Fetal alcohol exposure (FAE) is a significant public health concern, as it can result from maternal alcohol consumption during pregnancy and lead to a range of adverse effects on the developing fetus. One critical area of investigation is whether FAE causes external abnormalities in the affected individuals. These abnormalities may include distinctive facial features, growth deficiencies, and other visible anomalies that can serve as indicators of prenatal alcohol exposure. Understanding the link between FAE and external abnormalities is essential for early identification, intervention, and prevention strategies, as well as for raising awareness about the risks associated with alcohol use during pregnancy. Research in this field not only sheds light on the developmental consequences of FAE but also emphasizes the importance of public health initiatives aimed at reducing alcohol consumption among pregnant women.
| Characteristics | Values |
|---|---|
| Facial Features | Smooth philtrum, thin upper lip, small palpebral fissures, flat nasal bridge, short upturned nose |
| Growth Deficits | Below-average height, weight, and head circumference at birth and throughout childhood |
| Skeletal Abnormalities | Joint abnormalities, curved spine (scoliosis), hip dislocation, shortened limbs |
| Organ Malformations | Heart defects (e.g., atrial septal defect, ventricular septal defect), kidney abnormalities, hearing and vision impairments |
| Neurodevelopmental Impairments | Microcephaly (small head circumference), cognitive deficits, learning disabilities, attention deficits, poor coordination |
| Skin Abnormalities | Excessive skin folds at the back of the neck, pale skin, strawberry-shaped birthmarks (hemangiomas) |
| Limb Anomalies | Shortened fingers or toes, fused digits (syndactyly), absent or underdeveloped limbs (rare) |
| Prevalence | Occurs in approximately 1-5 per 1,000 live births, depending on the population and diagnostic criteria |
| Diagnosis | Based on prenatal alcohol exposure history, characteristic facial features, growth deficits, and neurodevelopmental impairments |
| Prevention | Complete abstinence from alcohol during pregnancy is the only sure way to prevent fetal alcohol spectrum disorders (FASDs) |
Explore related products






What You'll Learn
![]()
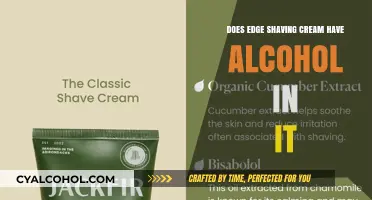
Facial anomalies linked to prenatal alcohol exposure
Prenatal alcohol exposure is a well-documented cause of a range of developmental issues, including distinct facial anomalies that are often grouped under the term Fetal Alcohol Spectrum Disorders (FASD). These facial abnormalities are among the most recognizable physical signs of fetal alcohol exposure and can serve as critical diagnostic features. The typical facial features associated with FASD include a smooth ridge between the nose and upper lip (smooth philtrum), a thin upper lip, and small eye openings (palpebral fissures). These characteristics are often referred to as the "sentinel facial features" and are present in individuals with the most severe form of the condition, known as Fetal Alcohol Syndrome (FAS). The smooth philtrum, in particular, is a highly specific indicator of prenatal alcohol exposure, as it is rarely seen in the general population without this exposure.
The development of these facial anomalies is linked to the disruptive effects of alcohol on the migrating neural crest cells during the first trimester of pregnancy. Neural crest cells play a crucial role in the formation of the face and other structures. When exposed to alcohol, these cells may fail to migrate properly or undergo apoptosis (programmed cell death), leading to the characteristic facial abnormalities. The severity of these anomalies can vary, but their presence is a strong indicator of the teratogenic effects of alcohol on the developing fetus. Early recognition of these facial features is essential for timely intervention and support for affected individuals.
In addition to the smooth philtrum, thin upper lip, and small palpebral fissures, other facial anomalies may be present in individuals with prenatal alcohol exposure. These can include a flattened midface, a shorter than average nose, and an abnormal groove on the upper lip. These features are often less specific than the sentinel facial features but contribute to the overall facial phenotype associated with FASD. It is important to note that while these anomalies are more pronounced in FAS, milder forms of prenatal alcohol exposure can still result in subtle facial changes that may require careful examination by a trained professional to detect.
The persistence of these facial anomalies into adulthood underscores the permanent nature of the damage caused by prenatal alcohol exposure. Unlike some other aspects of FASD, which may become less apparent over time, the facial features remain a lifelong marker of the condition. This permanence highlights the importance of prevention efforts, as there is no cure for FASD. Public health initiatives aimed at educating women about the risks of alcohol consumption during pregnancy are crucial in reducing the incidence of these facial anomalies and other associated disabilities.
Diagnosing facial anomalies linked to prenatal alcohol exposure requires a comprehensive approach, including detailed medical history, physical examination, and sometimes additional assessments. Healthcare providers should be trained to recognize the subtle and overt signs of FASD, as early diagnosis can lead to better outcomes through targeted interventions. These interventions may include educational support, behavioral therapy, and medical management of associated conditions. By understanding and addressing the facial anomalies associated with prenatal alcohol exposure, healthcare professionals can play a vital role in improving the quality of life for affected individuals and their families.
Cooking with Sherry: Does Alcohol Evaporate When Cooking?
You may want to see also
Explore related products

$12.99





![]()
Limb and joint defects in affected fetuses
Fetal alcohol exposure (FAE) is a well-documented cause of congenital abnormalities, including limb and joint defects. These defects are part of a broader spectrum of disorders known as Fetal Alcohol Spectrum Disorders (FASDs), with Fetal Alcohol Syndrome (FAS) being the most severe form. Limb and joint abnormalities in affected fetuses are primarily attributed to the teratogenic effects of ethanol on developing embryonic and fetal tissues, particularly during critical periods of organogenesis. The severity and type of defects can vary depending on the timing, duration, and dosage of alcohol exposure during pregnancy.
One of the most common limb defects associated with FAE is upper limb reduction anomalies, particularly involving the fingers and hands. Affected individuals may exhibit shortened or absent fingers (brachydactyly or adactyly), fusion of digits (syndactyly), or abnormal bending or positioning of the fingers (clinodactyly). These defects arise from disrupted development of the apical ectodermal ridge (AER), a critical signaling center in limb bud development, which is highly sensitive to alcohol-induced cell death and impaired proliferation. The hands are more frequently affected than the feet, likely due to the earlier developmental stage of the upper limbs during the period of peak vulnerability to alcohol exposure.
Joint abnormalities in fetuses exposed to alcohol often manifest as joint contractures or limited range of motion, particularly in the elbows, knees, and hips. These issues are thought to result from alcohol-induced alterations in musculoskeletal development, including impaired migration and differentiation of mesenchymal cells, which form the precursors to cartilage and bone. Additionally, alcohol exposure can disrupt the formation of articular cartilage, leading to malformed or underdeveloped joints. Over time, these structural abnormalities can contribute to functional impairments, such as difficulty with mobility or fine motor skills, in affected individuals.
Another significant limb defect linked to FAE is limb length discrepancies, where one limb is noticeably shorter than the other. This asymmetry is believed to stem from alcohol's interference with the growth plates (epiphyseal plates) in long bones, which regulate longitudinal bone growth. Ethanol exposure can cause premature fusion of these growth plates, leading to stunted growth in the affected limb. Limb length discrepancies can have profound implications for posture, gait, and overall physical function, often requiring orthopedic interventions to address.
Finally, radioulnar synostosis, a condition where the radius and ulna bones in the forearm fuse together, is also observed in some fetuses with FAE. This abnormality restricts forearm rotation and can significantly impair hand function. The exact mechanism by which alcohol causes radioulnar synostosis is not fully understood but is thought to involve disruptions in the differentiation and organization of skeletal precursors during early limb development. Early detection and surgical intervention may be necessary to improve functional outcomes in affected individuals.
In summary, limb and joint defects in fetuses exposed to alcohol are diverse and can range from mild to severe, depending on the extent of exposure and developmental timing. These abnormalities underscore the critical importance of avoiding alcohol consumption during pregnancy to prevent irreversible congenital malformations. Healthcare providers play a key role in educating expectant mothers about the risks of FAE and in identifying and managing affected individuals to optimize their long-term outcomes.
Famous People Living with Fetal Alcohol Syndrome
You may want to see also
Explore related products






![]()
Growth deficiencies caused by alcohol consumption during pregnancy
Fetal alcohol exposure is a significant concern during pregnancy, as it can lead to a range of developmental issues, including growth deficiencies. When a pregnant individual consumes alcohol, it crosses the placenta and enters the fetus's bloodstream, disrupting normal growth and development. This interference can result in both immediate and long-term growth deficiencies, affecting various aspects of the child's physical and cognitive development. The severity of these deficiencies often depends on the timing, frequency, and amount of alcohol consumed during pregnancy.
One of the most noticeable growth deficiencies caused by alcohol consumption during pregnancy is intrauterine growth restriction (IUGR). IUGR occurs when the fetus does not grow at the expected rate, leading to a birth weight significantly below average. This condition is directly linked to alcohol's ability to restrict blood flow through the placenta, reducing the delivery of essential nutrients and oxygen to the developing fetus. As a result, affected infants often exhibit stunted length, weight, and head circumference, which can persist into childhood and adolescence. These physical abnormalities are often accompanied by developmental delays, further highlighting the detrimental impact of alcohol on fetal growth.
Alcohol exposure during pregnancy can also lead to skeletal and muscular abnormalities, contributing to long-term growth deficiencies. The developing fetal bones and muscles are particularly vulnerable to the toxic effects of alcohol, which can disrupt cell division and differentiation. This disruption may result in shortened limbs, joint abnormalities, and reduced muscle mass. For instance, children with fetal alcohol spectrum disorders (FASD) often present with limb anomalies, such as shorter than average fingers and limbs, which are directly attributable to prenatal alcohol exposure. These structural defects not only affect physical appearance but also impair mobility and functional abilities, impacting overall growth and quality of life.
In addition to physical growth deficiencies, alcohol consumption during pregnancy can impair organ development, particularly the brain and heart. The brain is highly sensitive to alcohol during critical periods of development, leading to microcephaly (an abnormally small head) and neurological deficits. Microcephaly is a visible external abnormality that often signifies underlying brain damage, including reduced brain volume and cognitive impairments. Similarly, alcohol exposure can disrupt heart development, leading to congenital heart defects, which may manifest as external abnormalities like chest deformities or visible signs of cardiac distress in severe cases. These organ-specific growth deficiencies underscore the systemic impact of alcohol on fetal development.
Lastly, the growth deficiencies caused by prenatal alcohol exposure often extend beyond infancy, affecting long-term growth trajectories. Children exposed to alcohol in utero frequently experience delayed puberty, slower growth rates, and reduced adult height compared to their peers. This prolonged impact is attributed to the irreversible damage alcohol causes to developing tissues and organs during critical periods of growth. Early intervention and supportive care can mitigate some of these effects, but prevention remains the most effective strategy. Avoiding alcohol consumption during pregnancy is crucial to ensuring optimal fetal growth and preventing the external and internal abnormalities associated with fetal alcohol exposure.
Starting an Alcohol Company: UK Guide
You may want to see also
Explore related products






![]()
Skin abnormalities associated with fetal alcohol exposure
Fetal alcohol exposure (FAE) is a significant concern during pregnancy, as it can lead to a range of developmental issues, including external abnormalities. Among these, skin abnormalities are notable and can serve as visible indicators of prenatal alcohol exposure. One of the most commonly observed skin-related issues in individuals with fetal alcohol spectrum disorders (FASD) is cutaneous dysmorphology, which refers to unusual skin features that arise due to disrupted fetal development. These abnormalities often manifest as thinned, translucent skin, which may appear more delicate and prone to bruising or damage. This occurs because alcohol interferes with the normal development of the dermal layer, reducing collagen production and affecting skin elasticity.
Another skin abnormality associated with FAE is the presence of vascular anomalies, such as telangiectasias or spider angiomas. These are small, dilated blood vessels that appear as red or purple spots on the skin's surface. Alcohol exposure during critical periods of fetal development can disrupt the formation of blood vessels, leading to these visible abnormalities. Additionally, individuals with FASD may exhibit striae, or stretch marks, even in the absence of rapid growth or weight gain. These striae are often more pronounced and widespread than those seen in the general population, further highlighting the impact of alcohol on skin integrity.
Hyperpigmentation and hypopigmentation are also observed in cases of fetal alcohol exposure. These conditions result in uneven skin tone, with patches of skin appearing darker or lighter than the surrounding areas. The exact mechanism behind these pigmentary changes is not fully understood, but it is believed that alcohol disrupts melanocyte function and distribution during fetal development. Such pigmentary abnormalities can be particularly distressing for affected individuals, as they are highly visible and may lead to social stigma.
Furthermore, FAE can impair the skin's ability to heal and regenerate, leading to delayed wound healing and an increased susceptibility to infections. This is due to alcohol's detrimental effects on the immune system and the skin's barrier function. As a result, individuals with FASD may experience prolonged healing times for cuts, scrapes, or surgical incisions, along with a higher risk of scarring. These skin-related issues underscore the importance of early detection and intervention in cases of prenatal alcohol exposure.
Lastly, cutaneous tags and nevi (moles) are more frequently observed in individuals with FASD. These benign skin growths are thought to arise from disruptions in cell proliferation and differentiation during fetal development. While typically harmless, their presence can serve as a clinical marker for underlying developmental abnormalities associated with alcohol exposure. Recognizing these skin abnormalities is crucial for healthcare providers, as they can prompt further evaluation for other FASD-related conditions and ensure appropriate support and management for affected individuals.
Alcohol Sales: Stadium Entry Rules Explained
You may want to see also
Explore related products






![]()
Organ malformations due to maternal alcohol use
Maternal alcohol use during pregnancy can have profound and lasting effects on fetal development, leading to a range of organ malformations. The developing fetus is highly susceptible to the teratogenic effects of alcohol, which can disrupt critical stages of organogenesis. Alcohol, or ethanol, crosses the placenta freely, exposing the fetus to the same concentration of alcohol as the mother. This exposure can interfere with cell proliferation, differentiation, and migration, resulting in structural abnormalities in various organs. The severity of these malformations often correlates with the timing, duration, and amount of alcohol consumption during pregnancy.
One of the most well-documented organ systems affected by maternal alcohol use is the cardiovascular system. Fetal alcohol exposure increases the risk of congenital heart defects, including septal defects, tetralogy of Fallot, and patent ductus arteriosus. These abnormalities arise from disrupted development of the heart’s structures during the first trimester, a critical period for cardiac morphogenesis. Ethanol-induced oxidative stress and apoptosis in cardiac cells are believed to contribute to these malformations, which can lead to lifelong cardiovascular complications for the affected individual.
The central nervous system (CNS) is another major target of alcohol-induced damage. Maternal alcohol consumption can result in neural tube defects, microcephaly, and abnormalities in brain structure, such as reduced corpus callosum size and altered cortical development. These malformations are often associated with functional impairments, including cognitive deficits, learning disabilities, and behavioral problems. The CNS is particularly vulnerable to alcohol exposure throughout pregnancy, as neurodevelopment is a prolonged process that continues into the third trimester.
Alcohol exposure can also lead to renal and skeletal malformations. The kidneys, which develop in the first trimester, may exhibit dysplasia or agenesis, impairing renal function. Skeletal abnormalities, such as shortened limbs, joint contractures, and facial dysmorphology, are common in fetal alcohol spectrum disorders (FASD). These defects are thought to result from ethanol’s interference with mesenchymal cell differentiation and bone matrix formation. Additionally, the liver may be affected, with hepatomegaly and fatty infiltration observed in some cases.
Finally, the risk of organ malformations due to maternal alcohol use underscores the importance of prevention and early intervention. There is no known safe level of alcohol consumption during pregnancy, and even moderate drinking can pose risks. Healthcare providers play a critical role in educating women about the potential harms of alcohol use during pregnancy and offering support for abstinence. Early identification of affected children is essential for implementing interventions that can mitigate the long-term consequences of these organ malformations.
Alcohol and Your Colon: What's the Connection?
You may want to see also
Frequently asked questions
No, fetal alcohol exposure does not always lead to visible external abnormalities. While some individuals with Fetal Alcohol Spectrum Disorders (FASD) may exhibit facial anomalies such as a smooth philtrum, thin upper lip, or small eye openings, many affected individuals show no external signs, making diagnosis more challenging.
The most common external abnormalities linked to fetal alcohol exposure include distinctive facial features like a smooth ridge between the nose and upper lip (philtrum), thin upper lip, small head circumference (microcephaly), and smaller-than-average eyes. These features are often collectively referred to as the "FAS facial phenotype."
While some physical abnormalities, such as growth deficiencies, may improve with proper nutrition and medical care, the distinctive facial features associated with fetal alcohol exposure are typically permanent. Early intervention and supportive therapies can help manage associated developmental and cognitive challenges.
No, external abnormalities are just one aspect of fetal alcohol exposure. More significant concerns include cognitive impairments, behavioral issues, learning disabilities, and developmental delays, which can have long-term impacts on an individual's functioning and quality of life.