Alcoholism, a chronic and often progressive disorder characterized by an inability to control or stop drinking despite adverse consequences, remains a significant public health concern in the United States. Recent data from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) estimates that approximately 14.5 million Americans aged 12 and older struggle with alcohol use disorder (AUD), representing about 5.3% of this population. This staggering figure highlights the widespread impact of alcoholism, affecting individuals across all demographics, socioeconomic backgrounds, and age groups. Understanding the prevalence of alcoholism is crucial for developing effective prevention, treatment, and support strategies to address this pervasive issue and reduce its societal and personal toll.
Explore related products






What You'll Learn
- Prevalence by Age Group: Alcoholism rates vary significantly across different age demographics in the United States
- Gender Differences: Men and women show distinct patterns in alcoholism prevalence and treatment-seeking behavior
- Regional Variations: Alcoholism rates differ by state, influenced by cultural, economic, and policy factors
- Impact of Socioeconomics: Lower income and education levels correlate with higher alcoholism rates nationally
- Trends Over Time: Alcoholism statistics have fluctuated over decades due to societal and policy changes
![]()
Prevalence by Age Group: Alcoholism rates vary significantly across different age demographics in the United States
Alcoholism doesn’t strike uniformly across the lifespan. Data reveals a clear pattern: rates of alcohol use disorder (AUD) peak in young adulthood, specifically among those aged 18-29. This age group faces a prevalence rate of approximately 14.5%, according to the National Survey on Drug Use and Health (NSDUH). Think college students grappling with newfound freedom, peer pressure, and academic stress, often turning to alcohol as a coping mechanism. Binge drinking, defined as consuming 4-5 drinks in a short period for women and men respectively, is alarmingly common in this demographic, significantly increasing the risk of developing AUD.
Early intervention is crucial. Universities and colleges should prioritize accessible mental health services, alcohol education programs, and alternative stress management strategies to combat this trend.
A stark contrast emerges when examining older adults. While overall prevalence decreases with age, individuals over 65 face unique challenges. The NSDUH reports a 1.2% AUD rate in this group, but this statistic belies a hidden struggle. Older adults often experience social isolation, grief, and chronic pain, leading to self-medication with alcohol. Additionally, age-related changes in metabolism make them more susceptible to the effects of alcohol, even at lower doses. A single drink for a 70-year-old can have the same impact as two or three for a younger person. Healthcare providers must be vigilant in screening older adults for alcohol misuse, even when consumption appears moderate.
Community programs fostering social connection and addressing age-related challenges are vital in preventing and treating AUD in this vulnerable population.
The middle ground, ages 30-64, presents a more nuanced picture. Prevalence rates hover around 6-7%, reflecting a mix of established drinking patterns and potential midlife stressors. Career pressures, family responsibilities, and financial worries can contribute to problematic drinking. Interestingly, this age group also sees a gender disparity, with men experiencing AUD at roughly twice the rate of women. Tailored interventions are key. Workplace wellness programs incorporating stress management and alcohol awareness training can be effective. Additionally, targeted campaigns addressing gender-specific risk factors are crucial for both prevention and treatment.
Understanding these age-specific patterns allows for a more targeted and effective approach to combating alcoholism in the United States. By tailoring prevention, education, and treatment strategies to the unique needs of each demographic, we can work towards reducing the overall burden of this disease.
Alcohol Exposure in Kids: Healthy or Harmful?
You may want to see also
Explore related products






![]()
Gender Differences: Men and women show distinct patterns in alcoholism prevalence and treatment-seeking behavior
Alcoholism in the United States affects millions, but the story doesn’t end with raw numbers. A closer look reveals striking gender disparities in both prevalence and treatment-seeking behavior. Men are nearly twice as likely as women to meet the criteria for alcohol dependence, with approximately 9.4% of men and 4.2% of women in the U.S. struggling with this condition, according to the National Institute on Alcohol Abuse and Alcoholism (NIAAA). This gap, however, doesn’t tell the whole story. Women, despite lower overall rates, face unique risks and challenges when it comes to alcohol misuse.
Biological differences play a significant role in these disparities. Women metabolize alcohol differently than men due to lower body water content and higher body fat percentages, meaning they reach higher blood alcohol concentrations faster and with smaller amounts of alcohol. This makes women more susceptible to alcohol-related health issues, such as liver disease and brain damage, even when consuming less than their male counterparts. For instance, a woman drinking two standard drinks per day faces a higher risk of alcohol-related harm than a man consuming the same amount. This physiological vulnerability underscores why even moderate drinking can be riskier for women.
Treatment-seeking behavior further highlights gender differences. Men are more likely to enter treatment programs for alcoholism, but women often face barriers that delay or prevent their access to care. Societal stigma, childcare responsibilities, and a lack of gender-specific treatment options are among the hurdles women encounter. Research shows that women are more likely to seek help through primary care settings rather than specialized addiction programs, often due to concerns about judgment or the inability to step away from family obligations. This disparity in treatment access means women may struggle longer before receiving the support they need.
Addressing these gender differences requires tailored approaches. For women, early intervention strategies should focus on primary care settings, where they are more likely to engage. Screening tools like the AUDIT (Alcohol Use Disorders Identification Test) can be integrated into routine health visits to identify at-risk individuals. For men, destigmatizing treatment-seeking behavior and promoting awareness of the long-term health consequences of alcohol misuse could encourage earlier intervention. Both genders would benefit from programs that address the unique social and biological factors contributing to their alcohol use.
In practical terms, individuals and healthcare providers can take specific steps to mitigate these risks. Women should be aware of the NIAAA’s recommendation to limit alcohol intake to one standard drink per day, while men should cap consumption at two. Partners, friends, and family members can play a role by fostering open conversations about alcohol use and supporting loved ones in seeking help. Ultimately, recognizing and addressing these gender-specific patterns is crucial for reducing the overall burden of alcoholism in the U.S. and ensuring that everyone, regardless of gender, has access to effective care.
Alcoholism: Disease or Not? Impact of the Label
You may want to see also
Explore related products






![]()
Regional Variations: Alcoholism rates differ by state, influenced by cultural, economic, and policy factors
Alcoholism rates in the U.S. are not uniform; they fluctuate dramatically across states, revealing a complex interplay of cultural, economic, and policy influences. For instance, states like Wisconsin and North Dakota consistently report higher rates of excessive drinking, often attributed to a deeply ingrained drinking culture and colder climates that encourage indoor socializing. Conversely, Utah and Mississippi exhibit lower rates, influenced by religious norms and restrictive alcohol policies. These variations underscore the importance of understanding local contexts when addressing alcohol-related issues.
Consider the economic factors at play. States with higher unemployment rates, such as West Virginia and Kentucky, often see elevated alcohol misuse as individuals turn to drinking as a coping mechanism. In contrast, wealthier states like California and New York, despite having higher alcohol availability, may have lower rates of alcoholism due to better access to healthcare and mental health resources. This disparity highlights the need for targeted interventions that address both economic stressors and substance abuse.
Policy measures also play a pivotal role in shaping regional alcoholism rates. States with stricter alcohol laws, such as higher taxes on alcohol or limited sales hours, tend to have lower consumption rates. For example, Pennsylvania’s state-controlled liquor stores contrast sharply with the laissez-faire approach in states like Louisiana, where alcohol is readily available in gas stations and grocery stores. Such policy differences directly impact accessibility and, consequently, consumption patterns.
Cultural attitudes toward alcohol further complicate the picture. In the South, social drinking is often intertwined with hospitality and tradition, which can normalize heavy drinking. Meanwhile, in the Northeast, urban lifestyles and a fast-paced culture may contribute to higher rates of binge drinking among younger adults. Understanding these cultural nuances is essential for crafting effective prevention and treatment strategies that resonate with specific communities.
To address regional variations in alcoholism, policymakers and health advocates must adopt a tailored approach. For high-risk states, initiatives could include economic development programs to reduce unemployment, stricter enforcement of alcohol laws, and culturally sensitive public health campaigns. In states with lower rates, maintaining vigilance and promoting healthy drinking norms remain crucial. By acknowledging the unique factors driving alcoholism in each region, we can move beyond one-size-fits-all solutions and make meaningful progress in reducing alcohol-related harm nationwide.
Can Dogs Safely Consume Alcohol? Risks and Dangers Explained
You may want to see also
Explore related products






![]()
Impact of Socioeconomics: Lower income and education levels correlate with higher alcoholism rates nationally
Socioeconomic status plays a pivotal role in shaping health outcomes, and alcoholism is no exception. National data consistently reveals a stark correlation: individuals with lower income and education levels are disproportionately affected by alcohol use disorder (AUD). For instance, a 2020 study by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) found that adults with household incomes below $25,000 were nearly twice as likely to experience AUD compared to those earning over $75,000 annually. This disparity underscores the need to examine the underlying mechanisms linking socioeconomic factors to alcohol dependency.
Consider the daily stressors faced by low-income individuals: financial instability, job insecurity, and limited access to healthcare. These pressures often create a fertile ground for alcohol misuse as a coping mechanism. Unlike higher-income counterparts, who may have access to therapy, wellness programs, or stress-management resources, lower-income individuals frequently turn to alcohol as an affordable and readily available escape. For example, a six-pack of beer or a bottle of liquor can cost as little as $5—a seemingly small price to pay for temporary relief from overwhelming stress. However, this short-term solution often spirals into long-term dependency, exacerbating both health and financial burdens.
Education levels further compound this issue. Individuals with lower educational attainment are less likely to receive comprehensive health education, including the risks associated with excessive drinking. A high school dropout, for instance, may lack awareness of the recommended alcohol limits—up to one drink per day for women and up to two for men, according to the Dietary Guidelines for Americans. Without this knowledge, they may engage in binge drinking (defined as 4 or more drinks for women and 5 or more for men in about 2 hours) without understanding the heightened risk of developing AUD. Education also influences career opportunities, with higher-paying jobs often requiring advanced degrees, leaving those with less education in roles that may perpetuate financial strain and stress.
Addressing this socioeconomic gap requires targeted interventions. Public health initiatives should focus on making affordable mental health services and addiction treatment accessible to low-income communities. For example, community health centers could offer sliding-scale therapy sessions or free support groups like Alcoholics Anonymous. Schools in underserved areas should integrate substance abuse education into curricula, ensuring students understand the risks of alcohol misuse from a young age. Additionally, policymakers could advocate for higher minimum wages or expanded social safety nets to alleviate the financial stressors that drive alcohol dependency.
In conclusion, the correlation between lower socioeconomic status and higher alcoholism rates is not merely a statistical anomaly but a reflection of systemic inequalities. By addressing the root causes—financial instability, limited access to resources, and inadequate education—society can mitigate the disproportionate impact of AUD on vulnerable populations. Practical steps, from community-based interventions to policy reforms, are essential to breaking the cycle of alcohol dependency among those most at risk.
Does Benzyl Alcohol Burn? Understanding Its Flammability and Safety
You may want to see also
Explore related products






![]()
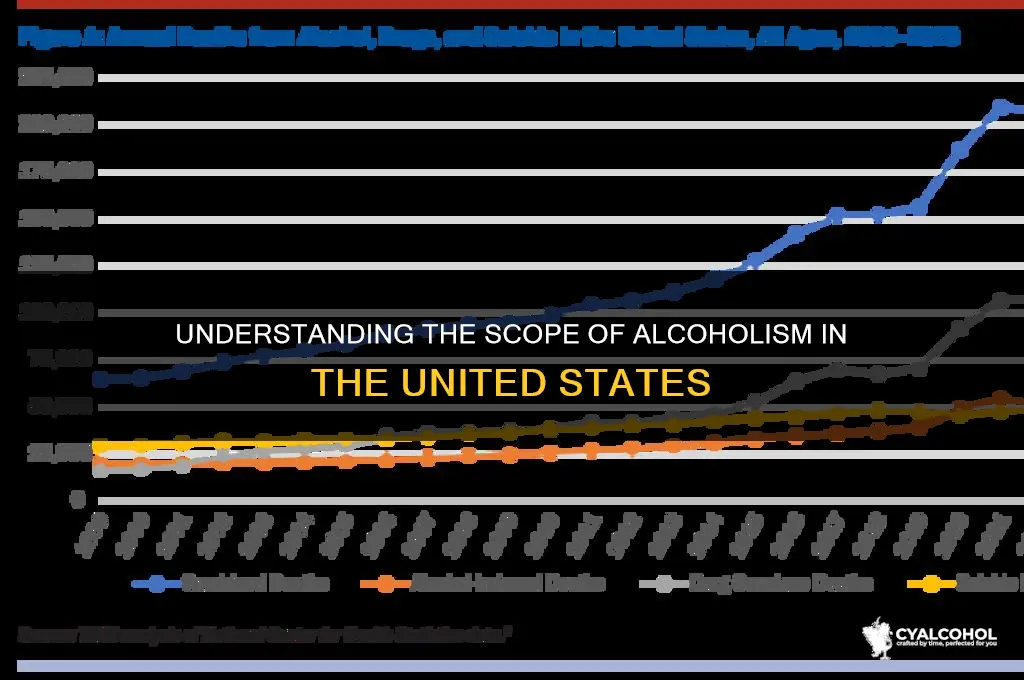
Trends Over Time: Alcoholism statistics have fluctuated over decades due to societal and policy changes
Alcoholism rates in the U.S. have not followed a straight line. Since the 1970s, when roughly 15% of adults met criteria for alcohol dependence, the prevalence has oscillated between 7% and 10%, according to data from the National Survey on Drug Use and Health. These shifts aren’t random—they mirror broader societal currents and policy interventions. For instance, the 1980s saw a sharp decline in alcoholism rates coinciding with the implementation of stricter drunk-driving laws and public awareness campaigns like "Friends Don’t Let Friends Drive Drunk." This period demonstrated how policy and cultural attitudes can directly influence behavior, reducing alcohol-related harm and dependency.
Consider the demographic breakdown: among adults aged 18–25, alcoholism rates peaked in the early 2000s at nearly 12%, likely fueled by binge-drinking culture on college campuses. In contrast, rates among adults over 50 have remained relatively stable, hovering around 5%. This disparity highlights the impact of generational trends and targeted interventions. For example, campus-based programs promoting responsible drinking and stricter enforcement of underage drinking laws have contributed to a gradual decline in young adult alcoholism rates since 2010. Meanwhile, older adults, often overlooked in prevention efforts, may benefit from initiatives addressing age-related stressors like retirement or isolation.
A closer look at gender reveals another layer of fluctuation. Historically, men have had higher alcoholism rates than women, with a 2:1 ratio in the 1980s. However, this gap has narrowed significantly, with women’s rates increasing by 85% between 2002 and 2019, compared to a 35% increase among men. This shift coincides with changing societal roles, marketing strategies targeting women, and rising stress levels. For instance, wine culture has been heavily marketed to women as a form of relaxation, with phrases like "mommy juice" normalizing daily drinking. Addressing this trend requires gender-specific interventions, such as campaigns challenging the normalization of alcohol as self-care.
Policy changes continue to play a pivotal role. The 2016 Surgeon General’s report on alcohol, the first in over 30 years, called for a comprehensive approach to reduce excessive drinking. Since then, states like Utah have lowered the legal BAC limit to 0.05%, while others have expanded access to telehealth for addiction treatment. Early data suggests these measures are having an impact: emergency room visits related to alcohol declined by 5% in states with stricter policies between 2018 and 2022. However, challenges remain, particularly in rural areas where treatment access is limited. Policymakers must balance enforcement with support, ensuring that those struggling with alcoholism have pathways to recovery.
Finally, economic factors cannot be ignored. During the 2008 recession, alcoholism rates ticked upward, particularly among middle-aged men facing job loss and financial strain. Conversely, the COVID-19 pandemic saw a 14% increase in alcohol sales in 2020, yet alcoholism rates remained stable, possibly due to reduced social drinking opportunities. These examples underscore the need for proactive measures during crises, such as integrating mental health screenings into unemployment services or expanding virtual support groups. By understanding these trends, we can design interventions that not only respond to current challenges but also anticipate future shifts in alcohol use patterns.
The Fruit-Forward: Understanding Alcohol's Fruitiest Flavors
You may want to see also
Frequently asked questions
As of recent estimates, approximately 14.5 million Americans aged 12 and older are classified as having Alcohol Use Disorder (AUD), commonly referred to as alcoholism.
The 14.5 million alcoholics represent about 5.3% of the U.S. population aged 12 and older, based on data from the National Survey on Drug Use and Health (NSDUH).
Men are more likely to be alcoholics, with about 9.0% of men aged 12 and older having AUD, compared to 5.7% of women in the same age group.
Among young adults aged 18–25, approximately 10.5% meet the criteria for AUD, making this age group the most affected by alcoholism in the United States.