Alcoholism, a chronic and often devastating condition, affects millions of individuals worldwide, transcending age, gender, and socioeconomic boundaries. According to the World Health Organization (WHO), over 3 million deaths annually are attributed to harmful alcohol use, making it a significant global health concern. In the United States alone, approximately 14.5 million adults struggle with alcohol use disorder (AUD), yet only a fraction receive treatment. The impact extends beyond the individual, straining families, workplaces, and healthcare systems. Despite its prevalence, stigma and lack of awareness often prevent people from seeking help, highlighting the urgent need for education, support, and accessible resources to address this widespread issue.
Explore related products






What You'll Learn
- Prevalence by Age Group: Alcoholism rates vary significantly across different age demographics globally
- Gender Differences: Men and women exhibit distinct patterns in alcohol dependency and treatment
- Geographic Variations: Regional factors influence alcoholism rates, from cultural norms to availability
- Treatment Seeking Behavior: Only a fraction of alcoholics actively seek professional help or rehab
- Impact of Socioeconomics: Poverty, education, and employment status correlate with higher alcoholism risks
![]()
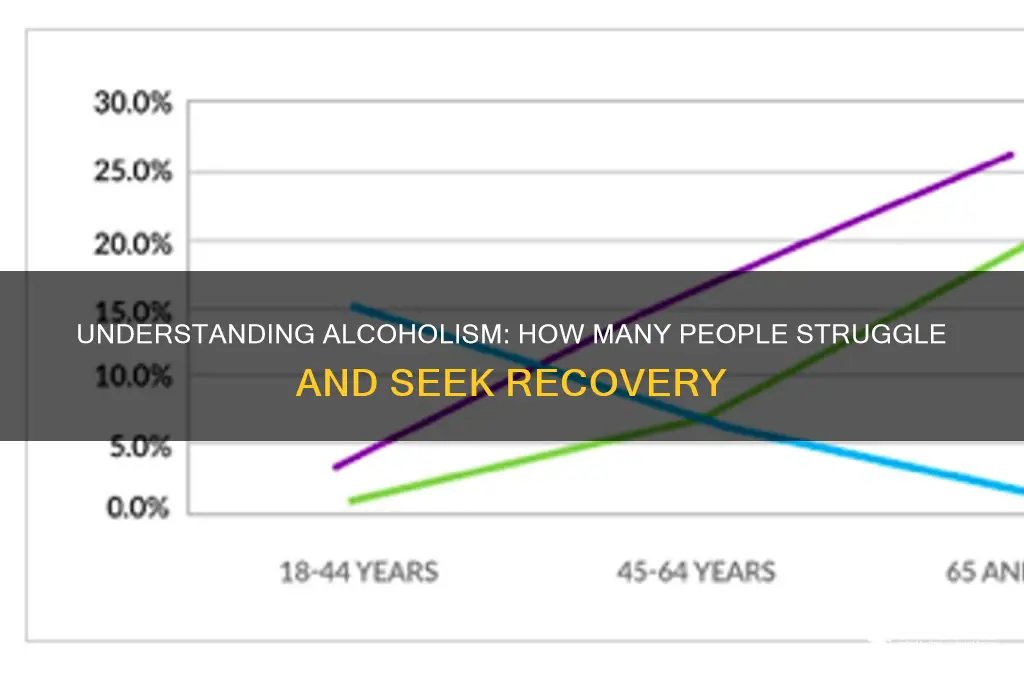
Prevalence by Age Group: Alcoholism rates vary significantly across different age demographics globally
Alcoholism doesn’t strike uniformly across the lifespan. Global data reveals a striking pattern: rates of alcohol use disorder (AUD) peak in young adulthood (ages 18–25), with studies showing prevalence rates as high as 15–20% in this demographic. This surge aligns with developmental factors like brain maturation, peer influence, and increased access to alcohol in college or early career settings. Binge drinking, defined as 5+ drinks for men or 4+ for women in a single occasion, is alarmingly common here, often serving as a gateway to dependency.
Contrast this with middle-aged adults (ages 26–49), where AUD prevalence stabilizes around 8–10%. While rates decline from the young adult peak, this group faces unique risks. Chronic stress, work-life imbalance, and unresolved mental health issues often drive problematic drinking. A 2020 WHO report noted that middle-aged men, in particular, account for 70% of alcohol-related hospitalizations in this bracket, frequently linked to sustained heavy drinking (15+ drinks/week for men, 8+ for women).
Older adults (ages 50+) defy stereotypes, with AUD prevalence dropping to 2–5%. However, this group faces underrecognized dangers. Age-related metabolic changes mean lower alcohol tolerance, while medication interactions (e.g., blood thinners or antidepressants) amplify risks. Late-onset AUD, often tied to retirement, grief, or isolation, is increasingly documented, yet remains underdiagnosed due to stigma and misattribution of symptoms to aging.
These age-specific trends demand tailored interventions. For young adults, prevention should target campus policies and digital literacy to counter pro-drinking messaging. Middle-aged populations benefit from workplace wellness programs integrating mental health screenings. Older adults require geriatric-specific AUD assessments, avoiding assumptions that alcohol misuse is a "young person’s problem." Understanding these variations isn’t just academic—it’s actionable, shaping how we screen, treat, and support those at risk.
Abstaining from Alcohol: 30-Day Challenge for a Healthier You
You may want to see also
Explore related products






![]()
Gender Differences: Men and women exhibit distinct patterns in alcohol dependency and treatment
Alcoholism doesn't discriminate, but its grip tightens differently on men and women. While men are statistically more likely to develop alcohol use disorder (AUD), women face a unique set of challenges when it comes to dependency and recovery. Understanding these gender-specific patterns is crucial for tailoring effective treatment strategies.
Men, traditionally socialized to suppress emotions and prioritize stoicism, often turn to alcohol as a coping mechanism for stress, anxiety, and societal pressures. This, coupled with higher societal acceptance of heavy drinking among men, contributes to their higher rates of AUD. Studies show that men are nearly twice as likely as women to meet the criteria for AUD, with binge drinking (defined as 5 or more drinks on an occasion for men) being particularly prevalent.
Women, on the other hand, face a double-edged sword. They metabolize alcohol differently, reaching higher blood alcohol concentrations faster and experiencing more severe health consequences at lower doses. This "telescoping" effect means women progress from initial use to dependence more rapidly than men. Additionally, women are more likely to self-medicate with alcohol to cope with trauma, depression, and anxiety, conditions that are often underdiagnosed and undertreated in this demographic.
The treatment landscape also reflects these gender disparities. Traditional rehab programs, often designed with a male-dominated perspective, may fail to address the unique needs of women. Women benefit from programs that incorporate trauma-informed care, address co-occurring mental health issues, and provide childcare support, recognizing the societal pressures that often prevent women from seeking help.
Bridging the gap in alcohol dependency treatment requires a nuanced approach. Gender-specific treatment programs, tailored to address the distinct biological, psychological, and social factors influencing AUD in men and women, offer a more promising path to recovery. By acknowledging these differences, we can move beyond a one-size-fits-all approach and provide effective, compassionate care for all individuals struggling with alcoholism.
Is 13 Drinks Too Much? Understanding Alcohol Consumption Limits
You may want to see also
Explore related products


$19.95 $19.95




![]()
Geographic Variations: Regional factors influence alcoholism rates, from cultural norms to availability
Alcoholism rates are not uniform across the globe; they fluctuate dramatically based on geographic location, influenced by a complex interplay of cultural, economic, and regulatory factors. In Eastern Europe, for instance, countries like Russia and Belarus report some of the highest per capita alcohol consumption rates worldwide, with vodka deeply ingrained in social and cultural traditions. Conversely, predominantly Muslim countries such as Saudi Arabia and Pakistan exhibit significantly lower rates due to religious prohibitions against alcohol consumption. These disparities highlight how regional norms shape drinking behaviors, often dictating whether alcohol is a celebrated staple or a taboo.
Consider the role of availability and accessibility in driving alcoholism rates. In regions with lax regulations on alcohol sales, such as the United States, where alcohol is readily available in grocery stores, gas stations, and online, consumption tends to be higher. In contrast, countries like Norway and Sweden, which enforce strict state monopolies on alcohol sales and impose high taxes, have lower rates of alcoholism. These regulatory measures act as a deterrent, limiting both the physical and financial accessibility of alcohol. For individuals seeking to reduce their intake, understanding these regional policies can provide actionable insights—for example, advocating for stricter local regulations or consciously limiting access to alcohol in one’s environment.
Cultural attitudes toward alcohol also play a pivotal role in shaping regional alcoholism rates. In Mediterranean countries like Italy and Spain, wine is often consumed in moderation as part of daily meals, fostering a culture of responsible drinking. This contrasts sharply with binge-drinking cultures prevalent in countries like the United Kingdom or Australia, where alcohol is frequently associated with socializing and celebration, often leading to excessive consumption. For those struggling with alcoholism, adopting a mindful approach to drinking—such as pairing alcohol with meals or setting strict limits—can be a practical strategy inspired by these cultural norms.
Economic factors further exacerbate geographic variations in alcoholism rates. In regions with high unemployment and poverty, such as parts of Eastern Europe and sub-Saharan Africa, alcohol is often used as a coping mechanism, leading to higher rates of dependency. Conversely, wealthier regions may experience lower rates of alcoholism but higher rates of binge drinking among younger demographics, as disposable income enables frequent consumption. Addressing these disparities requires region-specific interventions, such as economic development programs in impoverished areas or targeted public health campaigns in affluent societies.
Finally, the age and gender dynamics of alcoholism vary significantly across regions, influenced by local customs and societal expectations. In Scandinavian countries, for example, young adults are more likely to engage in heavy episodic drinking, while in India, alcohol consumption is more prevalent among older men due to cultural restrictions on women’s drinking. Understanding these demographic patterns can inform tailored prevention strategies, such as age-specific education programs or gender-sensitive treatment approaches. By recognizing the unique regional factors at play, individuals and policymakers alike can develop more effective strategies to combat alcoholism in their communities.
First Spanish AA Meeting: Which Hispanic Country?
You may want to see also
Explore related products





![]()
Treatment Seeking Behavior: Only a fraction of alcoholics actively seek professional help or rehab
Despite the widespread prevalence of alcoholism, only about 10% of individuals struggling with alcohol use disorder (AUD) actively seek professional treatment. This startling statistic raises critical questions about the barriers to treatment and the factors influencing treatment-seeking behavior. For instance, stigma remains a significant hurdle, as societal misconceptions often label alcoholism as a moral failing rather than a medical condition. This perception discourages many from admitting their struggles, let alone pursuing help. Additionally, the cost and accessibility of treatment programs, such as inpatient rehab or therapy, can deter individuals, especially those without adequate insurance coverage. Understanding these obstacles is the first step in addressing why so few alcoholics engage with professional resources.
Consider the role of denial in treatment-seeking behavior. Many individuals with AUD underestimate the severity of their condition, believing they can control their drinking without external help. This cognitive distortion is reinforced by the gradual onset of alcoholism, which often blurs the line between moderate use and dependency. For example, a person might rationalize daily drinking as a stress-relief mechanism rather than a harmful habit. Breaking through this denial requires interventions that highlight the long-term health risks, such as liver disease, cardiovascular problems, and mental health deterioration. Family members or friends can play a pivotal role by initiating conversations grounded in empathy and factual information, encouraging their loved ones to reconsider their stance on treatment.
From a practical standpoint, increasing treatment accessibility is essential to improving engagement rates. Telehealth services, for instance, have emerged as a viable option for those unable to attend in-person sessions due to geographic, financial, or time constraints. These platforms offer counseling, medication management, and support groups remotely, reducing barriers to entry. Similarly, workplace programs that integrate mental health resources can normalize seeking help and provide discreet pathways to treatment. Employers can implement policies such as flexible scheduling for therapy appointments or subsidizing treatment costs, fostering an environment where employees feel supported in addressing AUD.
A comparative analysis of successful treatment models reveals the importance of personalized approaches. For younger adults, aged 18–25, peer-led interventions and social support networks often yield higher engagement rates, as this demographic tends to respond well to community-based initiatives. In contrast, older adults may benefit more from one-on-one therapy or medically supervised detox programs tailored to their physical health needs. Medications like naltrexone, acamprosate, or disulfiram can be prescribed to reduce cravings or induce negative effects from alcohol consumption, but their effectiveness varies by individual. Combining pharmacotherapy with behavioral therapy, such as Cognitive Behavioral Therapy (CBT), has shown promising results in sustaining long-term sobriety.
Ultimately, addressing the gap in treatment-seeking behavior requires a multifaceted strategy. Public awareness campaigns can combat stigma by framing alcoholism as a treatable condition, much like diabetes or hypertension. Policymakers must prioritize funding for affordable treatment options and mandate insurance coverage for AUD services. On an individual level, recognizing the early signs of alcoholism—such as increased tolerance, withdrawal symptoms, or neglecting responsibilities—can prompt timely intervention. By dismantling barriers and fostering a culture of support, we can encourage more individuals to take the courageous step toward recovery.
Singapore Airlines Business Class: Premium Alcohol Selection Revealed
You may want to see also
Explore related products






![]()
Impact of Socioeconomics: Poverty, education, and employment status correlate with higher alcoholism risks
Socioeconomic factors cast a long shadow over the prevalence of alcoholism, with poverty, education, and employment status emerging as critical determinants. Consider this: individuals living below the poverty line are twice as likely to develop alcohol use disorder (AUD) compared to their higher-income counterparts. The stress of financial instability, limited access to healthcare, and fewer opportunities for social mobility create a fertile ground for substance abuse. For instance, a study by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) found that 15% of adults in low-income households struggle with AUD, compared to 7% in higher-income brackets. This disparity underscores how economic hardship can drive individuals toward alcohol as a coping mechanism.
Education, or the lack thereof, further exacerbates this risk. Those with lower educational attainment—defined as a high school diploma or less—face a 30% higher likelihood of developing alcoholism. Education not only provides knowledge about the dangers of alcohol but also opens doors to better employment opportunities and social networks that discourage harmful behaviors. For example, a high school dropout is more likely to work in unstable, low-wage jobs, increasing their exposure to stress and reducing their access to resources for mental health support. Conversely, individuals with a college degree are more likely to engage in moderate drinking patterns, if at all, due to greater awareness and socioeconomic stability.
Employment status plays a dual role in this equation. Unemployment, particularly long-term joblessness, is a significant risk factor for alcoholism. The loss of structure, income, and self-worth that accompanies unemployment can lead to increased alcohol consumption as a means of escape. A study published in *Addiction* journal revealed that unemployed individuals are 60% more likely to develop AUD compared to those with stable employment. Even underemployment—working in jobs below one’s skill level or part-time when full-time work is desired—can contribute to feelings of inadequacy and stress, further fueling alcohol misuse.
However, it’s not just the absence of employment that matters; the nature of work also plays a role. Low-wage, high-stress jobs with irregular hours, such as those in the service or construction industries, are associated with higher rates of alcoholism. These jobs often lack benefits like health insurance or paid leave, leaving workers with fewer resources to address mental health issues. For instance, a bartender or construction worker might face social pressure to drink as part of their job culture, blurring the line between professional and personal alcohol use.
Addressing these socioeconomic factors requires targeted interventions. For poverty, expanding access to affordable housing, food assistance, and healthcare can reduce the financial stress that drives alcohol misuse. Educational initiatives, such as vocational training programs or subsidies for higher education, can empower individuals to break the cycle of low-wage work. Employers can play a role by offering mental health resources, flexible work schedules, and fair wages to reduce workplace stress. Policymakers must also prioritize funding for addiction treatment programs in underserved communities, ensuring that those most at risk have access to support. By tackling these root causes, we can mitigate the impact of socioeconomics on alcoholism and foster healthier, more equitable communities.
Alcohol Flush Reaction: Can Red Face Disappear Over Time?
You may want to see also
Frequently asked questions
Approximately 14.5 million adults aged 18 and older in the United States alone struggle with alcohol use disorder (AUD), according to the National Institute on Alcohol Abuse and Alcoholism (NIAAA). Globally, the World Health Organization (WHO) estimates that over 283 million people (5.1% of the global population) had alcohol use disorders in 2016.
In the United States, about 5.8% of adults (approximately 14.5 million people) had alcohol use disorder (AUD) in 2019, based on data from the NIAAA. This includes both mild, moderate, and severe cases of alcoholism.
Yes, alcoholism tends to be more prevalent among younger adults. According to the NIAAA, adults aged 18–25 have the highest rates of alcohol use disorder, with about 14.5% of this age group affected. Rates decrease with age, with about 6.7% of adults aged 26–29 and 3.8% of adults aged 30 and older dealing with AUD.
Men are more likely to struggle with alcoholism than women. The NIAAA reports that 9.0% of men (approximately 9.8 million) and 5.5% of women (approximately 4.7 million) in the United States had AUD in 2019. However, women may face unique health risks and faster progression of alcohol-related issues due to differences in metabolism and body composition.