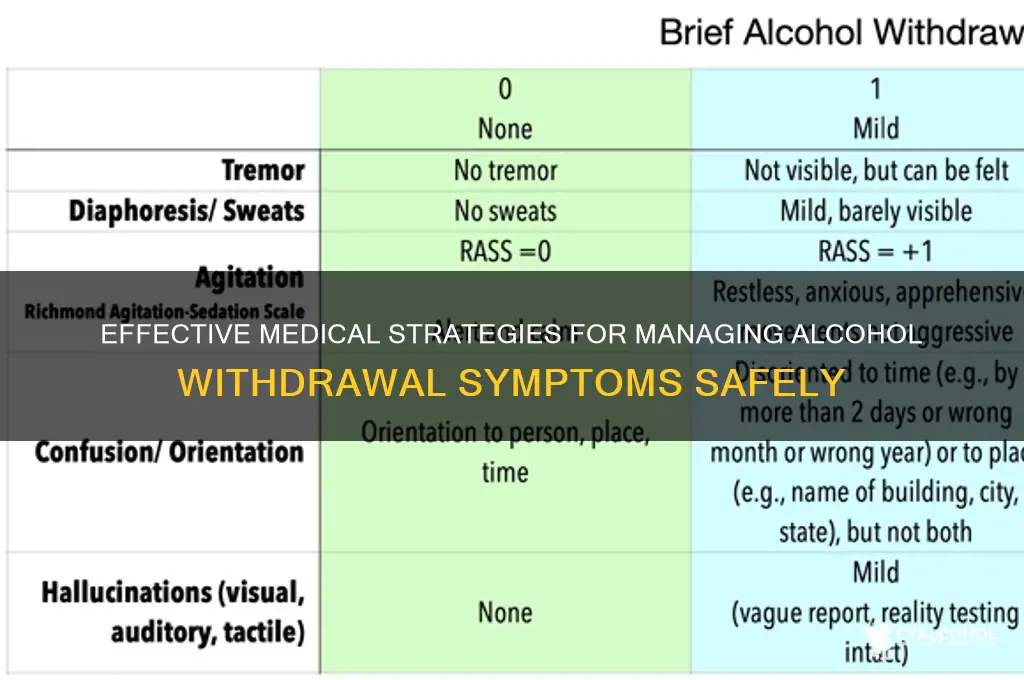
Treating alcohol withdrawal requires a carefully managed approach to ensure safety and minimize complications, as the process can range from mild to life-threatening. Doctors typically begin by assessing the severity of withdrawal symptoms using tools like the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) scale, which evaluates symptoms such as anxiety, tremors, and nausea. Mild to moderate cases may be managed with outpatient care, involving medications like benzodiazepines (e.g., diazepam or lorazepam) to alleviate anxiety and prevent seizures, along with supportive care such as hydration and nutritional support. Severe cases, particularly those at risk of delirium tremens (DTs), often require hospitalization for close monitoring and intravenous medications. Additionally, doctors may prescribe anticonvulsants, antipsychotics, or beta-blockers to address specific symptoms, while also addressing underlying nutritional deficiencies, such as thiamine supplementation to prevent Wernicke-Korsakoff syndrome. Throughout treatment, psychological support and counseling are integrated to encourage long-term sobriety and prevent relapse.
| Characteristics | Values |
|---|---|
| Assessment and Monitoring | Thorough medical history, physical exam, and lab tests (e.g., blood alcohol level, electrolytes, liver function). Use of tools like CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol) to gauge severity. |
| Setting of Treatment | Outpatient for mild withdrawal; inpatient or intensive care for moderate to severe cases, especially with complications like seizures or delirium tremens (DTs). |
| Medications | Benzodiazepines (e.g., diazepam, lorazepam) are first-line for symptom management. Anticonvulsants (e.g., carbamazepine) and beta-blockers (e.g., propranolol) may be used in specific cases. |
| Fluid and Electrolyte Management | Intravenous fluids and electrolytes (e.g., magnesium, potassium) to correct dehydration and imbalances caused by prolonged alcohol use. |
| Nutritional Support | Thiamine (vitamin B1) supplementation to prevent Wernicke-Korsakoff syndrome, a common complication of chronic alcohol use. Multivitamins and balanced nutrition are also provided. |
| Psychosocial Support | Counseling, therapy (e.g., cognitive-behavioral therapy), and support groups (e.g., Alcoholics Anonymous) to address underlying addiction and prevent relapse. |
| Management of Complications | Specific treatments for seizures (e.g., benzodiazepines), delirium tremens (high-dose benzodiazepines, antipsychotics), and other complications like infections or gastrointestinal bleeding. |
| Long-Term Treatment | Medications like disulfiram, naltrexone, or acamprosate to support sobriety. Ongoing therapy and support systems to maintain abstinence. |
| Patient Education | Education on the risks of alcohol withdrawal, the importance of abstinence, and strategies to cope with cravings and triggers. |
| Follow-Up Care | Regular follow-up appointments to monitor progress, adjust treatment, and provide ongoing support for recovery. |
Explore related products






What You'll Learn
- Medications for Symptoms: Benzodiazepines, antipsychotics, and anticonvulsants manage anxiety, seizures, and hallucinations during withdrawal
- Detoxification Protocols: Medically supervised detox ensures safety, monitors vitals, and prevents complications like delirium tremens
- Hydration and Nutrition: IV fluids, vitamins (thiamine), and balanced meals address dehydration and malnutrition
- Psychological Support: Counseling, therapy, and support groups aid emotional recovery and relapse prevention
- Aftercare Planning: Outpatient programs, sober living, and follow-ups sustain long-term sobriety and health
![]()
Medications for Symptoms: Benzodiazepines, antipsychotics, and anticonvulsants manage anxiety, seizures, and hallucinations during withdrawal
Alcohol withdrawal is a complex and potentially life-threatening condition that demands precise medical intervention. Among the arsenal of treatments, medications play a pivotal role in managing the most severe symptoms: anxiety, seizures, and hallucinations. Benzodiazepines, antipsychotics, and anticonvulsants are the cornerstone drugs in this approach, each targeting specific manifestations of withdrawal with tailored efficacy.
Benzodiazepines, such as diazepam (Valium) or lorazepam (Ativan), are the first-line treatment for alcohol withdrawal due to their potent anxiolytic and anticonvulsant properties. These medications act on the GABA receptors in the brain, calming overactivity caused by alcohol cessation. Dosage is critical and often individualized; for instance, diazepam may be administered in 10 mg doses every 6–8 hours, titrated downward as symptoms subside. Prolonged-release formulations can reduce the risk of rebound withdrawal, a common concern with shorter-acting benzodiazepines. However, their use requires caution in patients with a history of substance abuse or respiratory compromise, as they carry a risk of dependence and sedation.
Antipsychotics, like haloperidol or quetiapine, are reserved for managing severe agitation or hallucinations that benzodiazepines alone cannot control. These drugs modulate dopamine receptors, stabilizing psychotic symptoms during withdrawal. For example, haloperidol can be given in 2.5–5 mg doses every 4–6 hours, but its use is limited by potential side effects such as extrapyramidal symptoms (EPS). Quetiapine, a newer atypical antipsychotic, offers a more favorable side effect profile and may be preferred in patients with comorbid conditions. Antipsychotics are not a standalone treatment but rather an adjunct to benzodiazepines, addressing specific symptoms while minimizing risks.
Anticonvulsants, such as carbamazepine or gabapentin, provide an alternative for patients who cannot tolerate benzodiazepines or require additional seizure prophylaxis. These medications stabilize neuronal membranes, reducing the likelihood of seizures during withdrawal. Carbamazepine, for instance, is dosed at 200 mg twice daily, gradually increased to 400 mg twice daily as tolerated. Gabapentin, with its milder side effect profile, can be initiated at 300 mg three times daily and titrated up to 1200 mg three times daily. While anticonvulsants lack the broad-spectrum efficacy of benzodiazepines, they offer a valuable option for patients with specific contraindications or preferences.
In practice, the choice of medication depends on the patient’s symptom severity, medical history, and risk factors. For instance, older adults or those with hepatic impairment may require lower doses or alternative agents to avoid toxicity. Continuous monitoring is essential, as withdrawal symptoms can escalate rapidly. Combining these medications with supportive care, such as hydration and nutritional support, enhances their effectiveness. Ultimately, the goal is not just symptom management but a safe transition to long-term recovery, often involving counseling and behavioral therapies.
Do Ripe Bananas Naturally Contain Alcohol? Surprising Facts Revealed
You may want to see also
Explore related products






![]()
Detoxification Protocols: Medically supervised detox ensures safety, monitors vitals, and prevents complications like delirium tremens
Alcohol withdrawal is a perilous process that demands professional oversight. Medically supervised detoxification protocols are the cornerstone of safe and effective treatment, mitigating risks and ensuring patient stability. These protocols typically involve a structured approach to tapering alcohol consumption under close medical supervision, often in an inpatient setting. The primary goal is to manage withdrawal symptoms, which can range from mild anxiety and tremors to severe complications like seizures and delirium tremens (DTs). Without medical intervention, the unpredictability of withdrawal can lead to life-threatening outcomes, making supervised detox not just beneficial but essential for high-risk individuals.
The detoxification process begins with a comprehensive assessment to determine the severity of dependence and potential withdrawal risks. This includes evaluating the patient’s medical history, alcohol consumption patterns, and physical condition. Based on this assessment, doctors may prescribe medications such as benzodiazepines (e.g., diazepam or lorazepam) to alleviate symptoms and prevent complications. Dosages are carefully titrated, starting with higher amounts during the acute phase and gradually tapering off to minimize dependence on the medication itself. For instance, a typical regimen might involve 10–20 mg of diazepam every 6–8 hours, adjusted based on symptom severity and patient response.
Monitoring vitals is a critical component of medically supervised detox. Continuous observation of heart rate, blood pressure, temperature, and respiratory rate helps detect early signs of complications like DTs, which can manifest within 48–96 hours after the last drink. Nurses and physicians use standardized tools like the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) to quantify withdrawal severity and guide treatment adjustments. This proactive approach allows for immediate intervention, such as administering additional medication or intravenous fluids, to stabilize the patient and prevent escalation.
Beyond medication and monitoring, supportive care plays a vital role in detoxification protocols. Patients receive hydration and nutritional support, as chronic alcohol use often leads to deficiencies in essential vitamins like thiamine, which can exacerbate neurological complications. Psychological support is equally important, as withdrawal can induce anxiety, depression, and insomnia. Counseling and therapy sessions help patients cope with emotional distress and prepare for long-term recovery. Practical tips, such as maintaining a structured daily routine and avoiding triggers, are also provided to enhance resilience during and after detox.
In conclusion, medically supervised detoxification protocols are a systematic, evidence-based approach to managing alcohol withdrawal safely. By combining medication, vital sign monitoring, and supportive care, these protocols minimize the risk of severe complications like delirium tremens while addressing the physical and psychological challenges of withdrawal. For individuals struggling with alcohol dependence, this structured and compassionate care is not just a treatment—it’s a lifeline to recovery.
Why Do People Become Alcoholics?
You may want to see also
Explore related products






![]()
Hydration and Nutrition: IV fluids, vitamins (thiamine), and balanced meals address dehydration and malnutrition
Chronic alcohol use wreaks havoc on the body's fluid balance and nutrient stores. Dehydration, electrolyte imbalances, and malnutrition are common in those withdrawing from alcohol, exacerbating symptoms like tremors, confusion, and organ dysfunction. Addressing these deficiencies is a cornerstone of medical management during alcohol withdrawal.
Intravenous (IV) fluids are often the first line of defense. Normal saline (0.9% sodium chloride) is typically administered to rapidly replenish fluids and electrolytes lost through vomiting, diarrhea, and increased urination, common during withdrawal. The rate of IV fluid administration is carefully monitored by medical professionals, taking into account the patient's individual needs and the severity of dehydration.
Thiamine (vitamin B1) deficiency is a particularly dangerous consequence of chronic alcohol use, leading to Wernicke-Korsakoff syndrome, a neurological disorder characterized by confusion, memory loss, and coordination problems. High-dose thiamine supplementation, often administered intravenously, is crucial during withdrawal to prevent and treat this potentially irreversible condition. The recommended dose is typically 100-200 mg intravenously daily for several days, followed by oral supplementation.
Balanced meals, though seemingly simple, are equally vital. Alcohol often displaces nutritious food in the diet, leading to deficiencies in vitamins, minerals, and essential amino acids. A diet rich in fruits, vegetables, whole grains, and lean protein helps restore these deficiencies and supports the body's healing process. Small, frequent meals are often better tolerated during the acute withdrawal phase, gradually increasing in size as the patient's appetite improves.
This multi-pronged approach to hydration and nutrition – IV fluids, thiamine supplementation, and balanced meals – forms a crucial foundation for managing alcohol withdrawal. By addressing these fundamental needs, healthcare providers can significantly improve patient comfort, prevent complications, and pave the way for a successful recovery.
Safe Boating and Alcohol: Understanding Legal Limits and Risks
You may want to see also
Explore related products






![]()
Psychological Support: Counseling, therapy, and support groups aid emotional recovery and relapse prevention
Alcohol withdrawal isn't just a physical battle; it's a psychological war. The emotional turmoil—anxiety, depression, guilt—can be as debilitating as the shakes and sweats. This is where counseling, therapy, and support groups step in, not as luxuries, but as essential tools for rebuilding a life shattered by addiction.
Imagine a person, newly sober, grappling with the void alcohol once filled. Counseling provides a safe space to explore the root causes of their drinking, unraveling the tangled web of emotions and triggers. Cognitive Behavioral Therapy (CBT), for instance, equips them with concrete strategies to challenge negative thought patterns and develop healthier coping mechanisms. It's like learning a new language, one that replaces self-destruction with self-compassion.
Therapy isn't a quick fix; it's a journey. Group therapy, in particular, offers a unique power: the power of shared experience. Sitting in a room with others who understand the struggle fosters a sense of belonging, shattering the isolating grip of addiction. Hearing others' stories, their triumphs and setbacks, provides invaluable perspective and hope. It's a reminder that recovery isn't linear, that relapses are detours, not dead ends.
Support groups, like Alcoholics Anonymous, provide a lifeline beyond the therapist's office. They offer a community, a network of understanding individuals who become a surrogate family. The 12-step program, while not for everyone, provides a structured framework for personal growth and accountability. Regular meetings become anchors, grounding individuals in their commitment to sobriety and reminding them they are not alone.
Think of psychological support as the scaffolding that holds a person upright as they rebuild their life. It's not about erasing the past, but about learning to live with it, to forge a new identity free from the chains of addiction. It's about finding the strength to face the darkness and emerge, not unscathed, but transformed.
Alcohol's Impact: How Drinking Disrupts Your Sleep Cycle
You may want to see also
Explore related products





![]()
Aftercare Planning: Outpatient programs, sober living, and follow-ups sustain long-term sobriety and health
Detox is just the beginning. Without robust aftercare, relapse rates for alcohol use disorder soar to 70-90% within a year. Outpatient programs, sober living environments, and structured follow-ups form a critical safety net, addressing the psychological, social, and behavioral roots of addiction that detox alone cannot.
Outpatient Programs: Structured Support Without Hospital Walls
Outpatient programs offer flexibility for those transitioning from inpatient detox or seeking early intervention. Intensive Outpatient Programs (IOPs) typically meet 3-5 days weekly for 3-4 hours, blending group therapy, individual counseling, and education on relapse prevention. Partial Hospitalization Programs (PHPs) provide a higher level of care, often 5-7 days a week for 6 hours, ideal for individuals with co-occurring mental health disorders. Both formats incorporate evidence-based therapies like Cognitive Behavioral Therapy (CBT) and Motivational Interviewing (MI), with medication management for cravings (e.g., naltrexone 50 mg daily or acamprosate 666 mg three times daily). Key to success is consistent attendance, which studies show reduces relapse by up to 50% in the first year.
Sober Living Homes: Bridging the Gap Between Treatment and Independence
Sober living homes (SLHs) provide a drug- and alcohol-free environment for individuals exiting detox or inpatient rehab. Residents adhere to strict rules: mandatory drug testing, curfews, and participation in 12-step meetings or outpatient therapy. Unlike rehab centers, SLHs are peer-driven, fostering accountability through shared experiences. Research indicates residents who stay in SLHs for at least 90 days demonstrate higher abstinence rates and improved social functioning. For instance, a study in the *Journal of Psychoactive Drugs* found that 69% of SLH residents remained abstinent after 6 months, compared to 24% of those without such housing. Practical tip: Look for SLHs certified by state associations, as these adhere to higher standards of care.
Follow-Up Care: The Lifeline for Long-Term Sobriety
Follow-up care is the backbone of sustained recovery, yet it’s often overlooked. Regular check-ins with addiction specialists, primary care physicians, or therapists help monitor progress, adjust medications, and address emerging triggers. Telehealth platforms have expanded access, allowing remote sessions for those in rural areas or with transportation barriers. A critical component is contingency management, where rewards (e.g., gift cards) incentivize negative drug tests. Studies show this approach increases treatment retention by 30%. Equally vital are family therapy sessions, which rebuild trust and educate loved ones on supporting recovery. For maximum effectiveness, follow-ups should occur weekly for the first month, biweekly for months 2-3, and monthly thereafter, tailored to individual risk factors.
Integrating the Three Pillars for Holistic Recovery
Combining outpatient programs, sober living, and follow-ups creates a multi-layered defense against relapse. For example, a 35-year-old professional might attend IOP sessions after work, reside in an SLH to avoid triggers at home, and meet biweekly with a therapist to process emotional challenges. This integrated approach addresses the biological (medication), psychological (therapy), and social (community) dimensions of addiction. Caution: Avoid overloading schedules, as burnout can derail progress. Instead, prioritize consistency and self-compassion. The goal isn’t perfection but resilience—building a life where sobriety is not just possible but sustainable.
Alcohol and Gout: Understanding the Link to Flare-Ups
You may want to see also
Frequently asked questions
Doctors first assess the severity of withdrawal symptoms using tools like the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar). They stabilize the patient, manage dehydration and electrolyte imbalances, and administer medications to prevent complications.
Benzodiazepines (e.g., diazepam, lorazepam) are the primary medications used to manage withdrawal symptoms. Other medications like anticonvulsants (e.g., carbamazepine) or beta-blockers may be used in specific cases to address symptoms like seizures or anxiety.
The acute phase of withdrawal treatment usually lasts 5–7 days, but the duration can vary based on the severity of symptoms and individual factors. Long-term treatment may include therapy and medications to support sobriety.
Mild to moderate withdrawal may be managed at home under medical supervision, but severe cases (e.g., delirium tremens) require hospitalization to prevent life-threatening complications like seizures or dehydration.
Therapy, such as cognitive-behavioral therapy (CBT) or counseling, is crucial for addressing the underlying causes of alcohol use and preventing relapse. It is often integrated into long-term treatment plans after the acute withdrawal phase.