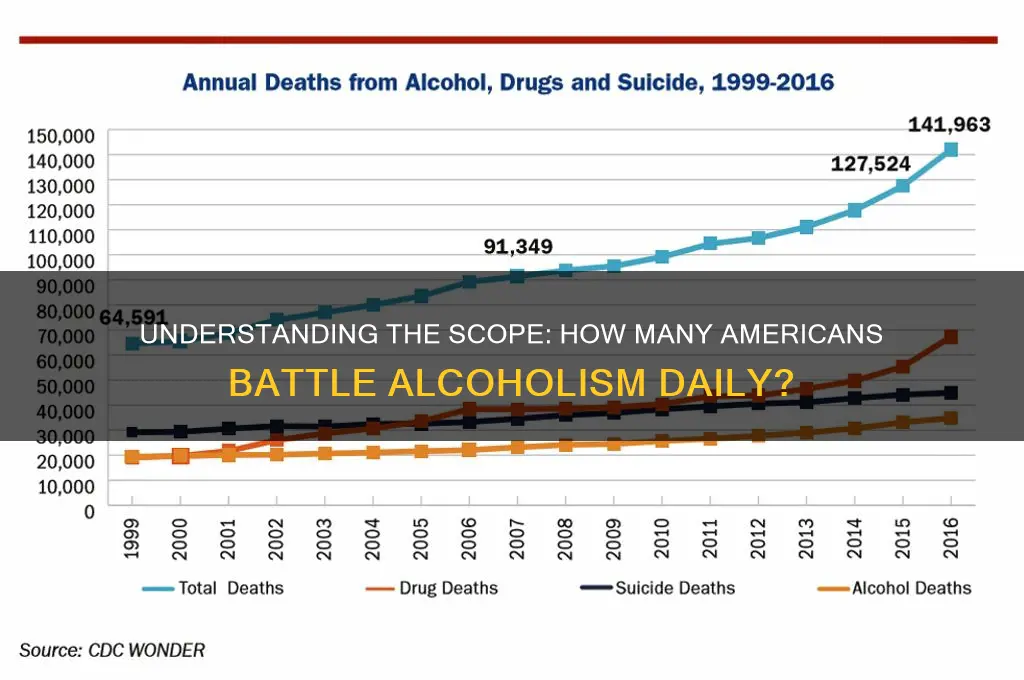
Alcoholism remains a pervasive and often overlooked issue in the United States, affecting millions of Americans across all demographics. According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA), approximately 14.5 million adults aged 18 and older struggled with alcohol use disorder (AUD) in 2019, yet only a fraction receive treatment. Additionally, excessive alcohol consumption contributes to over 95,000 deaths annually, making it a leading preventable cause of death in the country. Factors such as societal norms, stress, and lack of access to affordable care exacerbate the problem, highlighting the urgent need for increased awareness, support systems, and resources to address this widespread public health crisis.
Explore related products






What You'll Learn
- Prevalence by Age Group: Alcoholism rates vary significantly across different age demographics in the U.S
- Gender Differences: Men and women exhibit distinct patterns and risks for alcohol dependency
- Regional Variations: Certain U.S. states report higher alcoholism rates than others
- Economic Impact: Alcoholism imposes substantial financial burdens on individuals and healthcare systems
- Treatment Accessibility: Many Americans face barriers to accessing effective alcoholism treatment programs
![]()
Prevalence by Age Group: Alcoholism rates vary significantly across different age demographics in the U.S
Alcoholism doesn't strike evenly across the lifespan. While the overall prevalence of alcohol use disorder (AUD) in the U.S. hovers around 14.5 million adults, the distribution is far from uniform. Young adults, aged 18-25, bear the brunt, with a staggering 14.3% meeting the criteria for AUD. This rate is nearly double that of adults aged 26 and older, where the prevalence drops to 7.3%.
This disparity isn't merely a statistical quirk. It reflects a confluence of factors unique to early adulthood. The brain is still developing during this period, particularly the prefrontal cortex, which governs impulse control and decision-making. This biological vulnerability, coupled with the social pressures of college, newfound independence, and experimentation, creates a perfect storm for risky drinking behaviors. Binge drinking, defined as consuming 4 or more drinks for women and 5 or more for men in a single occasion, is alarmingly prevalent among this age group, further increasing the risk of developing AUD.
A stark contrast emerges when examining older age groups. While the overall prevalence decreases, it's important to note that AUD in older adults often goes undiagnosed and untreated. Physical and social changes associated with aging can mask the signs of alcoholism. Additionally, older adults may be more likely to self-medicate with alcohol to cope with chronic pain, loneliness, or grief, making identification and intervention crucial.
Understanding these age-specific patterns is crucial for targeted prevention and treatment strategies. For young adults, interventions should focus on education about the risks of binge drinking, promoting healthy coping mechanisms, and fostering responsible drinking habits. For older adults, healthcare providers need to be vigilant in screening for AUD, addressing underlying mental health issues, and offering age-appropriate treatment options. By tailoring our approach to the unique needs of each age group, we can more effectively combat the pervasive problem of alcoholism in the U.S.
Diluting Ammonia: The Right Water-to-Cleaner Ratio
You may want to see also
Explore related products






![]()
Gender Differences: Men and women exhibit distinct patterns and risks for alcohol dependency
Alcoholism doesn't discriminate, but its grip tightens differently on men and women. While roughly 14.5 million Americans struggle with alcohol use disorder (AUD), men are nearly twice as likely to be affected. This disparity isn't simply a numbers game; it's a complex interplay of biology, societal norms, and psychological factors.
Men, traditionally encouraged to suppress emotions and project strength, often turn to alcohol as a coping mechanism. This "stiff upper lip" mentality can lead to higher consumption rates and a greater risk of developing AUD. Women, on the other hand, face a different set of challenges. Their bodies metabolize alcohol differently, making them more susceptible to its effects even at lower doses. A woman's body typically contains less water than a man's, leading to higher blood alcohol concentration after consuming the same amount of alcohol. This means a woman drinking two standard drinks in an hour will experience a higher BAC than a man drinking the same amount.
This biological vulnerability is compounded by societal pressures. Women are often judged more harshly for drinking, leading to a higher likelihood of hiding their consumption and delaying treatment. The "wine mom" trope, while seemingly harmless, normalizes excessive drinking as a coping mechanism for the stresses of motherhood, further blurring the lines between social drinking and dependency.
Recognizing these gender-specific risks is crucial for effective prevention and treatment. Men may benefit from programs addressing emotional expression and healthy coping mechanisms, while women may require interventions focused on challenging societal norms and providing safe spaces for seeking help.
Understanding these gender differences isn't about assigning blame, but about tailoring solutions. By acknowledging the unique challenges faced by men and women, we can develop more effective strategies to combat alcoholism and offer hope for recovery to all who struggle.
Pabst vs. Coors Original: Comparing Alcohol Content in These Beers
You may want to see also
Explore related products


$19.95 $19.95

$10 $10



![]()
Regional Variations: Certain U.S. states report higher alcoholism rates than others
Alcoholism rates in the U.S. aren't uniform—they fluctuate dramatically by state, influenced by factors like cultural norms, economic conditions, and access to healthcare. For instance, states like Wisconsin and North Dakota consistently report higher rates of binge drinking and alcohol-related deaths, often tied to colder climates and social traditions that normalize heavy drinking. Conversely, Utah and other states with significant Mormon populations exhibit lower rates due to religious prohibitions against alcohol consumption. These regional disparities highlight the interplay between local culture and individual behavior, underscoring the need for state-specific prevention strategies.
Consider the economic landscape: states with higher unemployment rates, such as West Virginia and Mississippi, often see elevated alcohol misuse as individuals turn to drinking as a coping mechanism. In contrast, wealthier states like California and New York, despite having higher alcohol availability, tend to report lower rates of alcoholism, possibly due to better access to mental health resources and public health campaigns. This suggests that addressing alcoholism requires not just individual intervention but also systemic solutions targeting economic stability and community support.
Geographic isolation also plays a role. Rural states like Montana and Wyoming face unique challenges, including limited access to treatment facilities and higher rates of alcohol-related traffic fatalities. Urban areas, while better equipped with resources, often struggle with binge drinking among younger demographics, particularly college students. Tailoring interventions to these distinct environments—such as mobile clinics in rural areas or campus-based education programs—could significantly reduce regional disparities.
Finally, policy differences between states cannot be overlooked. States with stricter alcohol regulations, such as higher taxes or limited sales hours, tend to have lower alcoholism rates. For example, Pennsylvania’s state-controlled liquor stores contrast sharply with the laissez-faire approach in states like Nevada, where alcohol is readily available 24/7. Advocates for public health could push for evidence-based policies, such as increasing alcohol taxes or restricting sales hours, to mitigate regional variations in alcoholism rates. Understanding these regional nuances is crucial for crafting effective, localized solutions to a national problem.
Alcoholism: A Gateway to Greater Health Risks
You may want to see also
Explore related products






![]()
Economic Impact: Alcoholism imposes substantial financial burdens on individuals and healthcare systems
Alcoholism doesn’t just drain personal finances; it systematically erodes economic stability for individuals and communities. Consider this: the average cost of a single inpatient rehab stay in the U.S. ranges from $6,000 to $30,000, depending on duration and facility type. For someone earning the federal minimum wage of $7.25 per hour, this equates to 827 to 4,138 work hours—or roughly 5 to 25 months of full-time labor. Even outpatient treatment, while less expensive, can cost $5,000 annually, a significant burden for the 20% of Americans who lack sufficient emergency savings. These figures exclude indirect costs like lost wages, legal fees, or increased insurance premiums, which compound the financial strain. For low-income individuals, alcoholism often becomes a debt trap, forcing trade-offs between treatment and basic needs like rent or groceries.
Now, shift the lens to healthcare systems, where alcoholism acts as a silent budget saboteur. The National Institute on Alcohol Abuse and Alcoholism estimates that alcohol-related healthcare costs totaled $28 billion in 2020, with Medicaid and Medicare covering over 40% of these expenses. Emergency room visits alone account for $1.4 billion annually, as alcohol is a factor in 20% of ER admissions. Chronic conditions like cirrhosis, pancreatitis, and alcohol-induced dementia drive long-term care costs, with liver disease treatments averaging $85,000 per patient annually. Hospitals in states with higher alcohol consumption rates, such as Wisconsin and North Dakota, report 30% higher readmission rates for alcohol-related illnesses, straining resources and inflating operational costs. These systemic burdens translate to higher insurance premiums for all, regardless of alcohol use.
To mitigate these costs, targeted interventions are critical—but they require upfront investment. For instance, implementing Screening, Brief Intervention, and Referral to Treatment (SBIRT) in primary care settings costs approximately $12 per patient but saves $300 in downstream healthcare expenses by identifying at-risk individuals early. Similarly, raising alcohol taxes by 10% could reduce consumption by 5–15%, lowering alcohol-related hospitalizations by up to 9%, according to the World Health Organization. Employers can also play a role by offering Employee Assistance Programs (EAPs), which provide free counseling and treatment referrals, reducing absenteeism and improving productivity. A study by the Harvard Business Review found that every dollar invested in EAPs yields a $3–$5 return in reduced healthcare costs and improved workplace performance.
Finally, consider the generational economic ripple effects of untreated alcoholism. Children of alcoholics are 4 times more likely to develop substance use disorders themselves, perpetuating a cycle of dependency and financial instability. These individuals often face barriers to education and employment, with 70% of incarcerated adults in the U.S. reporting substance abuse issues. Breaking this cycle requires community-based solutions, such as school-based prevention programs and affordable family therapy, which cost $50–$100 per session but can prevent thousands in future treatment and criminal justice expenses. By reframing alcoholism as a preventable economic crisis, rather than a moral failing, policymakers and individuals alike can prioritize solutions that save both lives and money.
Backpacking Stove: Filling with Alcohol Safely
You may want to see also
Explore related products






![]()
Treatment Accessibility: Many Americans face barriers to accessing effective alcoholism treatment programs
Approximately 14.5 million Americans aged 12 and older struggle with alcohol use disorder (AUD), yet only about 7.2% of them receive treatment. This staggering gap highlights a critical issue: treatment accessibility. For many, the path to recovery is obstructed by financial, logistical, and systemic barriers that perpetuate cycles of addiction. Understanding these obstacles is the first step toward dismantling them and ensuring that effective treatment is available to all who need it.
Consider the financial burden, one of the most pervasive barriers. Treatment programs can cost anywhere from $5,000 to $80,000, depending on the level of care, duration, and facility. While the Affordable Care Act mandates insurance coverage for substance use disorders, many plans impose restrictive limits on inpatient stays or require high out-of-pocket costs. For individuals without insurance—a group disproportionately affected by AUD—the expense is often insurmountable. Even those with coverage may face hidden costs, such as transportation to treatment centers or lost wages during recovery, which further limit accessibility.
Geography exacerbates these challenges, particularly in rural areas. Over 60% of rural counties in the U.S. lack a single licensed addiction treatment provider. Residents may need to travel hours to reach the nearest facility, a logistical nightmare for those without reliable transportation or support systems. Urban areas, while better equipped, often have long waitlists for publicly funded programs, leaving individuals in critical need of immediate care without options. Telehealth has emerged as a partial solution, but its effectiveness is limited by lack of broadband access in rural communities and the inability to provide essential services like detoxification remotely.
Stigma remains a silent but powerful barrier, deterring many from seeking help. Fear of judgment from employers, family, or healthcare providers often leads individuals to delay or avoid treatment altogether. This is particularly true for professionals in high-stakes careers, who may worry about the impact of disclosing their struggles on their reputation or licensure. Addressing stigma requires systemic change, including workplace policies that protect employees seeking treatment and public awareness campaigns that reframe addiction as a treatable medical condition rather than a moral failing.
To improve accessibility, a multi-faceted approach is necessary. Policymakers must expand Medicaid coverage and enforce stricter regulations on insurance providers to ensure comprehensive, affordable care. Investment in rural healthcare infrastructure, including mobile clinics and telehealth expansion, can bridge geographical gaps. Employers can play a role by offering confidential support programs and flexible leave policies for employees in treatment. Finally, destigmatizing AUD through education and media representation can encourage more individuals to seek help without fear. By tackling these barriers head-on, we can move closer to a reality where treatment is not a privilege but a right for all Americans struggling with alcoholism.
Alcohol's Impact: How Drinking Depletes Essential Nutrients in Your Body
You may want to see also
Frequently asked questions
Approximately 14.5 million Americans aged 12 and older had Alcohol Use Disorder (AUD) in 2019, according to the National Institute on Alcohol Abuse and Alcoholism (NIAAA).
About 5.8% of the U.S. population aged 12 and older, or roughly 1 in every 18 individuals, struggled with AUD in 2019, based on NIAAA data.
Yes, adults aged 18 to 25 have the highest prevalence of AUD, with about 14.5% of this age group affected, compared to 6.7% of adults aged 26 and older.
Only about 7.2% of individuals with AUD receive treatment annually, meaning millions of Americans with alcoholism do not seek or receive professional help, according to NIAAA.