Acute alcohol withdrawal is a serious and potentially life-threatening condition that occurs when individuals with alcohol dependence abruptly stop or significantly reduce their alcohol intake. Symptoms can range from mild, such as anxiety and tremors, to severe, including seizures, hallucinations, and delirium tremens (DTs). Effective management of acute alcohol withdrawal requires a structured approach, typically involving medical supervision, pharmacotherapy, and supportive care. Benzodiazepines are the cornerstone of treatment, used to alleviate withdrawal symptoms and prevent complications, while adjunctive medications may be employed to address specific symptoms. Additionally, monitoring vital signs, hydration, and nutritional status is crucial, as is providing psychological support and planning for long-term recovery to reduce the risk of relapse. Early intervention and a tailored treatment plan are essential to ensure safety and improve outcomes for individuals navigating this challenging process.
Explore related products






What You'll Learn
- Assessment & Triage: Identify severity, risk factors, and medical stability for tailored withdrawal management
- Pharmacotherapy Options: Benzodiazepines, anticonvulsants, and adjuncts to alleviate symptoms and prevent complications
- Symptom Monitoring: Track CIWA-Ar scores, vital signs, and neurological status for timely intervention
- Supportive Care: Hydration, nutrition, and electrolyte balance to address dehydration and malnutrition
- Psychosocial Support: Counseling, therapy, and referral to addiction treatment for long-term recovery
![]()
Assessment & Triage: Identify severity, risk factors, and medical stability for tailored withdrawal management
Acute alcohol withdrawal is a spectrum disorder, ranging from mild anxiety and tremors to life-threatening seizures and delirium tremens (DTs). The first step in managing this condition is a thorough assessment and triage to determine the severity of withdrawal, identify risk factors, and ensure medical stability. This process is critical for tailoring the appropriate level of care and intervention, whether it’s outpatient management, inpatient monitoring, or intensive care. Without accurate assessment, patients risk undertreatment, overtreatment, or complications that could have been prevented.
Severity assessment begins with validated tools like the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar), which scores symptoms such as nausea, tremors, and agitation on a scale of 0 to 7. A total score of 8–15 indicates mild withdrawal, 16–20 suggests moderate withdrawal, and scores above 20 signal severe withdrawal requiring immediate medical attention. For example, a patient with a CIWA-Ar score of 22, exhibiting severe agitation and visual hallucinations, would likely need benzodiazepines administered in a monitored setting. It’s crucial to reassess symptoms every 2–4 hours during the peak withdrawal period (24–72 hours) to adjust treatment dynamically.
Risk factors play a pivotal role in triage decisions. Patients with a history of seizures, DTs, or multiple withdrawal episodes are at higher risk for complications. Age (especially over 60), comorbid medical conditions (e.g., liver disease, cardiovascular issues), and concurrent substance use (e.g., benzodiazepines, opioids) further elevate risk. For instance, a 55-year-old with cirrhosis and a history of DTs should be admitted to a hospital, even if initial symptoms appear mild. Conversely, a 30-year-old with no prior complications and a CIWA-Ar score of 10 might be managed safely as an outpatient with oral diazepam (e.g., 10 mg every 6 hours as needed) and close follow-up.
Medical stability is non-negotiable before initiating withdrawal management. Vital signs (heart rate, blood pressure, temperature) must be within safe limits, and laboratory tests (e.g., electrolytes, liver function, blood glucose) should rule out critical abnormalities. Hypokalemia, for example, can exacerbate cardiac arrhythmias in the context of withdrawal, while hypoglycemia may mimic or worsen symptoms. If a patient presents with a heart rate of 120 bpm, systolic blood pressure of 160 mmHg, and a temperature of 101°F, treatment should focus on stabilizing these parameters before addressing withdrawal symptoms.
The ultimate goal of assessment and triage is to match the patient’s needs with the appropriate level of care. Mild withdrawal may be managed with supportive care and oral benzodiazepines, while severe cases often require intravenous medications and continuous monitoring. For example, a patient at high risk for DTs might receive a loading dose of lorazepam (e.g., 2 mg IV) followed by a tapered regimen based on CIWA-Ar scores. By systematically evaluating severity, risk factors, and medical stability, clinicians can prevent complications, optimize resource utilization, and improve patient outcomes in acute alcohol withdrawal.
Round1 Alcohol Policy: What You Need to Know Before Visiting
You may want to see also
Explore related products






![]()
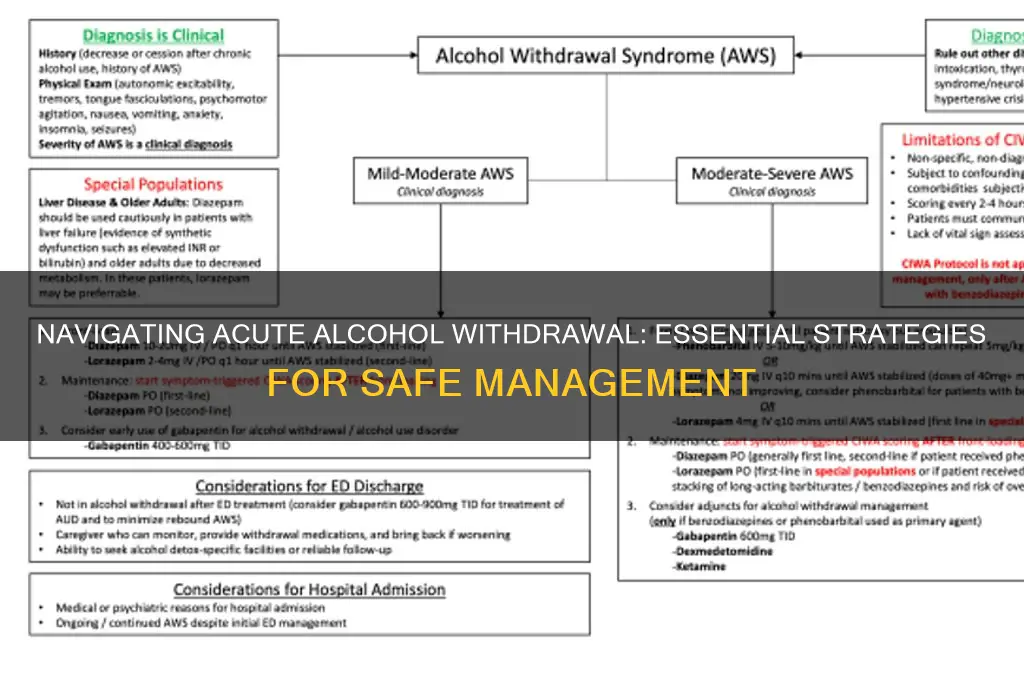
Pharmacotherapy Options: Benzodiazepines, anticonvulsants, and adjuncts to alleviate symptoms and prevent complications
Acute alcohol withdrawal demands prompt pharmacotherapy to mitigate symptoms and avert life-threatening complications like seizures or delirium tremens. Benzodiazepines, the cornerstone of treatment, act on GABA receptors to dampen neuronal excitability. Short-acting agents like lorazepam (1-2 mg orally every 4-6 hours) or diazepam (5-10 mg orally every 6 hours) are preferred for their predictable metabolism and reduced accumulation in hepatic impairment, a common comorbidity in this population. Dosing should be individualized using symptom-triggered scales (e.g., CIWA-Ar), titrating upward until mild sedation is achieved, then tapering over 7-14 days to prevent protracted withdrawal or benzodiazepine dependence.
Anticonvulsants offer a viable alternative for patients with mild-to-moderate withdrawal or benzodiazepine contraindications. Carbamazepine (200 mg orally twice daily) and valproate (500 mg orally twice daily) have demonstrated efficacy in randomized trials, though their slower onset of action necessitates adjunctive benzodiazepines for immediate symptom control. Gabapentin (300-600 mg orally three times daily), while off-label, shows promise in reducing anxiety and insomnia, though its role as monotherapy remains unestablished. These agents lack cross-tolerance with benzodiazepines, making them useful in patients with prior benzodiazepine misuse.
Adjuncts play a critical role in addressing specific symptoms and complications of withdrawal. Beta-blockers (e.g., propranolol 20-40 mg orally twice daily) or alpha-adrenergic agonists (e.g., clonidine 0.1-0.3 mg orally three times daily) can mitigate autonomic hyperactivity, though caution is warranted in patients with bradycardia or hypotension. Thiamine (500 mg intravenously or intramuscularly daily for 3-5 days) is mandatory to prevent Wernicke’s encephalopathy, particularly in malnourished individuals. Haloperidol (2.5-5 mg orally or intravenously every 4-6 hours) may be considered for agitation refractory to benzodiazepines, though its use risks lowering the seizure threshold.
Practical considerations underscore the importance of monitoring and flexibility in pharmacotherapy. Continuous cardiac monitoring is essential during severe withdrawal due to the risk of arrhythmias. Inpatient treatment is recommended for patients with prior withdrawal seizures, delirium tremens, or significant medical comorbidities. Outpatient management with long-acting benzodiazepines (e.g., chlordiazepoxide 50-100 mg orally three times daily) may be feasible for mild cases, provided close follow-up is ensured. Education on the risks of abrupt alcohol cessation and the importance of adherence to tapering schedules is critical to prevent rebound withdrawal.
The choice of pharmacotherapy must balance efficacy, safety, and patient-specific factors. While benzodiazepines remain first-line, anticonvulsants and adjuncts provide valuable alternatives in select populations. A structured, individualized approach, guided by clinical assessment and symptom severity, optimizes outcomes and minimizes complications in acute alcohol withdrawal.
Does Barrel-Aged Mocha Contain Alcohol? Exploring the Brewing Process
You may want to see also
Explore related products






![]()
Symptom Monitoring: Track CIWA-Ar scores, vital signs, and neurological status for timely intervention
Acute alcohol withdrawal is a potentially life-threatening condition that demands vigilant monitoring to prevent complications. At the heart of this monitoring is the systematic tracking of CIWA-Ar scores, vital signs, and neurological status, which together provide a comprehensive view of the patient’s condition. The CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol, Revised) is a 10-item scale that quantifies withdrawal severity, with scores ranging from 0 to 67. A score above 8 typically indicates the need for pharmacological intervention, while scores above 20 signal severe withdrawal requiring immediate attention. This tool is not just a checklist but a dynamic instrument that guides treatment intensity and frequency.
Vital signs—blood pressure, heart rate, temperature, and respiratory rate—are equally critical to monitor, as alcohol withdrawal can induce autonomic hyperactivity, leading to hypertension, tachycardia, and hyperthermia. For instance, a sustained heart rate above 100 bpm or systolic blood pressure over 150 mmHg may necessitate benzodiazepine administration to prevent progression to seizures or delirium tremens. Monitoring should occur at least every 4 hours during the first 24–48 hours, with adjustments based on symptom severity. Portable monitors or automated systems can streamline this process, but manual checks remain essential for accuracy, especially in patients with fluctuating symptoms.
Neurological status assessment is another cornerstone of symptom monitoring, focusing on mental status, tremors, and seizure activity. Confusion, agitation, or disorientation are red flags for impending delirium tremens, a medical emergency with a mortality rate of up to 5% if untreated. The use of the Glasgow Coma Scale (GCS) can help standardize this assessment, though simpler observations—such as the ability to follow commands or the presence of nystagmus—are equally valuable. For patients at high risk, continuous EEG monitoring may be warranted, though this is typically reserved for specialized settings.
Integrating these monitoring elements requires a structured approach. For example, a nursing protocol might dictate CIWA-Ar assessments every 2–4 hours, with vital signs checked concurrently. If the CIWA-Ar score rises by 4 points or exceeds 15, or if vital signs deviate from baseline (e.g., temperature >100.4°F), benzodiazepines such as diazepam (10–20 mg orally) or lorazepam (2–4 mg intravenously) should be administered. Neurological changes, however minor, should prompt immediate reevaluation and potential escalation of care. This tiered response system ensures that interventions are proportional to the patient’s needs, minimizing overmedication while preventing under-treatment.
In practice, symptom monitoring is both an art and a science. It demands clinical judgment to interpret data trends—for instance, recognizing that a CIWA-Ar score plateauing at 12 might indicate benzodiazepine tolerance rather than stable withdrawal. Documentation is equally vital; clear, time-stamped records of scores, vital signs, and interventions not only guide ongoing care but also protect against medicolegal risks. By mastering this monitoring framework, healthcare providers can transform acute alcohol withdrawal from a crisis into a manageable condition, ensuring patient safety and fostering recovery.
White Claw Hard Seltzer: Alcohol Content Explained
You may want to see also
Explore related products






![]()
Supportive Care: Hydration, nutrition, and electrolyte balance to address dehydration and malnutrition
Acute alcohol withdrawal often leads to severe dehydration, electrolyte imbalances, and malnutrition, which exacerbate symptoms and complicate recovery. Addressing these issues through supportive care is a cornerstone of effective management. Dehydration occurs due to increased urination, vomiting, and decreased fluid intake, while malnutrition results from poor dietary habits and alcohol’s interference with nutrient absorption. Electrolyte imbalances, particularly hypokalemia (low potassium) and hypomagnesemia (low magnesium), are common and can cause cardiac arrhythmias, muscle weakness, and seizures. Restoring hydration, replenishing nutrients, and correcting electrolytes are critical to stabilizing the patient and preventing complications.
Hydration is the first priority in supportive care. Oral rehydration solutions (ORS) are ideal for mild to moderate dehydration, providing a balanced mix of water, sodium, and glucose. For severe cases, intravenous fluids such as normal saline (0.9% sodium chloride) or lactated Ringer’s solution may be necessary. The goal is to replace fluid losses gradually, aiming for 1–2 liters of fluid in the first 24 hours, adjusted based on the patient’s condition. Monitoring urine output (aiming for pale yellow urine) and vital signs helps gauge hydration status. Caution must be taken to avoid overhydration, which can lead to fluid overload, particularly in patients with liver dysfunction.
Nutrition plays a pivotal role in recovery, as chronic alcohol use depletes essential vitamins and minerals, particularly thiamine (vitamin B1), folate, and magnesium. Thiamine deficiency, for instance, can lead to Wernicke-Korsakoff syndrome, a life-threatening condition. Patients should receive a balanced diet rich in complex carbohydrates, lean proteins, and healthy fats. If oral intake is poor, enteral feeding (via nasogastric tube) or parenteral nutrition may be required. Supplementation with thiamine (100–300 mg/day), folate (1 mg/day), and a multivitamin is often recommended. Small, frequent meals are easier to tolerate and can improve nutrient absorption.
Electrolyte imbalances require careful correction, as rapid shifts can trigger arrhythmias or seizures. Potassium levels should be monitored daily, with replacement guided by serum levels and clinical symptoms. Oral potassium chloride (20–40 mEq/day) is suitable for mild deficits, while intravenous potassium (10–20 mEq/hour) is reserved for severe cases. Magnesium replacement is equally important, with oral magnesium oxide (400–800 mg/day) or intravenous magnesium sulfate (2–4 grams over 5–30 minutes) used depending on severity. Phosphate and calcium levels should also be assessed, particularly in malnourished patients.
Practical tips for caregivers include encouraging patients to sip fluids throughout the day, offering bland, easily digestible foods like bananas, rice, or yogurt, and monitoring for signs of electrolyte imbalance (e.g., muscle cramps, irregular heartbeat). Collaboration with a dietitian can ensure tailored nutritional support. While supportive care alone does not treat withdrawal, it creates a foundation for safer pharmacological intervention and long-term recovery. By addressing dehydration, malnutrition, and electrolyte imbalances, clinicians can significantly improve patient outcomes and reduce the risk of complications.
Alcoholism and GABA Receptors: Understanding the Brain's Adaptation
You may want to see also
Explore related products






![]()
Psychosocial Support: Counseling, therapy, and referral to addiction treatment for long-term recovery
Acute alcohol withdrawal is a critical phase that demands more than just medical intervention; it requires a robust psychosocial support system to address the underlying behavioral and emotional triggers of addiction. Counseling and therapy play a pivotal role in this stage by helping individuals develop coping strategies, understand the root causes of their addiction, and build resilience against relapse. For instance, cognitive-behavioral therapy (CBT) has been shown to reduce relapse rates by up to 50% in the first year of recovery, making it a cornerstone of long-term treatment plans. Referral to specialized addiction treatment programs, such as inpatient rehab or outpatient therapy, ensures continuity of care beyond the acute withdrawal phase, fostering sustained recovery.
Consider the case of a 35-year-old individual experiencing severe anxiety and insomnia during withdrawal. A therapist might employ mindfulness-based stress reduction techniques to manage these symptoms, teaching the patient to focus on the present moment rather than cravings or past mistakes. Simultaneously, family therapy sessions could be initiated to repair relationships damaged by addiction, creating a supportive home environment. Practical tips include scheduling daily therapy sessions during the first week of withdrawal, when psychological distress peaks, and gradually tapering frequency as stability improves. For those with co-occurring mental health disorders, integrated treatment plans that address both addiction and conditions like depression or PTSD are essential for holistic recovery.
The persuasive argument for psychosocial support lies in its ability to transform short-term abstinence into long-term sobriety. Without addressing the psychological aspects of addiction, individuals are at high risk of returning to alcohol use as a maladaptive coping mechanism. For example, a study published in the *Journal of Addiction Medicine* found that patients who engaged in therapy during withdrawal were 60% more likely to remain abstinent after six months compared to those who relied solely on medication. This highlights the necessity of embedding counseling and therapy into the withdrawal management process, not as optional add-ons but as critical components of care.
Comparatively, while medications like benzodiazepines or anticonvulsants manage physical symptoms, they do little to address the behavioral patterns that drive addiction. Psychosocial support bridges this gap by equipping individuals with tools to navigate triggers, such as stress or social pressure, without resorting to alcohol. For instance, a therapist might work with a patient to identify high-risk situations—like attending social events where alcohol is present—and develop strategies like bringing a supportive friend or practicing refusal skills. Referral to peer support groups, such as Alcoholics Anonymous, further enhances recovery by providing a community of individuals facing similar challenges.
In conclusion, psychosocial support is not a luxury but a necessity in managing acute alcohol withdrawal and ensuring long-term recovery. By combining counseling, therapy, and referral to addiction treatment, individuals gain the emotional, cognitive, and social resources needed to break the cycle of addiction. Practical steps include starting therapy within the first 48 hours of withdrawal, integrating family or group sessions, and ensuring a seamless transition to ongoing treatment programs. With the right support, acute withdrawal becomes not just a phase to survive, but a foundation for a healthier, alcohol-free life.
Why Alcohol Labels Lack Nutrition Facts: Uncovering the Hidden Truth
You may want to see also
Frequently asked questions
The first steps include assessing the severity of withdrawal symptoms using tools like the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar), ensuring a safe and supportive environment, and administering medications such as benzodiazepines to manage symptoms like anxiety, tremors, and seizures.
Acute alcohol withdrawal symptoms usually peak within 24–72 hours after the last drink and can last 5–7 days. However, some individuals may experience prolonged withdrawal symptoms, such as insomnia or anxiety, for several weeks.
Benzodiazepines (e.g., diazepam, lorazepam) are the first-line treatment to manage withdrawal symptoms. Other medications like anticonvulsants (e.g., carbamazepine) or beta-blockers may be used in specific cases. Thiamine and fluids are also administered to prevent complications like Wernicke’s encephalopathy.
Seek emergency care if the person experiences severe symptoms such as seizures, hallucinations, rapid heartbeat, high fever, or confusion, as these may indicate delirium tremens (DTs), a life-threatening complication of alcohol withdrawal. Immediate medical intervention is critical in such cases.