Alcohol-related deaths have been a significant public health concern globally, with far-reaching consequences for individuals, families, and societies. Since 1996, the number of alcohol-attributable fatalities has steadily risen, reflecting the pervasive impact of excessive alcohol consumption on mortality rates. Factors such as increased availability, changing social norms, and inadequate prevention strategies have contributed to this alarming trend. Understanding the scale and trajectory of alcohol-related deaths since 1996 is crucial for informing policy interventions, raising awareness, and addressing the underlying causes of this preventable public health crisis.
| Characteristics | Values |
|---|---|
| Total Alcohol-Related Deaths (1996-2020) | Approximately 1,000,000 (U.S. data, CDC) |
| Annual Alcohol-Related Deaths (2020) | ~99,000 (U.S., CDC) |
| Leading Cause of Alcohol Deaths | Liver disease, alcohol poisoning, accidents, and cardiovascular issues |
| Gender Disparity | Males account for ~70% of alcohol-related deaths (global average) |
| Age Group Most Affected | 45-64 years old (highest mortality rate) |
| Global Alcohol Deaths (Annually) | ~3 million (WHO, 2018) |
| Economic Cost (U.S. Annually) | ~$249 billion (CDC, 2010 data, adjusted for inflation) |
| Trend Since 1996 | Steady increase, with a sharp rise during the COVID-19 pandemic |
| Preventable Deaths Percentage | ~50% of alcohol-related deaths are preventable (global estimates) |
Explore related products






What You'll Learn
- Annual Alcohol-Related Deaths: Trends in alcohol-attributable fatalities from 1996 to present
- Geographic Variations: Regional differences in alcohol-related mortality rates globally
- Age and Gender Impact: How age and gender influence alcohol-related death statistics
- Cause-Specific Deaths: Breakdown of deaths by liver disease, accidents, or other alcohol-linked causes
- Policy Effects: Influence of alcohol regulations and public health initiatives on death rates
![]()
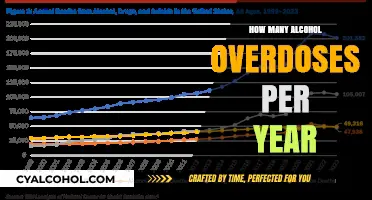
Annual Alcohol-Related Deaths: Trends in alcohol-attributable fatalities from 1996 to present
Since 1996, alcohol-related deaths have shown a troubling upward trajectory, with global estimates suggesting a rise from approximately 1.4 million deaths annually in the late 1990s to over 3 million in recent years. This increase is not uniform across regions or demographics, highlighting the complexity of the issue. For instance, Eastern Europe has historically reported some of the highest rates, with alcohol-attributable fatalities often linked to heavy drinking cultures and limited public health interventions. In contrast, North America and Western Europe have seen more modest increases, though specific age groups, such as middle-aged adults, have experienced alarming spikes in deaths related to alcohol-induced liver disease and accidents.
Analyzing the data reveals that the types of alcohol-related deaths have shifted over time. In the late 1990s, acute incidents like drunk-driving fatalities dominated the statistics, driven by lax enforcement of drunk-driving laws in many countries. However, since the mid-2000s, chronic conditions such as cirrhosis, cardiovascular diseases, and cancers attributable to long-term alcohol consumption have become the leading causes. This shift underscores the need for public health strategies that address both binge drinking and sustained, moderate-to-high alcohol intake. For example, a 2021 study found that individuals consuming more than 14 standard drinks per week faced a 20% higher risk of alcohol-related mortality compared to those who drank less.
A comparative analysis between genders and age groups further illuminates the trends. Men consistently account for a disproportionate share of alcohol-related deaths, with rates often 2–3 times higher than women. However, the gap is narrowing, particularly among younger women, as binge drinking among females aged 18–25 has increased by 40% since 1996 in some countries. Among age groups, the 45–64 cohort has seen the steepest rise in fatalities, often attributed to the cumulative effects of decades of drinking and the onset of age-related health issues. This demographic shift has significant implications for healthcare systems, as these individuals often require intensive, long-term treatment for conditions like alcoholic hepatitis.
To address these trends, practical interventions must be tailored to specific populations. For younger adults, school-based education programs and stricter enforcement of underage drinking laws can curb early alcohol initiation. For middle-aged individuals, workplace wellness initiatives and routine health screenings could identify at-risk drinkers early. Policymakers should also consider evidence-based measures like increasing alcohol taxes, limiting advertising, and reducing availability in high-risk areas. For instance, countries that implemented minimum unit pricing for alcohol saw a 20% reduction in alcohol-related hospital admissions within two years.
In conclusion, the trends in alcohol-attributable fatalities since 1996 demand a multifaceted response. While global numbers have risen, understanding the regional, demographic, and causal variations allows for targeted interventions. By combining data-driven policies with community-level actions, societies can mitigate the growing toll of alcohol-related deaths and foster healthier drinking cultures.
Removing Alcohol Marker Stains from Wood
You may want to see also
Explore related products






![]()
Geographic Variations: Regional differences in alcohol-related mortality rates globally
Alcohol-related mortality rates vary dramatically across the globe, reflecting a complex interplay of cultural, economic, and policy factors. Eastern Europe, for instance, consistently reports some of the highest rates, with countries like Russia and Belarus experiencing over 20 alcohol-attributable deaths per 100,000 people annually. This contrasts sharply with regions like North Africa and the Middle East, where religious and cultural norms significantly limit alcohol consumption, resulting in rates often below 1 per 100,000. Such disparities highlight the influence of societal attitudes and traditions on drinking behaviors and their lethal consequences.
Consider the role of policy in shaping these geographic variations. In Scandinavia, despite high per capita alcohol consumption, stringent alcohol control measures—such as state monopolies on sales and high taxation—have helped mitigate mortality rates. Conversely, in parts of Africa and Latin America, weak regulatory frameworks and the prevalence of informal alcohol markets contribute to higher rates of alcohol-related deaths, particularly among younger age groups. For policymakers, these examples underscore the importance of tailored interventions that address regional specifics rather than adopting one-size-fits-all strategies.
A comparative analysis reveals that age and gender further stratify these regional differences. In high-income countries, alcohol-related deaths are predominantly seen in older adults, often linked to chronic conditions like liver disease. In contrast, low- and middle-income regions witness a higher proportion of deaths among younger men, frequently due to acute causes such as accidents or violence. This divergence suggests that prevention efforts must be age- and gender-specific, focusing on binge drinking interventions for youth in some areas and chronic disease management for older populations in others.
Practical tips for addressing these geographic variations include leveraging local data to identify at-risk populations and implementing culturally sensitive public health campaigns. For example, in regions with high rates of alcohol-related traffic fatalities, targeted enforcement of drunk-driving laws coupled with community education can yield significant reductions. Similarly, in areas where alcohol is deeply embedded in social practices, promoting moderate drinking through traditional media or community leaders may be more effective than blanket messaging. Understanding these nuances is key to crafting interventions that resonate locally and drive meaningful change.
Alcohol Addiction: Unraveling the Truths and Misconceptions
You may want to see also
Explore related products
![McKesson Isopropyl Rubbing Alcohol 70% [12 Count] USP First Aid Antiseptic, 16 oz](https://m.media-amazon.com/images/I/614SGew9G8L._AC_UY218_.jpg)




![]()
Age and Gender Impact: How age and gender influence alcohol-related death statistics
Alcohol-related deaths have shown distinct patterns when broken down by age and gender, revealing critical insights into vulnerability and risk factors. Since 1996, data consistently highlights that men account for a disproportionately higher number of alcohol-attributable deaths compared to women, often at a ratio of 2:1 or greater. This disparity is partly due to higher consumption rates among men, but biological differences also play a role. Women, on average, metabolize alcohol less efficiently due to lower body water content and higher fat-to-muscle ratio, making them more susceptible to liver damage and other alcohol-related health issues at lower consumption levels. However, this does not diminish the severity of alcohol’s impact on men, who often face societal pressures to drink heavily, leading to chronic conditions like cirrhosis and cardiovascular disease.
Age further complicates this landscape, with middle-aged adults (45–64) emerging as the most at-risk group for alcohol-related mortality. This demographic often juggles stressors such as career demands, financial pressures, and health decline, turning to alcohol as a coping mechanism. For instance, studies show that individuals in this age bracket are more likely to engage in binge drinking episodes, defined as consuming 5 or more drinks (for men) or 4 or more drinks (for women) in a single occasion. The cumulative effect of long-term alcohol use in this age group manifests in higher rates of liver disease, cancer, and accidental injuries. Conversely, younger adults (18–34) face risks tied to acute alcohol poisoning and accidents, while older adults (65+) are more prone to medication interactions and falls exacerbated by alcohol consumption.
Practical steps can mitigate these risks across age and gender groups. For middle-aged individuals, stress management techniques like mindfulness or therapy can reduce reliance on alcohol. Younger adults benefit from education on safe drinking limits and the dangers of mixing alcohol with energy drinks or drugs. Older adults should consult healthcare providers to review potential alcohol interactions with medications. Regardless of age, setting personal drinking limits—such as adhering to the CDC’s recommendation of up to 1 drink per day for women and 2 for men—can significantly lower health risks.
A comparative analysis of global trends underscores the influence of cultural norms on these statistics. Countries with higher societal acceptance of heavy drinking, such as Russia or Eastern European nations, report starker gender disparities in alcohol-related deaths. In contrast, regions with stricter alcohol policies or cultural taboos, like parts of the Middle East, show lower overall mortality rates but still exhibit age-related vulnerabilities. This suggests that while biology and age are immutable factors, policy and cultural shifts can mitigate risks, offering a pathway to reduce alcohol-attributable deaths across demographics.
Ultimately, understanding the interplay of age and gender in alcohol-related mortality is not just academic—it’s actionable. Tailored interventions, such as gender-specific treatment programs or age-targeted public health campaigns, can address unique risk factors. For example, women-only support groups may provide a safe space to discuss alcohol dependence, while workplace wellness programs could target middle-aged professionals. By acknowledging these differences, societies can move beyond one-size-fits-all approaches to create more effective strategies for prevention and treatment, potentially reversing the alarming trends observed since 1996.
Does AmeriHealth Insurance Cover Alcohol Rehab? What You Need to Know
You may want to see also
Explore related products




![]()
Cause-Specific Deaths: Breakdown of deaths by liver disease, accidents, or other alcohol-linked causes
Alcohol-related deaths are not a singular phenomenon but a complex web of cause-specific fatalities, each with its own trajectory since 1996. Liver disease, accidents, and other alcohol-linked causes dominate this landscape, each contributing uniquely to the overall toll. Understanding these breakdowns is crucial for targeted interventions and public health strategies.
Liver Disease: The Silent Killer
Chronic alcohol consumption remains the leading cause of liver disease, with cirrhosis being the most severe outcome. Since 1996, alcohol-related liver disease (ARLD) deaths have shown a steady rise in many countries, particularly among middle-aged adults (45–64 years). For instance, in the United States, ARLD deaths increased by over 50% between 1999 and 2017, with men accounting for nearly 70% of these fatalities. The progression from fatty liver to cirrhosis is insidious, often asymptomatic until irreversible damage occurs. Practical prevention includes limiting daily alcohol intake to 14 units per week for adults, as recommended by health authorities, and regular liver function tests for at-risk individuals.
Accidents: The Immediate Consequence
Alcohol-related accidents, including traffic fatalities, falls, and drownings, represent a more immediate and often preventable cause of death. Since 1996, global efforts to reduce drunk driving, such as stricter blood alcohol concentration (BAC) limits (e.g., 0.08% in many countries), have led to declines in alcohol-related road deaths. However, non-traffic accidents, particularly among younger adults (18–34 years), remain a persistent issue. For example, alcohol is implicated in over 40% of fatal falls in this age group. Public health campaigns emphasizing the risks of alcohol-impaired coordination and judgment, coupled with accessible public transportation options, can mitigate these risks.
Other Alcohol-Linked Causes: The Hidden Toll
Beyond liver disease and accidents, alcohol contributes to a spectrum of fatalities, including cardiovascular diseases, cancers, and suicides. Since 1996, alcohol-related cancers (e.g., liver, breast, and esophageal) have seen a notable increase, particularly in regions with rising alcohol consumption. For instance, alcohol is estimated to cause 4% of all cancer cases globally. Additionally, alcohol’s role in mental health crises is evident in its association with 20–30% of suicides in some studies. Addressing these causes requires a multifaceted approach, including education on the long-term health risks of alcohol, early mental health interventions, and policies to reduce alcohol availability and marketing.
Comparative Trends and Takeaways
While liver disease and accidents dominate alcohol-related deaths, the rise in other linked causes highlights the need for comprehensive strategies. Since 1996, the shift from acute (accidents) to chronic (liver disease, cancer) fatalities underscores the evolving nature of alcohol’s impact. Policymakers must balance immediate interventions, like stricter DUI laws, with long-term measures, such as taxation and advertising restrictions. For individuals, awareness of alcohol’s cumulative effects—from a single binge-drinking episode to decades of moderate consumption—is key to informed decision-making.
This breakdown of cause-specific deaths not only illuminates the scope of alcohol’s harm but also provides a roadmap for targeted action, ensuring that efforts are as diverse as the causes themselves.
How White Claw Gets Its Alcohol: The Fermentation Process Explained
You may want to see also
![]()
Policy Effects: Influence of alcohol regulations and public health initiatives on death rates
Alcohol-related deaths have shown a complex trajectory since 1996, influenced significantly by policy shifts and public health interventions. One striking example is the implementation of stricter drink-driving laws in many countries during the early 2000s. In the United States, the reduction of the legal blood alcohol concentration (BAC) limit from 0.10% to 0.08% in all states by 2004 coincided with a noticeable decline in alcohol-related traffic fatalities. According to the National Highway Traffic Safety Administration (NHTSA), these measures saved an estimated 30,000 lives between 1996 and 2018. This demonstrates how targeted regulations can directly impact mortality rates by altering behavior and reducing high-risk activities.
Public health initiatives focusing on education and prevention have also played a pivotal role. Campaigns like the U.K.’s “Drinkaware” and Australia’s “Alcohol. Think Again” have aimed to shift societal attitudes toward alcohol consumption, particularly among younger age groups. For instance, in Scotland, the introduction of minimum unit pricing (MUP) in 2018 led to a 13% reduction in alcohol-specific deaths within the first two years, as reported by Public Health Scotland. Such policies address affordability, a key driver of excessive drinking, and highlight the importance of economic measures in curbing harmful consumption patterns.
However, the effectiveness of these policies varies across demographics and regions. For example, while overall alcohol-related deaths have declined in some high-income countries, disparities persist among lower socioeconomic groups and Indigenous populations. In Canada, Indigenous communities continue to experience disproportionately higher rates of alcohol-attributable deaths, underscoring the need for culturally sensitive and targeted interventions. This suggests that while broad policies can yield positive outcomes, they must be complemented by localized strategies to address specific vulnerabilities.
A critical takeaway is the interplay between enforcement and education. Policies like taxation, licensing restrictions, and advertising bans can reduce availability and appeal, but their success relies on public awareness and compliance. For instance, France’s Evin Law, which restricts alcohol advertising, has been less effective in curbing youth drinking compared to countries with comprehensive school-based education programs. Combining regulatory measures with evidence-based education ensures a holistic approach, addressing both supply and demand factors in alcohol consumption.
Practical steps for policymakers include conducting regular reviews of alcohol control measures, leveraging data to identify at-risk populations, and fostering cross-sector collaboration. For individuals, understanding local regulations and participating in public health programs can amplify the impact of these initiatives. Ultimately, the decline in alcohol-related deaths since 1996 underscores the power of policy—when thoughtfully designed and rigorously implemented—to save lives and transform public health outcomes.
Signs of Alcohol Dementia: What to Watch For
You may want to see also
Frequently asked questions
While exact global figures are challenging to pinpoint due to varying reporting methods, the World Health Organization (WHO) estimates that alcohol contributes to approximately 3 million deaths annually worldwide. Since 1996, this would total over 90 million alcohol-related deaths.
According to the Centers for Disease Control and Prevention (CDC), alcohol-related deaths account for about 2.5% of all deaths in the U.S. annually. Since 1996, this translates to over 1 million alcohol-attributable deaths.
The number of alcohol-related deaths has generally increased globally since 1996, driven by factors like population growth, increased alcohol consumption in some regions, and rising rates of alcohol-related diseases such as liver cirrhosis and cancers.
Middle-aged adults (ages 45–64) have experienced the highest number of alcohol-related deaths since 1996, primarily due to chronic conditions like liver disease, cardiovascular issues, and alcohol-related accidents. However, younger age groups have also seen significant increases in alcohol-attributable deaths, particularly from acute causes like overdoses and injuries.