Fetal Alcohol Syndrome (FAS) is a serious condition resulting from prenatal alcohol exposure, characterized by a range of physical, cognitive, and behavioral impairments. While some of its physical features, such as facial abnormalities, can be observed clinically, diagnosing the neurological and structural brain abnormalities associated with FAS can be more challenging. Magnetic Resonance Imaging (MRI) has emerged as a valuable tool in identifying these subtle brain changes, including alterations in brain volume, corpus callosum size, and white matter integrity. However, the question of whether FAS consistently shows up on MRI remains complex, as findings can vary depending on the severity of exposure, age of the individual, and the specific MRI techniques used. Despite these challenges, MRI plays a crucial role in understanding the neurodevelopmental impact of prenatal alcohol exposure and supporting early intervention efforts.
| Characteristics | Values |
|---|---|
| Brain Volume Reduction | Decreased total brain volume, particularly in the corpus callosum, basal ganglia, and cerebellum. |
| Corpus Callosum Abnormalities | Thinning, agenesis, or dysmorphology of the corpus callosum, a common finding in FAS. |
| Cerebellar Hypoplasia | Reduced size or underdevelopment of the cerebellum, often associated with motor and cognitive deficits. |
| Basal Ganglia Anomalies | Structural abnormalities in the basal ganglia, linked to movement and behavioral issues. |
| Cortical Malformations | Irregularities in the cerebral cortex, including pachygyria (thickened gyri) and polymicrogyria (excessive small gyri). |
| White Matter Abnormalities | Reduced white matter volume and altered microstructure, affecting neural connectivity. |
| Ventricular Enlargement | Dilatation of the ventricles, indicating possible atrophy or developmental issues. |
| Facial Dysmorphology (not directly visible on MRI) | While not an MRI finding, facial abnormalities (e.g., smooth philtrum, thin upper lip) are clinical indicators of FAS. |
| Diagnostic Sensitivity | MRI is highly sensitive for detecting structural brain abnormalities associated with FAS, but not all cases show definitive findings. |
| Age-Related Changes | Findings may become more pronounced with age, as developmental delays and brain maturation differences emerge. |
| Differential Diagnosis | MRI findings overlap with other neurodevelopmental disorders, requiring clinical correlation for definitive diagnosis. |
Explore related products






What You'll Learn
![]()
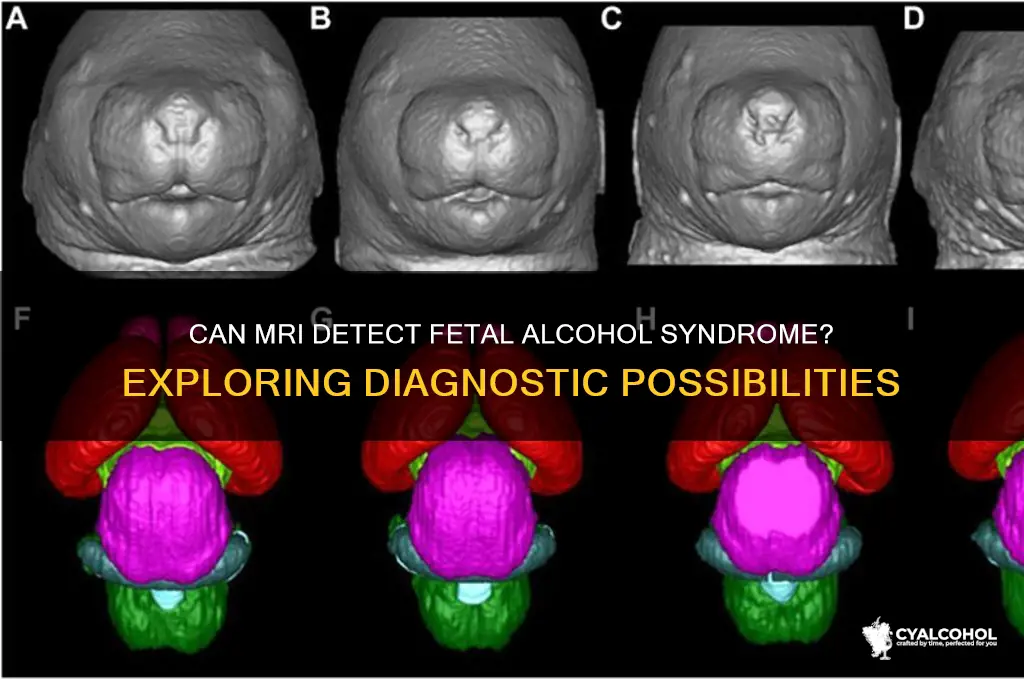
MRI detection of FAS brain abnormalities
Magnetic Resonance Imaging (MRI) has emerged as a valuable tool in the detection and assessment of brain abnormalities associated with Fetal Alcohol Spectrum Disorders (FASD), including Fetal Alcohol Syndrome (FAS). While FAS is primarily diagnosed through clinical evaluation of facial dysmorphology, growth deficits, and neurodevelopmental impairments, MRI provides a non-invasive means to visualize and quantify structural brain anomalies that may not be apparent through behavioral assessments alone. Research indicates that individuals with FAS often exhibit specific brain abnormalities, such as reduced brain volume, corpus callosum agenesis or dysgenesis, and alterations in the basal ganglia and cerebellum. These findings highlight the potential of MRI to complement clinical diagnosis by providing objective, anatomical evidence of alcohol-induced brain damage.
MRI detection of FAS-related brain abnormalities typically involves high-resolution structural imaging sequences, such as T1-weighted and T2-weighted scans, which allow for detailed visualization of brain tissue and structural integrity. Advanced MRI techniques, including diffusion tensor imaging (DTI) and voxel-based morphometry (VBM), further enhance the ability to detect subtle changes in white matter microstructure and regional gray matter volume, respectively. Studies have consistently shown that individuals with FAS have smaller total brain volumes, particularly in the cerebellum and frontal lobes, which are critical for motor coordination and executive functioning. The corpus callosum, the primary commissure connecting the cerebral hemispheres, is frequently found to be thinner or partially absent in affected individuals, a finding that correlates with deficits in interhemispheric communication and cognitive processing.
Another key area of focus in MRI detection of FAS is the basal ganglia, a group of subcortical nuclei involved in motor control and reward-based learning. Alcohol exposure during fetal development can lead to abnormalities in the caudate nucleus and putamen, which are detectable on MRI and associated with impairments in motor skills, attention, and behavior regulation. Additionally, MRI studies have identified alterations in the hippocampus, a region crucial for memory formation, which may explain the learning and memory difficulties commonly observed in individuals with FAS. These structural abnormalities are often accompanied by functional changes, though functional MRI (fMRI) is less commonly used in routine diagnostic settings due to its complexity and cost.
Despite its utility, MRI detection of FAS brain abnormalities is not without challenges. The variability in alcohol exposure levels and timing during pregnancy can result in a wide spectrum of brain anomalies, making it difficult to establish a standardized MRI profile for FAS. Furthermore, many of the brain changes observed in FAS overlap with those seen in other neurodevelopmental disorders, necessitating careful interpretation of imaging findings in the context of clinical history and behavioral assessments. Nonetheless, MRI remains a critical tool for confirming the presence of brain abnormalities in suspected cases of FAS, particularly when facial dysmorphology is subtle or absent, and for monitoring disease progression or response to intervention over time.
In conclusion, MRI plays a pivotal role in the detection and characterization of brain abnormalities associated with FAS, offering a window into the structural consequences of prenatal alcohol exposure. By identifying reductions in brain volume, corpus callosum anomalies, and alterations in key regions such as the basal ganglia and cerebellum, MRI provides objective evidence to support clinical diagnosis and inform targeted interventions. As research continues to refine MRI techniques and their application in FAS, this imaging modality will likely become an increasingly integral component of comprehensive FASD evaluation and management.
Moderate Drinking: What Does It Mean?
You may want to see also
Explore related products

$12.99





![]()
FAS-related structural changes visible on MRI
Fetal Alcohol Syndrome (FAS) is a condition resulting from prenatal alcohol exposure, characterized by a range of physical, cognitive, and behavioral impairments. Magnetic Resonance Imaging (MRI) has emerged as a valuable tool for identifying structural abnormalities associated with FAS, providing detailed insights into the brain's anatomy. One of the most consistent FAS-related structural changes visible on MRI is corpus callosum agenesis or hypoplasia. The corpus callosum, a bundle of nerve fibers connecting the brain's hemispheres, is often underdeveloped or partially absent in individuals with FAS. This anomaly can be clearly visualized on MRI scans, appearing as a thinning or complete absence of this critical structure, which correlates with cognitive and motor deficits observed in affected individuals.
Another significant finding on MRI is microcephaly, or reduced brain volume, which is a hallmark of FAS. Prenatal alcohol exposure disrupts normal brain development, leading to an overall decrease in brain size. MRI scans often reveal a smaller-than-normal cerebrum, particularly in the frontal and parietal lobes, which are critical for executive functioning, decision-making, and learning. Additionally, the ventricles—fluid-filled spaces in the brain—may appear enlarged due to the reduced brain tissue volume, a feature easily detectable on MRI.
Abnormalities in the basal ganglia and cerebellum are also commonly observed in FAS cases. The basal ganglia, involved in motor control and reward-based learning, may show reduced volume or altered morphology on MRI. Similarly, the cerebellum, essential for coordination and balance, often exhibits hypoplasia or structural irregularities in individuals with FAS. These changes are associated with the motor and coordination difficulties frequently seen in affected children.
White matter abnormalities are another key FAS-related finding on MRI. Prenatal alcohol exposure can disrupt myelination, the process of forming a protective sheath around nerve fibers. On MRI, this appears as diffuse white matter signal changes or reduced white matter volume, particularly in the frontal and temporal lobes. These alterations are linked to cognitive impairments, attention deficits, and poor academic performance in individuals with FAS.
Finally, facial dysmorphology, a clinical feature of FAS, can also be indirectly supported by MRI findings. While MRI primarily focuses on brain structures, the presence of brain abnormalities in conjunction with characteristic facial features (e.g., smooth philtrum, thin upper lip) strengthens the diagnosis. Advanced MRI techniques, such as diffusion tensor imaging (DTI), can further elucidate microstructural changes in the brain, providing a more comprehensive understanding of FAS-related neuropathology. In summary, MRI plays a crucial role in identifying FAS-related structural changes, offering a non-invasive means to assess the extent of brain damage caused by prenatal alcohol exposure.
Alcohol's Impact: Sweaty Hands and Feet
You may want to see also
Explore related products






![]()
MRI accuracy in diagnosing fetal alcohol syndrome
MRI technology has been increasingly utilized in the diagnosis of Fetal Alcohol Spectrum Disorders (FASD), including Fetal Alcohol Syndrome (FAS), due to its non-invasive nature and ability to provide detailed images of the brain. However, the accuracy of MRI in diagnosing FAS is a topic of ongoing research, as the condition presents with subtle and variable brain abnormalities that can be challenging to detect. Studies have shown that MRI can identify specific structural anomalies associated with FAS, such as reduced corpus callosum size, microcephaly, and alterations in the basal ganglia. These findings are crucial because they align with the neurodevelopmental impairments observed in individuals with FAS, such as cognitive deficits and behavioral issues. Despite these advancements, the sensitivity and specificity of MRI in diagnosing FAS remain limited, particularly in cases where the abnormalities are mild or atypical.
One of the primary challenges in using MRI for FAS diagnosis is the lack of standardized criteria for interpreting imaging results. The brain abnormalities in FAS can be highly variable, and not all individuals with the condition exhibit the same structural changes. This variability makes it difficult to establish a definitive set of MRI markers for FAS. Additionally, many of the brain anomalies seen in FAS overlap with those found in other neurodevelopmental disorders, such as ADHD or autism, further complicating the diagnostic process. Researchers are working to develop more refined imaging protocols and analytical tools to improve the accuracy of MRI in identifying FAS-specific patterns, but these efforts are still in the early stages.
Advances in MRI techniques, such as diffusion tensor imaging (DTI) and functional MRI (fMRI), have shown promise in enhancing the diagnostic accuracy for FAS. DTI, for example, can detect microstructural changes in white matter tracts, which are often disrupted in individuals with FAS. These disruptions correlate with impairments in executive function and motor skills, providing additional evidence of alcohol-related brain damage. Similarly, fMRI can reveal functional abnormalities in brain networks, offering insights into the cognitive and behavioral deficits associated with FAS. While these advanced techniques improve the sensitivity of MRI in detecting FAS, they are not yet widely available in clinical settings and require further validation.
Another factor influencing MRI accuracy in FAS diagnosis is the age of the individual being scanned. Brain abnormalities in FAS may be more pronounced in early childhood, making MRI more effective during this developmental stage. However, as individuals age, the brain undergoes significant changes, and some FAS-related anomalies may become less apparent or harder to distinguish from age-related variations. This underscores the importance of early intervention and the need for longitudinal studies to track how MRI findings evolve over time in individuals with FAS.
In conclusion, while MRI is a valuable tool in the diagnosis of FAS, its accuracy is currently limited by the complexity and variability of the condition. Ongoing research aims to refine MRI techniques and establish clearer diagnostic criteria to improve its utility. For now, MRI should be used as part of a comprehensive diagnostic approach that includes clinical assessments, behavioral evaluations, and a detailed history of prenatal alcohol exposure. As technology advances, MRI is likely to play an increasingly important role in identifying and understanding the neurobiological impact of FAS.
Confronting an Alcoholic: Tips for a Tough Conversation
You may want to see also
Explore related products






![]()
Brain regions affected by FAS on MRI
Fetal Alcohol Spectrum Disorders (FASD), including Fetal Alcohol Syndrome (FAS), are characterized by a range of physical, behavioral, and cognitive impairments resulting from prenatal alcohol exposure. Magnetic Resonance Imaging (MRI) has emerged as a valuable tool for identifying structural brain abnormalities associated with FAS. Research consistently highlights several key brain regions that are particularly vulnerable to the teratogenic effects of alcohol. These regions include the corpus callosum, cerebellum, basal ganglia, and cortical areas, with each showing distinct patterns of alteration on MRI.
One of the most consistently reported findings in FAS is a reduction in the size of the corpus callosum, the primary commissure connecting the two cerebral hemispheres. MRI studies frequently reveal thinning or complete agenesis of this structure, which is critical for interhemispheric communication. This abnormality is thought to underlie some of the cognitive and motor coordination difficulties observed in individuals with FAS. The corpus callosum's susceptibility to alcohol exposure during early fetal development makes it a hallmark feature in neuroimaging studies of FAS.
The cerebellum, another region highly sensitive to prenatal alcohol exposure, often exhibits volume reductions and structural abnormalities on MRI. This brain area plays a crucial role in motor control, balance, and cognitive functions such as attention and language. Cerebellar hypoplasia, or underdevelopment, is a common finding in FAS and correlates with the fine motor and coordination challenges faced by affected individuals. Additionally, the cerebellar vermis, a midline structure, is frequently noted to be dysmorphic or reduced in size, further emphasizing the cerebellum's vulnerability.
Cortical abnormalities are also evident in FAS, with MRI studies showing reductions in overall brain volume, cortical thinning, and altered gyrification patterns. The frontal and temporal lobes, which are involved in executive functioning, memory, and social behavior, are particularly affected. These regions' developmental disruptions contribute to the cognitive deficits, learning difficulties, and behavioral problems commonly associated with FAS. Advanced MRI techniques, such as diffusion tensor imaging (DTI), have further revealed microstructural abnormalities in white matter tracts connecting these cortical areas, highlighting the widespread impact of alcohol on brain connectivity.
The basal ganglia, critical for motor function and reward-based learning, are another set of structures affected by prenatal alcohol exposure. MRI studies often detect volume reductions in the caudate nucleus and putamen, which are part of the basal ganglia network. These changes are associated with the motor impairments and difficulties with goal-directed behavior observed in individuals with FAS. Additionally, alterations in the amygdala and hippocampus, regions involved in emotional regulation and memory, have been reported, though less consistently than the aforementioned areas.
In summary, MRI studies have identified specific brain regions affected by FAS, including the corpus callosum, cerebellum, basal ganglia, and cortical areas. These structural abnormalities provide critical insights into the neurobiological basis of the cognitive, motor, and behavioral challenges faced by individuals with FAS. While MRI is a powerful tool for detecting these changes, ongoing research is essential to refine diagnostic criteria and understand the full spectrum of brain alterations associated with prenatal alcohol exposure.
Alcohol and Diarrhea: What's the Link?
You may want to see also
Explore related products






![]()
Limitations of MRI in FAS diagnosis
While Magnetic Resonance Imaging (MRI) is a valuable tool in diagnosing various neurological conditions, its effectiveness in definitively diagnosing Fetal Alcohol Spectrum Disorders (FASD), including Fetal Alcohol Syndrome (FAS), has limitations. One of the primary constraints is the lack of specificity in the brain abnormalities associated with FAS. MRI can detect structural anomalies such as reduced brain volume, corpus callosum agenesis, and abnormalities in the basal ganglia, but these findings are not exclusive to FAS. Similar brain changes can occur in other neurodevelopmental disorders, such as ADHD, autism, or genetic syndromes, making it challenging to attribute these findings solely to prenatal alcohol exposure.
Another limitation is the variability in brain development and the subtle nature of some FAS-related abnormalities. Not all individuals with FAS exhibit overt structural changes detectable by MRI, especially in mild or moderate cases. The brain alterations in FAS can be diffuse and involve microstructural changes that standard MRI sequences may not capture. Advanced techniques like diffusion tensor imaging (DTI) or functional MRI (fMRI) might provide more detailed insights, but these are not routinely used in clinical practice and require specialized expertise for interpretation.
MRI is also limited in its ability to correlate imaging findings with functional or behavioral deficits. While structural abnormalities may be present, their relationship to cognitive, behavioral, or developmental impairments in FAS is not always clear-cut. This makes it difficult to use MRI as a standalone diagnostic tool, as it cannot confirm prenatal alcohol exposure or predict the severity of FASD-related disabilities. Clinical assessment, including detailed history of maternal alcohol use and neurodevelopmental evaluations, remains essential for diagnosis.
Furthermore, MRI is not universally accessible or feasible for all patients. The procedure can be costly, time-consuming, and requires the individual to remain still for extended periods, which may be challenging for children with developmental or behavioral issues. Additionally, MRI is contraindicated in individuals with certain medical devices or conditions, further limiting its utility in FAS diagnosis. These practical considerations underscore the need for a multidisciplinary approach that integrates imaging with clinical and behavioral assessments.
Lastly, the absence of FAS-specific biomarkers or patterns on MRI means that negative findings do not rule out the condition. Prenatal alcohol exposure can cause functional and cognitive impairments without significant structural abnormalities, making MRI an incomplete tool for diagnosis. Relying solely on MRI may lead to false negatives, emphasizing the importance of combining imaging with other diagnostic modalities. In summary, while MRI can contribute to the evaluation of FAS, its limitations in specificity, sensitivity, and practical application highlight the need for a comprehensive diagnostic framework.
Alcohol and Bowel Cancer: What's the Connection?
You may want to see also
Frequently asked questions
No, fetal alcohol syndrome does not always show up on an MRI. While MRI can detect certain brain abnormalities associated with FAS, such as reduced brain volume or structural changes, not all individuals with FAS will have visible abnormalities on imaging.
MRI findings associated with FAS can include reduced corpus callosum size, microcephaly (small head size), abnormalities in the basal ganglia, and overall reduced brain volume. However, these findings are not exclusive to FAS and may require clinical correlation.
No, an MRI cannot definitively diagnose fetal alcohol syndrome. Diagnosis relies on a combination of clinical evaluation, developmental history, physical examination, and imaging findings. MRI is a supportive tool, not a standalone diagnostic test.
Fetal alcohol syndrome can be detected on an MRI at any age, but abnormalities may be more apparent in childhood or adolescence when the brain is still developing. Early detection is possible, but subtle changes may not be visible in infancy.
While MRI is the most sensitive imaging modality for detecting brain abnormalities associated with FAS, other tests like CT scans or ultrasound may be used in certain cases. However, MRI remains the preferred choice due to its superior detail and lack of radiation exposure.































