Alcohol aversion therapy is a treatment approach designed to reduce or eliminate alcohol consumption by creating a negative association with alcohol through psychological and sometimes pharmacological methods. This therapy typically involves pairing the ingestion of alcohol with an unpleasant stimulus, such as nausea induced by medications like disulfiram, or through conditioned response techniques where patients are trained to associate alcohol with negative experiences. The goal is to trigger an aversive reaction whenever the individual consumes alcohol, thereby discouraging future drinking. While it has shown effectiveness for some individuals, its success often depends on patient motivation, the severity of alcohol dependence, and the integration of complementary therapies like counseling or support groups.
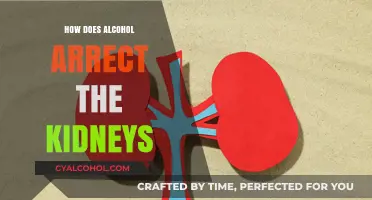
| Characteristics | Values |
|---|---|
| Mechanism | Pairs alcohol consumption with unpleasant stimuli to create aversion. |
| Stimuli Used | Nausea-inducing drugs (e.g., disulfiram), electric shocks, or bitter tastes. |
| Psychological Basis | Classical conditioning: associates alcohol with negative experiences. |
| Effectiveness | Moderate success rates; varies by individual and follow-up support. |
| Duration | Typically short-term therapy, often completed in a few sessions. |
| Side Effects | Nausea, anxiety, or temporary discomfort during treatment. |
| Long-Term Outcomes | Relapse possible without ongoing therapy or support. |
| Target Population | Individuals with severe alcohol dependence or those resistant to other treatments. |
| Combination Therapies | Often paired with counseling, cognitive-behavioral therapy, or support groups. |
| Controversies | Ethical concerns about coercion and potential psychological distress. |
| Latest Research (as of 2023) | Focus on personalized approaches and integrating technology for better outcomes. |
Explore related products





What You'll Learn
- Conditioned Taste Aversion: Pairing alcohol with nausea-inducing substances to create negative associations
- Behavioral Techniques: Using reinforcement and punishment to discourage alcohol consumption habits
- Psychological Mechanisms: Leveraging classical conditioning to alter drinking behavior through learned responses
- Medication-Assisted Therapy: Drugs like disulfiram induce aversive reactions when alcohol is consumed
- Long-Term Efficacy: Evaluating the sustainability of aversion therapy in reducing alcohol dependence
![]()
Conditioned Taste Aversion: Pairing alcohol with nausea-inducing substances to create negative associations
Alcohol aversion therapy leverages the brain's ability to form powerful associations between stimuli, a principle rooted in classical conditioning. Conditioned taste aversion (CTA) takes this a step further by deliberately pairing alcohol consumption with nausea-inducing substances, creating a negative association that discourages future drinking. This method is particularly effective because it taps into the body's natural survival mechanisms, where aversions to substances that cause discomfort are quickly learned and long-lasting. For instance, a single episode of nausea after consuming a specific food or drink can lead to a lasting avoidance of that item, even years later.
The process of CTA in alcohol aversion therapy typically involves administering a nausea-inducing medication, such as disulfiram, immediately after alcohol consumption. Disulfiram works by inhibiting the enzyme acetaldehyde dehydrogenase, causing acetaldehyde—a toxic byproduct of alcohol metabolism—to accumulate in the bloodstream. This buildup leads to unpleasant symptoms like nausea, vomiting, headaches, and rapid heartbeat. The key is timing: the medication must be taken within a specific window after drinking, usually within 10–15 minutes, to ensure the negative effects are directly linked to alcohol in the patient's mind. For example, a patient might consume a small, controlled amount of alcohol (e.g., 10–20 grams of ethanol) followed by 250–500 mg of disulfiram, depending on their tolerance and medical history.
While CTA is scientifically grounded, its success depends on several factors. First, the intensity and immediacy of the nausea are critical; mild discomfort may not create a strong enough aversion. Second, consistency is key—repeated pairings of alcohol with nausea reinforce the association. However, this approach is not without risks. Patients must be closely monitored to avoid severe reactions, especially in those with pre-existing health conditions. Additionally, CTA is most effective when combined with psychological interventions, such as cognitive-behavioral therapy, to address the underlying reasons for alcohol use.
A notable example of CTA in practice is the use of emetine, a nausea-inducing drug historically paired with alcohol in aversion therapy. Emetine’s potent effects made it highly effective but also led to its discontinuation due to safety concerns. Modern approaches prioritize safer alternatives like disulfiram, though even these require careful administration. For instance, therapists often start with lower doses of alcohol and medication, gradually increasing them as the patient’s tolerance and response are assessed. This stepwise approach minimizes risks while maximizing the therapeutic impact.
In conclusion, conditioned taste aversion is a targeted and potent tool in alcohol aversion therapy, but it demands precision and caution. By strategically pairing alcohol with nausea-inducing substances, therapists can create powerful negative associations that deter drinking. However, success hinges on careful dosing, timing, and patient monitoring, as well as integration with broader treatment strategies. For individuals struggling with alcohol dependence, CTA offers a unique and evidence-based pathway to recovery, though it is not a standalone solution. Practical tips include maintaining a consistent therapy schedule, communicating openly with healthcare providers, and being prepared for the physical and emotional challenges of the process.
Avoid Alcohol Post-Vaccination: Essential Tips for Optimal Recovery and Immunity
You may want to see also
Explore related products






![]()
Behavioral Techniques: Using reinforcement and punishment to discourage alcohol consumption habits
Alcohol aversion therapy leverages behavioral techniques rooted in operant conditioning to discourage drinking by pairing alcohol consumption with unpleasant consequences. Reinforcement and punishment are the twin pillars of this approach, reshaping habits through deliberate reward and deterrent systems. Positive reinforcement, for instance, involves rewarding abstinence—such as with praise, privileges, or tangible incentives—to encourage continued sobriety. Conversely, negative reinforcement removes aversive stimuli (e.g., reducing family tension) when drinking stops, reinforcing the behavior of abstaining. Punishment, on the other hand, introduces adverse outcomes directly linked to alcohol use, like nausea-inducing medications (e.g., disulfiram) or social sanctions, to deter future consumption.
Consider a structured program for a 35-year-old professional struggling with weekend binge drinking. Step one involves identifying a reinforcer—perhaps a $50 weekly reward for maintaining sobriety, deposited into a savings account. Step two introduces a punishment: consuming a single sip of alcohol triggers a mandatory 24-hour restriction from social activities. This dual approach creates a clear incentive-consequence dynamic, making abstinence more appealing than the temporary relief of drinking. For younger adults (ages 18–25), peer-based reinforcement, like group accountability challenges, often proves more effective than financial rewards, aligning with their social motivations.
However, caution is warranted. Overreliance on punishment can foster resentment or covert drinking behaviors, undermining long-term success. For example, pairing alcohol with emetic drugs (e.g., Antabuse) may work initially but risks creating a fear-based relationship with sobriety rather than intrinsic motivation. Similarly, excessive reinforcement (e.g., daily rewards) can lead to dependency on external incentives, failing to address the psychological roots of addiction. Balancing the two—such as gradually tapering rewards while introducing self-reflection exercises—ensures sustainability.
A comparative analysis highlights the efficacy of these techniques across demographics. Studies show older adults (50+) respond better to health-focused reinforcement (e.g., tracking improved liver function) than punitive measures, whereas adolescents benefit from immediate, tangible rewards paired with mild punishments (e.g., losing screen time for slip-ups). Cultural factors also play a role: collectivist societies may prioritize family-based reinforcement, while individualistic cultures lean toward personal achievement incentives.
In practice, specificity is key. For instance, a 45-year-old with a 10-year drinking history might pair a daily sobriety journal (reinforcement) with a pre-committed donation to a cause they dislike (punishment) for every drink consumed. Apps like *Sober Grid* can gamify reinforcement by awarding virtual badges for milestones, while wearable devices like BACtrack monitor compliance for punishment protocols. Takeaway: Behavioral techniques are most potent when tailored to individual triggers, preferences, and life stages, combining reinforcement and punishment in a way that fosters autonomy, not coercion.
Effective Ways to Flush Alcohol from Your System Safely and Quickly
You may want to see also
Explore related products






![]()
Psychological Mechanisms: Leveraging classical conditioning to alter drinking behavior through learned responses
Alcohol aversion therapy operates on the principle of classical conditioning, a psychological mechanism rooted in Pavlov’s experiments with dogs. By pairing alcohol consumption with an unpleasant stimulus, such as nausea induced by a medication like disulfiram, the therapy aims to create a conditioned negative response to alcohol. Over time, the brain associates drinking with discomfort, reducing the desire to consume alcohol. This method leverages the brain’s natural ability to form associations, turning a previously neutral stimulus (alcohol) into one that triggers aversion.
Consider the process step-by-step: first, a patient ingests a controlled dose of alcohol (typically 1–2 ounces of ethanol) under medical supervision. Within minutes, they are administered disulfiram (250–500 mg), which inhibits acetaldehyde dehydrogenase, causing acetaldehyde buildup and resulting in symptoms like nausea, flushing, and palpitations. This pairing occurs repeatedly, though sparingly, to avoid habituation. The key is consistency—each exposure reinforces the negative association, gradually altering the individual’s behavioral response to alcohol cues.
Critically, this approach differs from mere punishment. While punishment might temporarily suppress behavior, classical conditioning alters the underlying psychological response. For instance, a 35-year-old patient with a history of binge drinking might initially view alcohol as a reward. After aversion therapy, the sight of a beer bottle could evoke anticipatory nausea, shifting their perception from desire to avoidance. This shift is not just behavioral but neurological, as the amygdala and hippocampus rewire associations between alcohol and negative outcomes.
However, aversion therapy is not without limitations. Its effectiveness varies by individual, with success rates ranging from 30% to 70% depending on factors like motivation, dosage precision, and adherence to treatment protocols. For instance, younger adults (ages 18–25) may respond differently than older individuals due to differences in brain plasticity and drinking patterns. Additionally, the therapy requires strict medical oversight to prevent adverse reactions, such as severe hypotension or respiratory distress from disulfiram-ethanol interactions.
To maximize efficacy, practitioners should combine aversion therapy with cognitive-behavioral techniques. For example, patients can practice visualizing alcohol-related cues (e.g., a bar scene) while recalling the discomfort experienced during therapy sessions. This mental rehearsal strengthens the conditioned response, making it more robust in real-world scenarios. Practical tips include maintaining a journal to track triggers and responses, avoiding environments associated with drinking, and engaging in alternative reward systems, like exercise or hobbies, to replace alcohol’s role in stress relief.
In conclusion, alcohol aversion therapy exemplifies how classical conditioning can be harnessed to modify deeply ingrained behaviors. By systematically pairing alcohol with negative stimuli, it reshapes the brain’s response to drinking cues, offering a powerful tool for those struggling with alcohol dependence. While not a one-size-fits-all solution, its psychological foundation and structured approach make it a valuable component of comprehensive addiction treatment.
Which Government Agency Sets Alcohol Taxes in the U.S.?
You may want to see also
Explore related products






![]()
Medication-Assisted Therapy: Drugs like disulfiram induce aversive reactions when alcohol is consumed
Alcohol aversion therapy leverages the body's natural response to unpleasant stimuli, but medication-assisted therapy takes this a step further by chemically engineering those reactions. Disulfiram, a cornerstone of this approach, disrupts the body's ability to metabolize alcohol. Normally, alcohol is broken down into acetaldehyde, a toxic substance quickly cleared by the liver. Disulfiram blocks this process, allowing acetaldehyde to accumulate. This buildup triggers a cascade of intensely unpleasant symptoms, including nausea, vomiting, headache, flushing, and palpitations, within 10-30 minutes of alcohol consumption. The severity of these reactions acts as a powerful deterrent, conditioning the individual to associate drinking with immediate and severe discomfort.
For optimal effectiveness, disulfiram is typically prescribed at a daily dose of 250 mg, taken orally under supervision to ensure compliance. It's crucial to note that disulfiram itself is not addictive and does not directly reduce cravings. Its power lies in creating a strong negative reinforcement loop, where the fear of experiencing the aversive reaction becomes a powerful motivator for abstinence. This method is particularly suited for individuals with a history of chronic relapse who require a strong external deterrent to support their recovery efforts.
While disulfiram's effectiveness is well-documented, its use requires careful consideration. The drug is contraindicated in individuals with cardiovascular disease, severe psychiatric disorders, or those who are pregnant or breastfeeding. Additionally, patients must be fully committed to abstinence, as even small amounts of alcohol can trigger the aversive reaction. This includes avoiding hidden sources of alcohol, such as certain medications, mouthwashes, and even some food products. Regular monitoring by a healthcare professional is essential to ensure safety and adjust the treatment plan as needed.
The success of disulfiram-based aversion therapy hinges on a comprehensive approach. It should be integrated into a broader treatment plan that includes counseling, behavioral therapy, and social support. This multi-pronged strategy addresses the psychological and social factors contributing to alcohol dependence, while disulfiram provides a powerful physical deterrent. By combining these elements, medication-assisted aversion therapy offers a robust tool for individuals seeking to break free from the cycle of addiction and rebuild their lives.
Alcohol's Impact: Does Drinking Damage Brain Nerve Cells?
You may want to see also
Explore related products

![]()
Long-Term Efficacy: Evaluating the sustainability of aversion therapy in reducing alcohol dependence
Alcohol aversion therapy, a treatment designed to create a negative association with alcohol consumption, has shown promise in reducing alcohol dependence. However, its long-term efficacy remains a critical area of evaluation. This therapy typically involves pairing alcohol intake with an aversive stimulus, such as nausea induced by medications like disulfiram or emetine. While initial studies report success rates ranging from 30% to 70% in reducing drinking behavior, the sustainability of these outcomes is less clear. Understanding the factors that influence long-term success is essential for clinicians and patients alike.
One key challenge in assessing long-term efficacy is the variability in treatment protocols. Dosage, frequency, and duration of aversion therapy can differ significantly across studies. For instance, disulfiram is often prescribed at doses of 250–500 mg/day, but adherence to this regimen declines over time, particularly beyond the first six months. Similarly, emetine, administered in controlled settings, may produce immediate aversion but lacks standardized follow-up protocols to reinforce the learned response. Without consistent guidelines, it becomes difficult to compare outcomes and identify best practices for sustained recovery.
Another critical factor is the psychological readiness of the individual undergoing therapy. Aversion therapy is most effective when combined with cognitive-behavioral interventions that address underlying triggers for alcohol use. Patients who receive concurrent counseling or participate in support groups, such as Alcoholics Anonymous, tend to exhibit higher long-term abstinence rates. For example, a study published in the *Journal of Substance Abuse Treatment* found that individuals who combined aversion therapy with psychotherapy maintained sobriety for an average of 18 months, compared to 6 months for those receiving aversion therapy alone. This highlights the importance of a holistic approach to treatment.
Practical considerations also play a role in the sustainability of aversion therapy. Side effects of medications, such as liver toxicity associated with disulfiram, can deter long-term use. Additionally, the cost and accessibility of treatment may limit its adoption, particularly in underserved populations. To enhance long-term efficacy, clinicians should tailor treatment plans to individual needs, monitor progress regularly, and provide ongoing support. For instance, mobile health apps that track drinking behavior and offer real-time feedback could serve as a low-cost adjunct to traditional therapy.
In conclusion, while alcohol aversion therapy holds potential for reducing alcohol dependence, its long-term efficacy depends on standardized protocols, psychological readiness, and practical implementation strategies. By addressing these factors, clinicians can improve the sustainability of treatment outcomes and offer a more effective solution for individuals struggling with alcohol addiction. Future research should focus on developing evidence-based guidelines and exploring innovative tools to support long-term recovery.
Surviving with an Alcoholic: Strategies for Copping and Healing
You may want to see also
Frequently asked questions
Alcohol aversion therapy is a behavioral treatment that aims to reduce or eliminate alcohol consumption by creating a negative association with alcohol. It typically involves pairing alcohol with an unpleasant stimulus, such as nausea-inducing medication, to condition the individual to avoid alcohol.
Common methods include pairing alcohol with medications like disulfiram or emetine, which cause nausea, vomiting, or other aversive reactions when alcohol is consumed. Another approach is covert sensitization, where individuals imagine unpleasant consequences of drinking during therapy sessions.
Effectiveness varies; some individuals respond well, while others may not experience lasting changes. Success often depends on the person's motivation, the severity of their alcohol use disorder, and the specific method used. It is generally more effective when combined with other treatments like counseling.
Yes, potential risks include physical side effects from medications (e.g., nausea, headaches) and psychological distress from the aversive conditioning. It is important for the therapy to be administered by a trained professional to minimize risks and ensure safety.
Results can vary, but some individuals may experience changes in behavior shortly after treatment begins. Long-term success often requires ongoing support and additional therapies to address underlying issues related to alcohol use.