Alcohol withdrawal seizures are a significant concern for individuals who abruptly stop or reduce heavy and prolonged alcohol consumption. These seizures typically occur within 6 to 48 hours after the last drink and are part of a broader spectrum of alcohol withdrawal symptoms, which can range from mild anxiety to severe complications like delirium tremens. Studies indicate that approximately 5% to 25% of individuals experiencing alcohol withdrawal will develop seizures, with the risk increasing in those with a history of multiple withdrawal episodes, high levels of alcohol dependence, or concurrent medical conditions. Early recognition and medical intervention are crucial, as untreated seizures can lead to life-threatening complications. Understanding the prevalence and risk factors of alcohol withdrawal seizures is essential for effective prevention and management in clinical settings.
Explore related products






What You'll Learn
- Prevalence Rates: Percentage of alcohol withdrawal cases that experience seizures
- Risk Factors: Key factors increasing seizure likelihood during alcohol withdrawal
- Timing of Seizures: Typical time frame for seizures to occur post-withdrawal
- Severity Levels: How seizure intensity varies in alcohol withdrawal cases
- Prevention Strategies: Methods to reduce seizure risk during alcohol withdrawal
![]()
Prevalence Rates: Percentage of alcohol withdrawal cases that experience seizures
Alcohol withdrawal seizures are a critical concern for individuals discontinuing heavy and prolonged alcohol use, yet their prevalence is often misunderstood. Studies indicate that approximately 5% to 10% of individuals undergoing alcohol withdrawal will experience seizures, with the majority occurring within 6 to 48 hours after the last drink. This narrow window underscores the importance of medical supervision during detoxification, particularly for those with a history of heavy drinking or prior withdrawal complications.
The risk of seizures escalates with the severity of alcohol dependence. For instance, individuals consuming more than 15 standard drinks per day or those with a history of multiple withdrawal episodes are at significantly higher risk. Age and overall health also play a role; younger adults and those without comorbidities may experience seizures less frequently than older individuals or those with chronic health conditions. Recognizing these risk factors allows healthcare providers to tailor interventions, such as benzodiazepine therapy, to mitigate seizure risk effectively.
Comparatively, alcohol withdrawal seizures are less common than other symptoms like tremors or anxiety, which affect up to 95% of patients. However, their potential severity—including the risk of progression to delirium tremens—makes them a critical focus. For example, while only 3% to 5% of alcohol withdrawal cases develop delirium tremens, seizures are often a precursor, highlighting their role as a red flag for more severe complications. This distinction emphasizes the need for proactive management rather than reactive treatment.
Practical tips for minimizing seizure risk include gradual tapering of alcohol intake under medical guidance, especially for those with a history of heavy use. Hydration, balanced nutrition, and monitoring for early withdrawal symptoms (e.g., agitation, elevated heart rate) are also essential. For high-risk individuals, inpatient detoxification with medications like diazepam or lorazepam can reduce seizure incidence by up to 80%, according to clinical guidelines. Understanding these prevalence rates and risk factors empowers both patients and providers to navigate alcohol withdrawal safely.
Are Champagne Cupcakes Alcoholic? Unveiling the Truth Behind the Recipe
You may want to see also
Explore related products






![]()
Risk Factors: Key factors increasing seizure likelihood during alcohol withdrawal
Alcohol withdrawal seizures are a serious and potentially life-threatening complication, occurring in approximately 5-25% of individuals undergoing alcohol withdrawal. While not everyone experiencing withdrawal will have seizures, certain risk factors significantly increase the likelihood. Understanding these factors is crucial for identifying individuals at higher risk and implementing appropriate preventive measures.
Duration and Severity of Alcohol Use: The longer and heavier the alcohol consumption, the greater the risk. Individuals with a history of chronic, heavy drinking (defined as more than 15 drinks per week for men and 8 drinks per week for women) are particularly vulnerable. Those who have been drinking heavily for years are more likely to experience seizures during withdrawal compared to those with a shorter history of alcohol abuse.
A sudden cessation of alcohol intake after prolonged heavy use can lead to a severe form of withdrawal known as delirium tremens (DTs), which is characterized by seizures, hallucinations, and confusion.
Previous Withdrawal Seizures: A history of seizures during previous withdrawal episodes is a strong predictor of future seizures. This indicates a heightened susceptibility to the neurological disruptions caused by alcohol withdrawal. Individuals with such a history require close medical supervision during any subsequent withdrawal attempts.
Rapid Detoxification: Attempting to quit alcohol "cold turkey" or undergoing rapid detoxification without medical supervision significantly increases the risk of seizures. The abrupt removal of alcohol, a central nervous system depressant, can lead to a rebound effect, causing hyperexcitability in the brain and triggering seizures.
Co-occurring Medical Conditions: Certain medical conditions can exacerbate the risk of seizures during alcohol withdrawal. These include:
- Liver disease: Impaired liver function can affect the metabolism of alcohol and its byproducts, leading to increased toxicity and seizure risk.
- Electrolyte imbalances: Dehydration and malnutrition, common in chronic alcoholics, can disrupt electrolyte balance, further increasing seizure susceptibility.
- Head injuries: Pre-existing brain injuries can lower the seizure threshold, making individuals more vulnerable during withdrawal.
Age and Genetics: While less well-defined, age and genetic predisposition may also play a role. Older individuals may be more susceptible due to age-related changes in brain function and metabolism. Additionally, genetic variations in enzymes involved in alcohol metabolism could influence individual vulnerability to withdrawal seizures.
Practical Tips for Risk Reduction:
- Seek Professional Help: Never attempt to detox from alcohol alone. Medical supervision is crucial for managing withdrawal symptoms and preventing complications like seizures.
- Gradual Tapering: In some cases, a gradual reduction in alcohol intake under medical guidance can help minimize withdrawal severity and seizure risk.
- Medications: Certain medications, such as benzodiazepines, can be used to manage withdrawal symptoms and prevent seizures.
- Hydration and Nutrition: Maintaining adequate hydration and nutrition is essential for supporting the body during withdrawal and reducing the risk of electrolyte imbalances.
By recognizing these risk factors and taking appropriate precautions, individuals can significantly reduce the likelihood of experiencing seizures during alcohol withdrawal and increase their chances of a safe and successful recovery.
The Stinging Truth Behind Alcohol and Wounds
You may want to see also
Explore related products






![]()
Timing of Seizures: Typical time frame for seizures to occur post-withdrawal
Alcohol withdrawal seizures typically emerge within a specific window after the last drink, a critical period that demands vigilance. Most seizures occur 6 to 48 hours post-withdrawal, with the highest risk peaking around 24 hours. This timeframe aligns with the body’s struggle to regain equilibrium as blood alcohol levels plummet. Heavy, long-term drinkers are particularly susceptible, as their brains have adapted to the constant presence of alcohol, leading to hyperexcitability when it’s abruptly removed. For context, individuals consuming more than 15 standard drinks per day (or 10 for women) over months or years fall into this high-risk category. Understanding this timing is crucial for caregivers and individuals alike, as prompt medical intervention during this window can prevent complications like status epilepticus, a life-threatening condition of prolonged seizures.
Consider the scenario of a 45-year-old man who has been drinking a fifth of vodka daily for a decade. If he suddenly stops, his risk of seizures spikes sharply within the first day. This isn’t merely a theoretical concern—studies show that up to 5% of untreated alcohol withdrawal cases result in seizures during this critical period. The mechanism behind this timing lies in the brain’s GABA and glutamate systems, which become dysregulated during chronic alcohol use. When alcohol is removed, glutamate activity surges, triggering neuronal overactivity that manifests as seizures. This biological process underscores why the first 48 hours are so perilous.
While the 6- to 48-hour window is the most common, seizures can occasionally occur outside this range. Some individuals experience delayed seizures up to 5 days post-withdrawal, particularly if they have a history of multiple withdrawal episodes or underlying health conditions like liver disease. This extended risk highlights the importance of monitoring symptoms beyond the initial 48 hours. Practical tips for caregivers include tracking the time since the last drink, observing for early withdrawal signs like tremors or anxiety, and having access to emergency medical contact information. Benzodiazepines, administered under medical supervision, are the gold standard for preventing seizures during this period, but they require precise timing and dosing to be effective.
Comparatively, alcohol withdrawal seizures differ from other types of seizures in their predictability. Unlike epileptic seizures, which can occur spontaneously, withdrawal seizures are directly tied to the cessation of alcohol and follow a relatively consistent timeline. This predictability offers a unique opportunity for prevention, but it also means that ignoring the warning signs during the critical 6- to 48-hour window can have dire consequences. For instance, a patient who dismisses mild tremors at 12 hours post-withdrawal might not seek help until a seizure occurs at 24 hours, when intervention is far more urgent.
In conclusion, the timing of alcohol withdrawal seizures is both precise and perilous, concentrated within the first 6 to 48 hours after cessation. This knowledge isn’t just academic—it’s actionable. For high-risk individuals, such as those with a history of heavy drinking, planning for this window is essential. Whether through medical detoxification, caregiver vigilance, or access to emergency care, understanding this timeline can mean the difference between a manageable withdrawal and a life-threatening event. The takeaway is clear: the clock starts ticking with the last drink, and the first 48 hours are decisive.
Does Ventolin Contain Alcohol? Uncovering the Truth About Its Ingredients
You may want to see also
Explore related products






![]()
Severity Levels: How seizure intensity varies in alcohol withdrawal cases
Alcohol withdrawal seizures are a critical concern, with studies indicating they occur in approximately 5-10% of individuals undergoing severe withdrawal. However, the intensity of these seizures varies widely, influenced by factors such as the duration and amount of alcohol consumption, individual health status, and the presence of co-occurring conditions. Understanding the severity levels of these seizures is crucial for timely intervention and management.
Severity Spectrum: From Mild to Life-Threatening
Seizures during alcohol withdrawal typically fall into three broad categories: mild, moderate, and severe. Mild seizures, often generalized tonic-clonic (GTC) seizures, are the most common, characterized by brief convulsions lasting less than 2-3 minutes. These are frequently observed in individuals with a history of chronic alcohol use but may not always require emergency intervention. Moderate seizures involve recurrent episodes within a 24-hour period, increasing the risk of complications like injury or aspiration pneumonia. Severe seizures, such as status epilepticus (prolonged seizures lasting over 5 minutes), are rare but life-threatening, demanding immediate medical attention.
Dosage and Duration: Key Determinants of Seizure Intensity
The severity of alcohol withdrawal seizures is closely tied to the amount and duration of alcohol consumption. Individuals consuming more than 10 standard drinks daily (140 grams of ethanol) for several years are at higher risk of severe seizures. Similarly, abrupt cessation after prolonged heavy drinking triggers more intense withdrawal symptoms, including seizures. For instance, a 40-year-old with a 10-year history of consuming 15 drinks daily is more likely to experience severe seizures compared to someone with a shorter or less intense drinking history.
Practical Tips for Risk Mitigation
To minimize seizure severity, gradual tapering of alcohol intake under medical supervision is recommended. Benzodiazepines, such as diazepam or lorazepam, are first-line treatments to prevent or manage seizures, with dosages tailored to the individual’s withdrawal symptoms and medical history. For example, a patient with mild withdrawal may receive 5-10 mg of diazepam every 6 hours, while someone at high risk of severe seizures might require higher doses or continuous infusion. Monitoring vital signs, electrolyte levels, and hydration status is equally critical, as imbalances can exacerbate seizure intensity.
Comparative Analysis: Age and Comorbidities
Age and comorbidities significantly influence seizure severity. Younger individuals (18-30 years) with no pre-existing health conditions may experience milder seizures, while older adults (over 50) or those with liver disease, malnutrition, or concurrent substance use are more prone to severe episodes. For instance, a 55-year-old with cirrhosis and a 20-year drinking history is at substantially higher risk of life-threatening seizures compared to a 25-year-old with a 5-year history. Tailoring management strategies to these factors is essential for optimal outcomes.
In summary, alcohol withdrawal seizures exhibit a wide severity spectrum, influenced by factors like alcohol consumption patterns, age, and health status. Recognizing these levels and implementing targeted interventions, such as benzodiazepine therapy and supportive care, can significantly reduce risks and improve patient outcomes.
How Prohibition Unintentionally Boosted the Soft Drink Industry
You may want to see also
Explore related products






![]()
Prevention Strategies: Methods to reduce seizure risk during alcohol withdrawal
Alcohol withdrawal seizures are a serious and potentially life-threatening complication, occurring in approximately 5-25% of individuals undergoing alcohol detoxification. This wide range highlights the variability in risk, influenced by factors such as the duration and severity of alcohol use, genetic predisposition, and overall health. To mitigate this risk, a multifaceted approach is essential, combining medical supervision, pharmacotherapy, and lifestyle adjustments.
Step 1: Medical Assessment and Monitoring
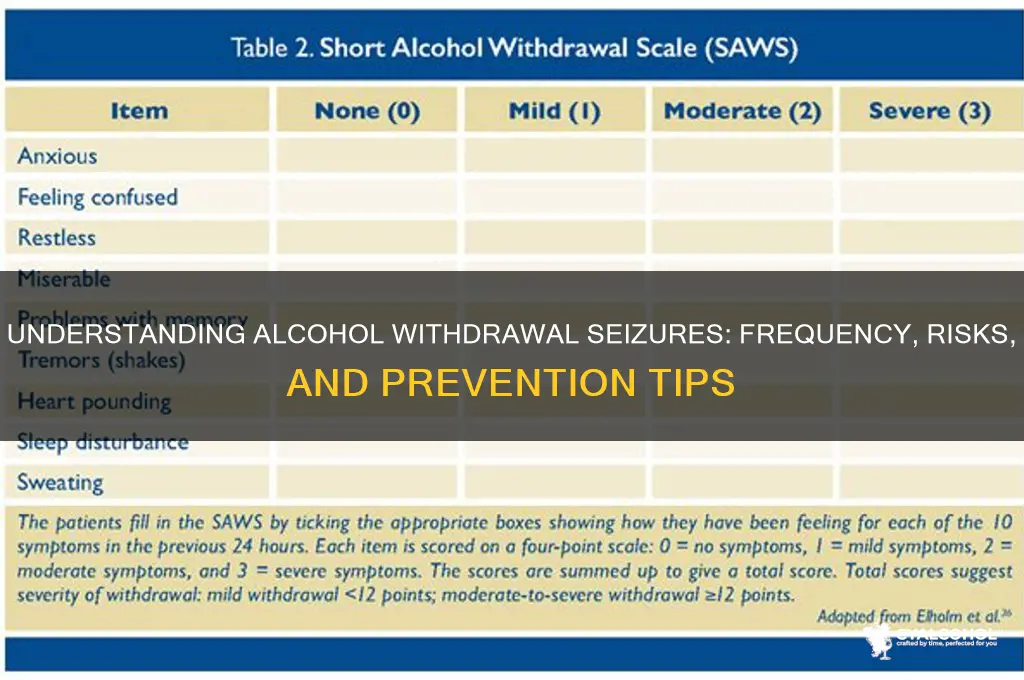
Begin with a thorough medical evaluation to identify high-risk individuals, such as those with a history of seizures, prolonged heavy drinking, or concurrent medical conditions. Continuous monitoring in a clinical setting is critical during the first 48-72 hours of withdrawal, as this is when seizures are most likely to occur. Vital signs, mental status, and withdrawal symptoms should be assessed regularly using tools like the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar).
Step 2: Pharmacological Interventions
Benzodiazepines remain the cornerstone of seizure prevention during alcohol withdrawal. These medications, such as diazepam (10-20 mg every 6-8 hours) or lorazepam (2-4 mg every 6-8 hours), modulate GABA receptors to reduce neuronal excitability. Dosage should be individualized based on symptom severity and tapered gradually to avoid dependence. In cases of benzodiazepine intolerance or contraindication, alternatives like carbamazepine (200 mg every 8 hours) or phenobarbital (260 mg daily) may be considered, though evidence is less robust.
Step 3: Nutritional Support and Hydration
Chronic alcohol use often leads to nutritional deficiencies, particularly in thiamine, magnesium, and electrolytes, which can exacerbate seizure risk. Administer intravenous thiamine (500 mg daily) to prevent Wernicke’s encephalopathy, a condition linked to seizures. Oral multivitamins and electrolyte replacement should also be provided. Adequate hydration is crucial, as dehydration can lower the seizure threshold.
Cautions and Considerations
While benzodiazepines are effective, they carry risks of oversedation, respiratory depression, and dependence, especially in older adults or those with hepatic impairment. Always assess for contraindications and monitor closely. Avoid abrupt discontinuation of alcohol or medications, as this can precipitate seizures. Patients with a history of liver disease require adjusted dosing due to altered drug metabolism.
Preventing seizures during alcohol withdrawal demands a proactive, individualized strategy. Combining medical oversight, targeted pharmacotherapy, and nutritional support maximizes safety and efficacy. Education on the risks of abrupt cessation and the importance of professional detoxification empowers individuals to seek timely care, reducing the likelihood of seizures and other complications.
How Boiling Point of Ethyl Alcohol Changes Physically
You may want to see also
Frequently asked questions
Alcohol withdrawal seizures occur in approximately 5-25% of individuals experiencing alcohol withdrawal, depending on the severity of their dependence and other factors.
Individuals with a history of heavy, long-term alcohol use, previous withdrawal seizures, or co-occurring medical conditions are at higher risk for alcohol withdrawal seizures.
Alcohol withdrawal seizures usually occur within 6 to 48 hours after the last drink, though they can sometimes appear up to 5 days after cessation of alcohol use.
Yes, alcohol withdrawal seizures can often be prevented with proper medical management, including supervised detoxification, medications like benzodiazepines, and gradual tapering of alcohol consumption under professional guidance.