The question of how many alcohol drinkers are alcoholics is a complex and nuanced issue, as it involves distinguishing between moderate, social drinking and problematic alcohol use. While many individuals consume alcohol without developing dependency, a significant portion of drinkers may fall into patterns of misuse or addiction. According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA), approximately 14.5 million adults in the United States alone struggle with alcohol use disorder (AUD), representing a small but concerning fraction of the overall drinking population. Factors such as genetics, environment, and mental health play a role in determining who may develop alcoholism, making it essential to approach the topic with an understanding of both individual risk factors and broader societal trends.
Explore related products





What You'll Learn
- Prevalence of Alcoholism: Percentage of drinkers meeting clinical criteria for alcohol use disorder (AUD)
- Social vs. Dependent Drinking: Distinguishing between casual consumption and problematic alcohol dependence
- Risk Factors for AUD: Genetic, environmental, and behavioral factors contributing to alcoholism development
- Diagnosis Challenges: Difficulty in identifying alcoholics due to stigma, denial, and varying symptoms
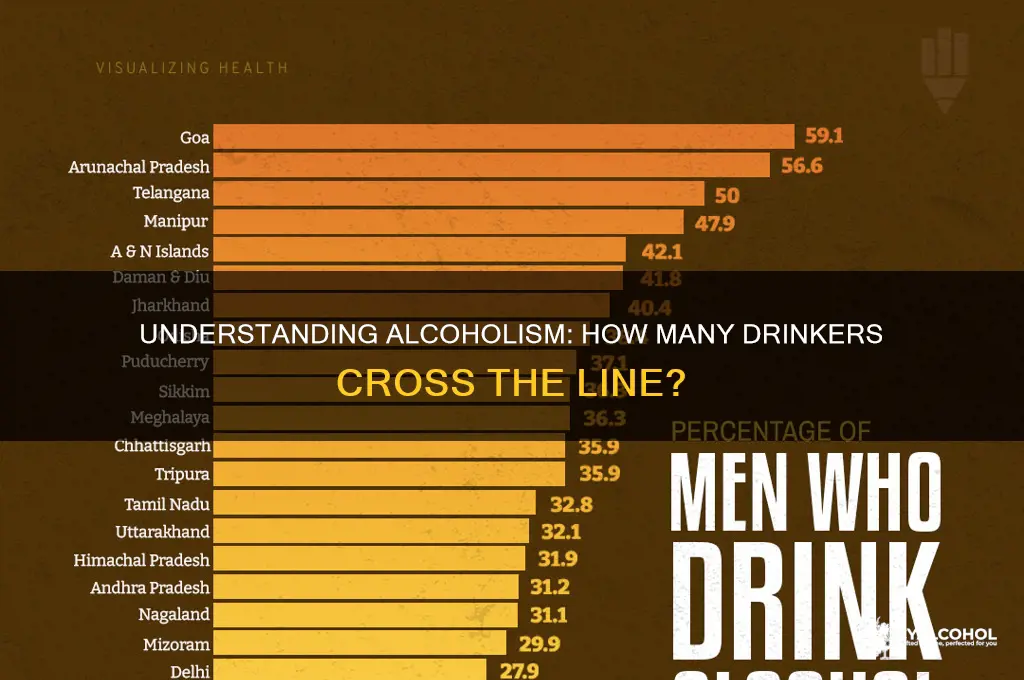
- Global vs. Regional Statistics: Comparing alcoholism rates across countries and cultural drinking patterns
![]()
Prevalence of Alcoholism: Percentage of drinkers meeting clinical criteria for alcohol use disorder (AUD)
Alcohol consumption is a widespread social practice, but the line between casual drinking and alcoholism is often blurred. According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA), approximately 14.5 million adults aged 18 and older in the United States meet the clinical criteria for Alcohol Use Disorder (AUD). This represents roughly 5.8% of the adult population. Strikingly, this figure does not include younger individuals under 18, who may also exhibit problematic drinking behaviors. Understanding this prevalence is crucial, as AUD is a chronic relapsing brain disorder characterized by an impaired ability to stop or control alcohol use despite adverse social, occupational, or health consequences.
To contextualize these numbers, consider that not all heavy drinkers are alcoholics, but all alcoholics are heavy drinkers. The NIAAA defines heavy drinking as consuming 4 or more drinks on any day for men and 3 or more drinks for women. However, meeting the criteria for AUD involves more than just quantity. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) outlines 11 criteria, including cravings, withdrawal symptoms, and continued use despite negative consequences. A person meeting 2 or more of these criteria within a 12-month period is diagnosed with AUD. This distinction highlights that alcoholism is not solely about how much one drinks but also about the loss of control and the impact on daily life.
Age and demographics play a significant role in the prevalence of AUD. For instance, young adults aged 18–25 have the highest rates of AUD, with 14.1% meeting the criteria. This is often attributed to the normalization of binge drinking in college and social settings. In contrast, only 1.4% of adults aged 65 and older meet the criteria, possibly due to health concerns or lifestyle changes. Gender also influences these statistics: men are twice as likely as women to develop AUD, with 9.4% of men and 4.9% of women affected. These disparities underscore the importance of tailored interventions that address specific risk factors within different populations.
Practical steps can be taken to identify and address AUD early. For individuals, monitoring drinking patterns and being honest about behaviors like drinking alone or hiding alcohol consumption is essential. Tools such as the CAGE questionnaire (a four-question screening test) or the AUDIT (Alcohol Use Disorders Identification Test) can help assess risk. For healthcare providers, routine screenings during check-ups can facilitate early detection. Treatment options range from behavioral therapies and medications like naltrexone to support groups such as Alcoholics Anonymous. The key is recognizing that AUD is a treatable condition, and seeking help is a sign of strength, not weakness.
In conclusion, while alcohol is a common part of many cultures, the prevalence of AUD—affecting nearly 6% of adults—demands attention. By understanding the clinical criteria, demographic trends, and available resources, individuals and communities can take proactive steps to mitigate the risks associated with alcoholism. Awareness and early intervention are vital in reducing the personal and societal toll of this disorder.
Can Alcoholics Overcome Cravings? Understanding Long-Term Recovery Challenges
You may want to see also
Explore related products






![]()
Social vs. Dependent Drinking: Distinguishing between casual consumption and problematic alcohol dependence
Alcohol consumption is a spectrum, with social drinking on one end and dependence on the other. Understanding the difference is crucial, as estimates suggest only about 10-15% of drinkers develop alcoholism, yet the line between casual use and problematic behavior can blur easily. Social drinking typically involves moderate, controlled intake—defined by the NIH as up to 1 drink per day for women and 2 for men—often in settings like dinners or celebrations. It’s purposeful, not compulsive, and doesn’t interfere with daily life. Dependent drinking, however, is marked by a loss of control, increased tolerance, and negative consequences such as health issues or strained relationships. Recognizing where on this spectrum an individual falls requires honest self-assessment and awareness of behavioral patterns.
Consider the context and frequency of drinking as a starting point for distinction. Social drinkers often adhere to unwritten rules: they rarely drink alone, limit intake in professional settings, and can abstain without discomfort. Dependent drinkers, in contrast, may use alcohol as a coping mechanism, drink in secrecy, or prioritize it over responsibilities. For instance, a social drinker might enjoy a glass of wine with dinner, while a dependent drinker might start the day with a drink to alleviate withdrawal symptoms. Tracking consumption—such as noting how many days per week alcohol is consumed—can provide clarity. If drinking exceeds 3-4 days weekly or involves binge drinking (4+ drinks for women, 5+ for men in 2 hours), it may signal a shift toward dependence.
Physical and psychological indicators further differentiate these behaviors. Social drinkers rarely experience cravings or withdrawal symptoms like tremors, anxiety, or nausea when abstaining. Dependent drinkers, however, often face these symptoms, which reinforce the cycle of consumption. Additionally, dependent drinking rewires the brain’s reward system, making it harder to derive pleasure from non-alcohol-related activities. Practical tips for self-evaluation include keeping a drinking diary, setting limits (e.g., no drinking on weekdays), and monitoring emotional responses to abstinence. If cutting back feels impossible or triggers distress, it’s a red flag for dependence.
Addressing dependent drinking requires a multifaceted approach. Unlike social drinking, which can be self-regulated, dependence often necessitates professional intervention. Treatment options range from therapy and support groups like AA to medications such as naltrexone or disulfiram. Early intervention is key—studies show that individuals who seek help within the first 5 years of problematic drinking have higher recovery rates. For those unsure of their status, screening tools like the AUDIT (Alcohol Use Disorders Identification Test) offer a structured way to assess risk. Ultimately, distinguishing between social and dependent drinking isn’t about judgment but about fostering a healthier relationship with alcohol, one informed by self-awareness and proactive measures.
Minimize Morning Odor: Alcohols That Leave Little to No Scent
You may want to see also
Explore related products


![DSS Games Who's Most Likely to...Kinda Clean Family Edition [A Party Game | Great for Adults & Teens | White Elephant Gift, Stocking Stuffer | Game Nights & Big Groups]](https://m.media-amazon.com/images/I/61h3VO1t3VL._AC_UL320_.jpg)



![]()
Risk Factors for AUD: Genetic, environmental, and behavioral factors contributing to alcoholism development
Not all alcohol drinkers are alcoholics, but understanding who is at risk for developing Alcohol Use Disorder (AUD) is crucial for prevention and early intervention. Approximately 14.5 million Americans aged 12 and older struggle with AUD, yet only a fraction receive treatment. This disparity highlights the importance of identifying risk factors that contribute to the development of alcoholism. Among these, genetic, environmental, and behavioral factors play significant roles, often intertwining to create a complex web of vulnerability.
Genetic predisposition acts as a silent contributor to AUD risk. Research indicates that genetics account for about 40-60% of the risk for alcoholism. Specific genes, such as those involved in alcohol metabolism (e.g., ADH1B and ALDH2), influence how the body processes alcohol. For instance, individuals with certain variants of these genes may experience unpleasant side effects like flushing, nausea, or rapid heartbeat after drinking, which can deter excessive consumption. Conversely, those without these variants may metabolize alcohol more efficiently, increasing their risk of developing AUD. Family history is another critical marker; having a first-degree relative with AUD can double or triple one’s risk. Understanding genetic risk allows for targeted interventions, such as genetic counseling or personalized treatment plans.
Environmental factors shape the landscape in which AUD develops. Exposure to alcohol at an early age, particularly before 15, significantly elevates the risk of AUD later in life. This is partly due to the developing brain’s heightened sensitivity to alcohol’s neurotoxic effects. Socioeconomic factors, such as poverty or lack of access to education, also contribute by limiting opportunities and increasing stress. Social environments, including peer pressure or living in communities with high alcohol availability, further amplify risk. For example, individuals in neighborhoods with a high density of liquor stores are more likely to engage in heavy drinking. Addressing these environmental risks requires systemic changes, such as stricter alcohol regulations and community-based prevention programs.
Behavioral patterns often serve as both indicators and accelerants of AUD risk. Regular binge drinking, defined as consuming 4 or more drinks (for women) or 5 or more drinks (for men) in about 2 hours, is a red flag. This behavior not only increases tolerance but also alters brain chemistry, making it harder to stop drinking. Co-occurring mental health disorders, such as depression or anxiety, frequently exacerbate the risk, as individuals may use alcohol as a coping mechanism. Practical steps to mitigate behavioral risks include setting strict drinking limits, engaging in stress-reducing activities like exercise or meditation, and seeking therapy for underlying mental health issues. Early intervention, such as brief counseling sessions, can also prevent mild AUD from progressing to severe stages.
The interplay of these factors underscores the need for a multifaceted approach to AUD prevention. For instance, a person with a genetic predisposition who grows up in an environment where alcohol is normalized and develops unhealthy coping mechanisms is at exponentially higher risk. By addressing genetic vulnerabilities through personalized medicine, modifying environmental triggers through policy and community action, and fostering healthier behaviors through education and support, the incidence of AUD can be significantly reduced. Recognizing these risk factors empowers individuals and communities to take proactive steps toward a healthier relationship with alcohol.
Quitting Alcohol and Chest Colds: Unraveling the Connection and Symptoms
You may want to see also
Explore related products

![DSS Games You Laugh You're Out [Try Not to Laugh Family Card Game for Adults & Teens | White Elephant Gift for Adults | 125 Prompt Fun Cards for Family Game Nights, & Holiday Parties Ages 14+]](https://m.media-amazon.com/images/I/71lk77mQeUL._AC_UL320_.jpg)




![]()
Diagnosis Challenges: Difficulty in identifying alcoholics due to stigma, denial, and varying symptoms
Stigma casts a long shadow over alcoholism, often preventing individuals from seeking help or even acknowledging their problem. Society’s judgmental gaze labels alcoholics as weak-willed or morally flawed, fostering shame and secrecy. This stigma doesn’t just affect public perception—it seeps into healthcare settings, where fear of judgment discourages honest conversations about drinking habits. For instance, a 2019 study in the *Journal of Addiction Medicine* found that 60% of patients underreported their alcohol consumption during medical visits due to embarrassment. This reluctance to disclose the full extent of their drinking complicates diagnosis, as healthcare providers rely on self-reported data to assess risk. Without accurate information, even the most well-intentioned professionals may miss critical signs of alcoholism.
Denial is another formidable barrier, not just for the drinker but for those around them. Alcoholics often minimize their drinking, rationalize excessive consumption, or compare themselves to "worse" cases to avoid confronting the reality of their addiction. This psychological defense mechanism is so powerful that it can distort self-awareness, making it nearly impossible for individuals to recognize their own dependency. For example, a person might claim they only drink socially, even if they consume 5–6 drinks per occasion multiple times a week—a pattern that exceeds the National Institute on Alcohol Abuse and Alcoholism’s (NIAAA) definition of moderate drinking (up to 1 drink per day for women, 2 for men). Loved ones may also enable denial by avoiding difficult conversations or downplaying concerns, further delaying intervention.
The variability of alcoholism symptoms adds another layer of complexity to diagnosis. Unlike conditions with clear biomarkers, alcoholism presents differently across individuals. Some may experience severe physical withdrawal symptoms like tremors or seizures, while others struggle primarily with psychological dependence. Age, gender, and genetic predisposition further influence how alcoholism manifests. For instance, younger drinkers may exhibit more outward signs of binge drinking, while older adults might hide their habit due to societal expectations. This lack of uniformity means that even experienced clinicians can struggle to identify alcoholism without a comprehensive assessment. Tools like the AUDIT (Alcohol Use Disorders Identification Test) help, but they require honest responses—something stigma and denial often obstruct.
Practical steps can mitigate these challenges, though they require sensitivity and persistence. Healthcare providers should create nonjudgmental environments where patients feel safe discussing their drinking habits. Screening questions should be framed neutrally, focusing on behavior rather than morality. For example, instead of asking, “Do you think you have a drinking problem?” providers might ask, “How many days per week do you have more than 2 drinks?” Family members can also play a role by approaching conversations with empathy, using specific examples of concerning behavior rather than accusatory language. For instance, saying, “I’ve noticed you seem more irritable after drinking lately,” is less confrontational than labeling someone an alcoholic. Early intervention is key, as addressing problematic drinking before it escalates increases the likelihood of successful treatment.
Ultimately, overcoming diagnosis challenges requires a shift in societal attitudes and individual awareness. Stigma must be replaced with compassion, denial with honesty, and ambiguity with clarity. By fostering an environment where alcoholism is treated as a medical condition rather than a moral failing, we can encourage more people to seek help. Until then, the true number of alcoholics among drinkers will remain obscured, leaving countless individuals to suffer in silence.
Why Alcohol Triggers Diarrhea: Understanding the Digestive Impact
You may want to see also
Explore related products






![]()
Global vs. Regional Statistics: Comparing alcoholism rates across countries and cultural drinking patterns
Alcoholism rates vary dramatically across the globe, influenced by cultural norms, economic factors, and regional policies. For instance, Eastern European countries like Belarus and Lithuania report some of the highest per capita alcohol consumption rates, with over 14 liters of pure alcohol consumed annually per person, compared to less than 2 liters in countries like Indonesia and Kuwait. These disparities highlight how regional drinking patterns shape alcoholism prevalence, with binge drinking cultures in Eastern Europe contributing to higher rates of alcohol use disorder (AUD).
To compare alcoholism rates effectively, consider the diagnostic criteria for AUD, which includes symptoms like inability to cut down, withdrawal, and continued use despite negative consequences. Globally, the World Health Organization estimates that 5.1% of the population aged 15 and older suffers from AUD, but regional variations are stark. In Russia, for example, studies suggest AUD affects up to 10% of the adult population, while in the United States, the figure hovers around 7%. Conversely, countries with predominantly Muslim populations, such as Saudi Arabia, report AUD rates below 1%, reflecting cultural and religious prohibitions on alcohol consumption.
Cultural drinking patterns play a pivotal role in these statistics. In Mediterranean countries like Italy and Spain, alcohol is often consumed in moderation with meals, leading to lower AUD rates despite relatively high per capita consumption. This contrasts with Nordic countries like Finland, where binge drinking is more common, resulting in higher AUD prevalence. Understanding these patterns can inform public health strategies, such as promoting moderate drinking norms or implementing stricter alcohol control measures in high-risk regions.
When analyzing these statistics, it’s crucial to account for underreporting and varying diagnostic methods. For example, stigma surrounding alcoholism in some cultures may lead to lower self-reported rates, while countries with robust healthcare systems may identify cases more accurately. Practical tips for policymakers include tailoring interventions to regional drinking cultures—such as education campaigns in binge-drinking regions or economic incentives for moderation in high-consumption areas. By addressing these nuances, global and regional comparisons can drive more effective strategies to combat alcoholism.
Alcohol Sales Tax Hike: Impact and Implications
You may want to see also
Frequently asked questions
It’s estimated that about 10-15% of alcohol drinkers develop alcohol use disorder (AUD), commonly referred to as alcoholism.
Not necessarily. Daily drinking alone doesn’t define alcoholism; it depends on the quantity, frequency, and impact on one’s life. Alcoholism is diagnosed based on criteria like loss of control, withdrawal symptoms, and negative consequences.
Yes, social drinking can progress to alcoholism if consumption increases, tolerance develops, or drinking begins to interfere with daily life and responsibilities.
Yes, men are generally more likely to develop alcoholism than women, but women may progress from casual drinking to addiction more quickly due to biological differences.
Signs include inability to stop drinking, neglecting responsibilities, withdrawal symptoms, and continued drinking despite negative consequences. Professional assessment is recommended for an accurate diagnosis.