Fetal Alcohol Syndrome (FAS) is a condition that occurs when a baby is exposed to alcohol during pregnancy, leading to a range of physical, behavioral, and cognitive impairments. One of the most recognizable aspects of FAS is the distinct facial features that affected babies often exhibit, including a smooth ridge between the nose and upper lip (philtrum), a thin upper lip, small eyes, and a smaller-than-average head size. These characteristics are a result of the developmental disruptions caused by alcohol exposure in utero. Beyond physical appearance, babies with FAS may also face challenges such as growth deficiencies, learning disabilities, and difficulties with attention and coordination, making early diagnosis and intervention crucial for their long-term well-being.
Explore related products






What You'll Learn
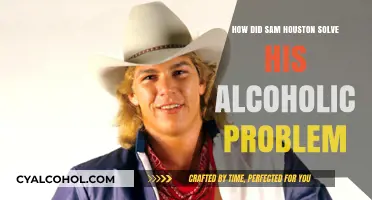
- Facial Features: Smooth philtrum, thin upper lip, small eyes, and flattened cheekbones are common indicators
- Growth Deficiencies: Below-average height, weight, and head circumference due to prenatal alcohol exposure
- Brain Development: Cognitive delays, learning disabilities, and poor memory linked to alcohol damage
- Behavioral Issues: Hyperactivity, attention deficits, and difficulties with social interactions often observed
- Physical Abnormalities: Joint and limb deformities, heart defects, and kidney problems may occur
![]()
Facial Features: Smooth philtrum, thin upper lip, small eyes, and flattened cheekbones are common indicators
Fetal Alcohol Syndrome (FAS) is a condition that can cause distinct facial abnormalities in affected babies, providing visual cues that are crucial for early identification. One of the most recognizable features is a smooth philtrum, the groove between the nose and upper lip. In typically developing infants, this area is well-defined with a series of vertical ridges. However, in babies with FAS, the philtrum appears flattened and less pronounced, almost blending seamlessly into the surrounding skin. This subtle yet significant difference is a key indicator for healthcare professionals during initial assessments.
Another characteristic facial feature is a thin upper lip, which often accompanies the smooth philtrum. Normally, a baby’s upper lip is fuller and more pronounced. In contrast, infants with FAS exhibit an upper lip that appears thinner and less voluminous, contributing to an overall altered facial expression. This combination of a smooth philtrum and thin upper lip creates a unique facial profile that is often described as "flat" or "smooth" in the middle region of the face.
Small eyes are another common indicator of FAS. Affected babies may have eyes that appear unusually narrow or widely spaced, with a reduced palpebral fissure length (the opening between the eyelids). This feature is often subtle but can be measured and compared to standardized norms for age-appropriate eye size. The small eye appearance, combined with the other facial anomalies, further distinguishes the facial phenotype of FAS.
Flattened cheekbones are yet another hallmark of this syndrome. Typically, babies have rounded, prominent cheekbones that contribute to the fullness of their faces. In infants with FAS, the cheekbones are often underdeveloped, resulting in a flatter appearance in the midface region. This flattening can make the face seem less contoured and more compressed from the side profile. Together, these facial features—smooth philtrum, thin upper lip, small eyes, and flattened cheekbones—create a distinct facial gestalt that is highly suggestive of prenatal alcohol exposure.
Early recognition of these facial features is critical for timely intervention and support. Healthcare providers, particularly pediatricians and neonatologists, should be trained to identify these subtle yet consistent indicators during routine examinations. Parents and caregivers can also play a role by being aware of these signs and seeking medical advice if they notice any abnormalities. While these facial features are not the only indicators of FAS, they are among the most visible and diagnostically valuable, serving as a starting point for further evaluation and comprehensive care.
Post-Sex Alcohol Wipes: Effective Hygiene or Unnecessary Practice?
You may want to see also
Explore related products






![]()
Growth Deficiencies: Below-average height, weight, and head circumference due to prenatal alcohol exposure
Prenatal alcohol exposure can lead to significant growth deficiencies in babies, manifesting as below-average height, weight, and head circumference. These physical characteristics are often among the first observable signs of Fetal Alcohol Syndrome (FAS) and are critical for early diagnosis. When a pregnant individual consumes alcohol, it interferes with the fetus’s ability to absorb essential nutrients and oxygen, stunting overall growth and development. As a result, affected infants are often noticeably smaller than their peers at birth, a condition known as intrauterine growth restriction (IUGR). This deficiency in size is not just a temporary issue but can persist throughout childhood and into adulthood, with individuals often remaining shorter and lighter than average.
Below-average height is a hallmark of FAS, with affected children frequently falling below the third percentile for height relative to their age group. This stunted growth is directly linked to the toxic effects of alcohol on developing cells and tissues, particularly those responsible for bone and muscle development. Over time, this height deficiency becomes more apparent as the child grows, often leading to disproportionate body features. Parents and caregivers may notice that the child’s limbs or torso appear shorter than expected, further emphasizing the impact of prenatal alcohol exposure on physical growth.
Weight deficiencies in babies with FAS are equally concerning, as these infants often struggle to gain weight at a normal rate. Alcohol disrupts the placenta’s function, reducing the transfer of nutrients and calories to the fetus, which results in poor weight gain both before and after birth. Low birth weight is common, and these babies may continue to lag in weight milestones during infancy and childhood. This underweight condition is not merely a cosmetic issue; it can lead to weakened immunity, developmental delays, and increased susceptibility to illnesses, compounding the challenges faced by these children.
Head circumference is another critical area affected by prenatal alcohol exposure, with many babies born with microcephaly—a condition characterized by an abnormally small head size. The brain’s growth is particularly sensitive to alcohol’s teratogenic effects, leading to reduced brain volume and impaired cognitive development. A smaller head circumference is often one of the most visible indicators of FAS and can be measured during routine pediatric check-ups. This measurement is a key diagnostic criterion, as it directly correlates with the severity of alcohol-related brain damage and subsequent developmental challenges.
The combination of below-average height, weight, and head circumference creates a distinct physical profile in babies with FAS. These growth deficiencies are not isolated issues but are interconnected, reflecting the systemic harm caused by prenatal alcohol exposure. Early identification of these signs is crucial, as it allows for timely intervention and support to address the child’s medical, developmental, and educational needs. Healthcare providers play a vital role in monitoring growth patterns and educating families about the long-term implications of FAS, emphasizing the importance of prevention through abstaining from alcohol during pregnancy.
Setting Up a Tasting Station: Alcoholic Beverages
You may want to see also
Explore related products






![]()
Brain Development: Cognitive delays, learning disabilities, and poor memory linked to alcohol damage
Fetal Alcohol Syndrome (FAS) is a condition that occurs when a mother consumes alcohol during pregnancy, leading to a range of physical, behavioral, and cognitive impairments in the developing fetus. One of the most profound and lasting effects of prenatal alcohol exposure is on brain development, which manifests as cognitive delays, learning disabilities, and poor memory. Alcohol is a teratogen, meaning it interferes with the normal development of the fetal brain, particularly during critical periods of neuronal growth and connectivity. The damage is often irreversible, making early intervention and support crucial for affected individuals.
Cognitive delays are a hallmark of FAS, with children often exhibiting significant challenges in areas such as problem-solving, reasoning, and abstract thinking. The prefrontal cortex, responsible for executive functions like planning and decision-making, is particularly vulnerable to alcohol-induced damage. As a result, children with FAS may struggle with tasks that require multi-step thinking or understanding cause-and-effect relationships. These delays are not always immediately apparent in infancy but become more evident as the child grows and faces increasingly complex cognitive demands. Early developmental milestones, such as rolling over, sitting up, and walking, may also be delayed due to the overall impact of alcohol on the central nervous system.
Learning disabilities are another common consequence of prenatal alcohol exposure. Affected children often face difficulties in acquiring and retaining academic skills, particularly in reading, mathematics, and language. The hippocampus, a brain region critical for memory and learning, is often damaged by alcohol, leading to challenges in encoding and retrieving information. For example, a child with FAS may struggle to remember sight words, follow multi-step instructions, or understand abstract concepts like time or money. These learning disabilities are not due to a lack of intelligence but rather to the structural and functional abnormalities in the brain caused by alcohol.
Poor memory is closely linked to the hippocampal damage seen in FAS. Children with this condition often have trouble with both short-term and long-term memory. They may forget instructions given just moments ago or struggle to recall events from their past. This memory impairment can significantly impact their ability to learn from experiences, follow routines, or build meaningful relationships. For instance, a child might repeatedly make the same mistakes because they cannot remember the consequences of their actions. Memory deficits also contribute to difficulties in social interactions, as the child may struggle to remember names, faces, or social norms.
The cognitive and learning challenges associated with FAS are often compounded by other neurodevelopmental issues, such as attention deficits and impulsivity. These co-occurring difficulties can make it harder for children to succeed in school and social settings, even with supportive interventions. It is essential for caregivers, educators, and healthcare providers to understand the specific cognitive profile of each child with FAS to tailor interventions effectively. Strategies such as structured routines, visual aids, and repetitive practice can help mitigate some of the learning challenges, but the underlying brain damage remains a lifelong barrier.
In summary, the impact of prenatal alcohol exposure on brain development is profound and far-reaching, leading to cognitive delays, learning disabilities, and poor memory in children with FAS. These impairments are rooted in the structural and functional damage to critical brain regions, particularly the prefrontal cortex and hippocampus. Early identification and targeted support are vital to help affected individuals reach their full potential, but prevention remains the most effective approach. Avoiding alcohol during pregnancy is the only way to eliminate the risk of FAS and ensure healthy brain development for the baby.
Sealing Alcohol Ink on Ceramic Tiles: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Behavioral Issues: Hyperactivity, attention deficits, and difficulties with social interactions often observed
Babies and children with Fetal Alcohol Syndrome (FAS) often exhibit a range of behavioral issues that can significantly impact their daily lives and development. One of the most noticeable behavioral challenges is hyperactivity. Unlike typical infant behavior, where periods of activity are balanced with rest, babies with FAS may display constant, excessive movement that seems difficult to soothe. This hyperactivity can manifest as incessant squirming, difficulty staying still during feeding or play, and an inability to engage in calm, focused activities. Parents and caregivers may find it challenging to manage this behavior, as traditional methods of calming a baby, such as swaddling or gentle rocking, may be less effective.
Attention deficits are another common behavioral issue in babies and young children with FAS. These children often struggle to maintain focus on tasks or stimuli, even those that are typically engaging for infants, such as colorful toys or soothing sounds. For example, a baby with FAS might quickly lose interest in a rattle or a mobile, shifting their attention rapidly from one thing to another without sustained engagement. This lack of focus can hinder early developmental milestones, such as learning cause-and-effect relationships or developing problem-solving skills. Caregivers may notice that the child seems easily distracted, even in quiet, controlled environments.
Difficulties with social interactions are also frequently observed in babies with FAS. Typically, infants begin to show social engagement through behaviors like smiling, cooing, and making eye contact. However, babies with FAS may struggle to initiate or respond to these social cues. They might appear indifferent to caregivers' attempts to interact, or they may exhibit inappropriate responses, such as turning away during play or failing to reciprocate smiles. These challenges can create a barrier to forming secure attachments, which are crucial for emotional and social development. Over time, these difficulties can lead to more pronounced social problems, such as trouble understanding social norms or engaging with peers.
The combination of hyperactivity, attention deficits, and social interaction difficulties can create a complex behavioral profile that requires tailored interventions. Early intervention strategies, such as structured play activities, sensory integration therapy, and consistent routines, can help manage these behaviors. Caregivers play a critical role in providing a supportive environment that minimizes overstimulation and maximizes opportunities for positive engagement. It’s important to approach these challenges with patience and understanding, recognizing that the child’s behavior is a result of prenatal exposure to alcohol rather than intentional misbehavior.
Finally, it’s essential to monitor these behavioral issues as the child grows, as they can evolve into more significant challenges in later childhood and adolescence. For instance, hyperactivity may persist as impulsivity, attention deficits can lead to learning difficulties, and social interaction problems may result in isolation or conflict with peers. Early identification and intervention, combined with ongoing support from healthcare professionals, educators, and therapists, can help mitigate these long-term effects and improve outcomes for children with FAS.
Understanding the Reaction Products of Carboxylic Acids and Alcohols
You may want to see also
Explore related products

$17





![]()
Physical Abnormalities: Joint and limb deformities, heart defects, and kidney problems may occur
Fetal Alcohol Syndrome (FAS) can lead to a range of physical abnormalities in affected babies, with joint and limb deformities being among the most visible. Exposure to alcohol during critical stages of fetal development can disrupt the formation of bones and joints, resulting in shortened or malformed limbs. Common deformities include underdeveloped fingers or toes, fused digits, and abnormal joint positioning. These abnormalities are often symmetrical, affecting both sides of the body equally. For example, a baby with FAS might have arms that are shorter than expected or joints that appear stiff or misaligned. Early identification of these deformities is crucial, as some may require surgical intervention or physical therapy to improve function and mobility.
Heart defects are another significant physical abnormality associated with FAS, as alcohol exposure can interfere with the normal development of the fetal heart. Babies with FAS may be born with structural defects such as atrial or ventricular septal defects, where holes in the heart’s walls allow blood to flow improperly between chambers. Other issues include coarctation of the aorta, a narrowing of the major artery that carries blood from the heart, or problems with heart valves. These defects can lead to symptoms like rapid breathing, poor weight gain, and fatigue. In severe cases, surgical repair may be necessary to correct the defect and ensure proper heart function. Regular cardiac monitoring is essential for children with FAS to manage these conditions effectively.
Kidney problems are also prevalent in babies with FAS, as alcohol exposure can impair the development of renal structures. Affected infants may have underdeveloped or malformed kidneys, leading to issues such as reduced kidney function or urinary tract abnormalities. Hydronephrosis, a condition where urine backs up into the kidneys, is commonly observed. These kidney problems can increase the risk of urinary tract infections and, in severe cases, may lead to long-term renal complications. Early detection through ultrasound and ongoing monitoring are critical to managing these issues and preventing further damage. Parents and caregivers should be aware of signs like swelling, changes in urination patterns, or blood in the urine, which may indicate kidney dysfunction.
The combination of joint and limb deformities, heart defects, and kidney problems in babies with FAS underscores the systemic impact of prenatal alcohol exposure. These physical abnormalities are often lifelong and can significantly affect a child’s quality of life. For instance, joint and limb deformities may limit mobility and require assistive devices, while heart and kidney issues demand ongoing medical care. It is essential for healthcare providers to conduct comprehensive evaluations at birth to identify these abnormalities early. Additionally, educating parents about the importance of avoiding alcohol during pregnancy is critical in preventing FAS and its associated physical challenges.
In summary, babies with FAS often exhibit physical abnormalities such as joint and limb deformities, heart defects, and kidney problems, which are direct consequences of prenatal alcohol exposure. These conditions can range from mild to severe and may require specialized medical interventions. Recognizing these abnormalities early allows for timely management and support, improving outcomes for affected children. Awareness and prevention remain the most effective strategies to combat the devastating effects of FAS on infant health and development.
Quitting Alcohol Cold Turkey: Is It Safe?
You may want to see also
Frequently asked questions
Babies with FAS often exhibit distinct facial abnormalities, including a smooth ridge between the nose and upper lip (smooth philtrum), thin upper lip, small eye openings (short palpebral fissures), and a flat nasal bridge.
No, the severity and specific features of FAS can vary widely among affected babies, depending on the timing and amount of alcohol exposure during pregnancy.
While some babies with FAS may have subtle or less noticeable facial features, many will still exhibit at least some characteristic facial abnormalities, even if they are mild.
The facial features of FAS are typically most noticeable in infancy and early childhood, though they may become less pronounced as the child grows, depending on individual development.