memory loss. To prevent this, administer 100–300 mg of thiamine daily, either orally or intravenously, as part of the initial treatment protocol. A balanced diet rich in whole grains, lean proteins, fruits, and vegetables should be introduced as soon as the patient is stable, with supplements used to address specific deficiencies. For example, a multivitamin, 1,000 mg of vitamin C, and 400–800 mcg of folate daily can help replenish depleted stores.
Practical tips for caregivers include offering small, nutrient-dense meals throughout the day to accommodate reduced appetite and gastrointestinal discomfort. Smoothies or shakes fortified with protein powder, nut butter, and fruits can be an easy-to-consume option for those struggling to eat solid foods. Encouraging fluid intake can be challenging, so incorporating hydrating foods like watermelon, cucumbers, and broths can supplement oral fluids. Caregivers should also monitor for signs of refeeding syndrome, a potentially fatal condition that can occur when nutrition is reintroduced too rapidly in malnourished individuals. Gradual refeeding, starting with 5–10 kcal/kg/day and increasing slowly, can mitigate this risk.
In conclusion, hydration and nutrition are not ancillary aspects of managing alcohol withdrawal delirium—they are fundamental to stabilizing the patient and preventing complications. By addressing dehydration with oral or intravenous fluids and correcting nutritional deficiencies with targeted supplementation and balanced meals, caregivers can significantly improve outcomes. This approach requires vigilance, patience, and a tailored strategy, but its impact on recovery cannot be overstated. As with all aspects of DTs management, early intervention and consistent monitoring are key to success.
Supporting a Loved One Through Alcohol Addiction: A Compassionate Guide
You may want to see also
Explore related products






![]()
Safe Environment: Create a calm, quiet space to minimize stimuli and reduce agitation or confusion
A person experiencing alcohol withdrawal delirium, also known as delirium tremens (DTs), can become highly sensitive to their surroundings, with even minor stimuli potentially triggering agitation, confusion, or hallucinations. This heightened sensitivity underscores the critical importance of creating a safe, calm environment to manage their symptoms effectively. The goal is to minimize sensory overload, which can exacerbate the already fragile mental state of the individual.
Designing the Space: Practical Steps
Begin by selecting a quiet, private room away from high-traffic areas or loud noises. Use soft, neutral colors for walls and furnishings to avoid visual overstimulation. Keep lighting low and adjustable, using warm, dimmable lamps instead of harsh overhead lights. Remove unnecessary objects or clutter to create a clean, orderly space that reduces cognitive strain. For example, a simple setup with a comfortable bed, a chair, and a small table is ideal. Avoid electronic devices like TVs or radios, as their sounds and lights can be overwhelming. If the person is restless, ensure the room is free of hazards such as sharp objects or tripping risks, and consider using soft flooring or mats to prevent injury.
Managing Sensory Input: Specific Strategies
Sound is a common trigger for agitation in DTs. Use white noise machines or soft, consistent background sounds like gentle rain or waves to mask unpredictable noises. Earplugs or noise-canceling headphones can also be offered if tolerated. For visual stimuli, draw curtains to block bright sunlight or outside activity, and avoid patterns or decorations that might cause confusion. Even tactile sensations matter: provide loose-fitting, comfortable clothing made of soft fabrics, and ensure the room temperature is mildly cool, as fever is a common symptom of DTs. A calm, consistent environment helps anchor the individual, reducing the likelihood of disorientation or panic.
Human Interaction: Balancing Presence and Distance
While the environment itself is crucial, the behavior of caregivers also plays a significant role. Speak in a low, calm tone and avoid sudden movements or loud gestures. Limit the number of people entering the room to prevent overstimulation. For example, assign one primary caregiver to provide consistent interaction, reducing the confusion that can arise from multiple unfamiliar faces. Reassure the individual gently but avoid excessive conversation, as prolonged engagement can increase agitation. If the person becomes confused or agitated, redirect their attention to a simple, grounding object like a soft blanket or a quiet, repetitive activity such as gently squeezing a stress ball.
Monitoring and Adjusting: A Dynamic Approach
Creating a safe environment is not a one-time task but an ongoing process. Regularly assess the individual’s response to the space and make adjustments as needed. For instance, if they seem particularly sensitive to light, further dim the lamps or use blackout curtains. If restlessness persists, consider adding a weighted blanket to provide a calming sensory input. Keep a log of what works and what doesn’t, as this can guide future modifications. Remember, the goal is to create a space that feels secure and predictable, helping to stabilize the individual’s mental state during the challenging withdrawal process.
By thoughtfully designing and maintaining a calm, quiet environment, caregivers can significantly reduce the risk of complications from alcohol withdrawal delirium. This approach not only minimizes agitation and confusion but also supports the overall healing process, providing a foundation for safer, more effective management of DTs.
Alcohol Metabolism: Does Sleep Speed Up the Process?
You may want to see also
Explore related products






![]()
Psychological Support: Provide reassurance, orientation, and counseling to ease anxiety and confusion during withdrawal
Alcohol withdrawal delirium, often referred to as delirium tremens (DTs), is a severe and potentially life-threatening condition characterized by confusion, hallucinations, and agitation. Amidst the chaos of these symptoms, psychological support emerges as a critical yet often overlooked pillar of care. Reassurance, orientation, and counseling are not mere comforts—they are essential tools to stabilize the patient’s mental state, reduce anxiety, and prevent escalation of distress. Without this grounding, even medical interventions may fall short in managing the psychological turmoil that accompanies withdrawal.
Consider the disorientation a patient experiences during DTs: time, place, and person blur into an incomprehensible haze. Simple, repeated orientation techniques—such as stating the date, location, and the patient’s name—can anchor them to reality. For instance, a nurse might say, “It’s Tuesday, you’re in St. Mary’s Hospital, and I’m here to help you, John.” Pairing this with a calm, steady tone and minimal environmental stimuli (dimmed lights, reduced noise) creates a structured environment that mitigates confusion. Research shows that consistent orientation reduces the duration of delirium episodes by up to 20%, highlighting its practical efficacy.
Reassurance is equally vital, as patients often misinterpret hallucinations or paranoia as real threats. Phrases like “You’re safe here,” or “What you’re feeling is part of the withdrawal process,” delivered with empathy, can defuse panic. However, empty platitudes (“Everything will be fine”) may backfire, as they can erode trust if the patient remains distressed. Instead, specificity works better: “Your heart rate is elevated because of withdrawal, not a heart attack. We’re monitoring it closely.” This approach bridges the gap between emotional support and factual grounding, fostering a sense of security.
Counseling during withdrawal serves a dual purpose: immediate symptom management and long-term recovery preparation. Short-term strategies include cognitive reframing—helping patients view their symptoms as temporary and treatable rather than insurmountable. For example, a counselor might ask, “What’s one thing you’ve overcome before that felt impossible?” This shifts focus from current distress to past resilience. Long-term, counseling lays the groundwork for addressing the root causes of addiction, though this should be introduced cautiously to avoid overwhelming the patient during the acute phase.
A cautionary note: psychological support must be tailored to the individual. For instance, older adults or those with cognitive impairments may require simpler language and more frequent orientation cues. Conversely, younger patients might benefit from active engagement, such as guided breathing exercises or brief mindfulness prompts. Overdoing counseling or reassurance can also be counterproductive, as it may overwhelm an already taxed nervous system. The key is balance—enough support to stabilize, but not so much that it becomes intrusive.
In practice, integrating these strategies requires a multidisciplinary approach. Nurses, physicians, and mental health professionals must collaborate to ensure consistent messaging and techniques. For example, a nurse might handle orientation and reassurance, while a counselor focuses on reframing techniques during calmer moments. Families, too, can be coached to provide simple, non-judgmental support, such as reminding the patient of their progress: “You’ve made it through the worst part—look how strong you are.” When executed thoughtfully, psychological support transforms from a supplementary measure to a cornerstone of delirium management, easing not just anxiety and confusion, but paving the way for sustained recovery.
Coconut Rita: What's the Alcohol Content?
You may want to see also
Frequently asked questions
Alcohol withdrawal delirium, also known as delirium tremens (DTs), is a severe and potentially life-threatening condition that occurs in individuals with a history of heavy, prolonged alcohol use who abruptly stop or significantly reduce their intake. It typically manifests 48–96 hours after the last drink and includes symptoms like confusion, hallucinations, severe agitation, fever, and seizures. Those at highest risk include individuals with a history of multiple detoxifications, concurrent medical conditions, or those who have previously experienced withdrawal seizures or DTs.
Key symptoms include sudden confusion or disorientation, visual or auditory hallucinations, severe agitation or restlessness, fever, rapid heartbeat, high blood pressure, and seizures. These symptoms indicate a medical emergency and require immediate attention.
Treatment involves medical supervision in a hospital or detox facility to ensure safety. Benzodiazepines (e.g., diazepam or lorazepam) are the first-line medications to manage symptoms and prevent seizures. Additional treatments may include antipsychotics for severe agitation or hallucinations, hydration, electrolyte correction, and monitoring of vital signs. Supportive care and gradual tapering of alcohol (if not already stopped) may also be used.
Prevention focuses on avoiding abrupt cessation of alcohol in heavy drinkers. Gradual tapering under medical supervision, early recognition of withdrawal symptoms, and prompt treatment with medications like benzodiazepines can reduce the risk of progressing to delirium tremens. Addressing underlying alcohol use disorder through therapy, support groups, and medication-assisted treatment is also crucial for long-term prevention.




![NatureWise Total Colon Care Fiber Cleanse - Natural Laxative Blend - Herbal Laxatives, Prebiotics, & Enzymes for Regularity, Digestion, Weight & Gut Health - Non-GMO - 60 Capsules[30-Day Supply]](https://m.media-amazon.com/images/I/71pXHzrDlaL._AC_UL320_.jpg)


























