The relationship between alcohol consumption and ferritin levels has garnered significant attention in medical research, as both factors play crucial roles in overall health. Ferritin, a protein that stores iron in the body, serves as a key indicator of iron status, while alcohol usage is known to influence various physiological processes, including liver function and nutrient metabolism. Studies suggest that chronic alcohol consumption may lead to elevated ferritin levels, potentially due to liver damage, inflammation, or disruptions in iron regulation. However, the exact mechanisms and the extent of this relationship remain complex, with individual factors such as the amount and duration of alcohol intake, genetic predispositions, and dietary habits also playing a role. Understanding this connection is essential for identifying risks associated with alcohol-related health issues and managing conditions like hemochromatosis or liver disease.
| Characteristics | Values |
|---|---|
| Effect of Alcohol on Ferritin Levels | Alcohol consumption, especially chronic and heavy drinking, is associated with increased ferritin levels. |
| Mechanism | Alcohol-induced liver damage (e.g., steatosis, fibrosis) leads to increased iron storage and reduced iron export, elevating ferritin. |
| Type of Alcohol | Both beer and spirits have been linked to higher ferritin levels, though the effect may vary by type and quantity. |
| Gender Differences | Men are more likely to experience elevated ferritin levels due to alcohol consumption compared to women, possibly due to differences in iron metabolism. |
| Dose-Dependent Effect | Higher alcohol intake correlates with greater increases in ferritin levels. |
| Reversibility | Reducing or abstaining from alcohol can lead to a decrease in ferritin levels over time. |
| Health Implications | Elevated ferritin due to alcohol may indicate liver damage or iron overload, increasing the risk of conditions like hemochromatosis or liver disease. |
| Confounding Factors | Other factors like diet, obesity, and genetic predisposition can also influence ferritin levels, complicating the direct link to alcohol. |
| Diagnostic Use | Elevated ferritin levels in heavy drinkers may serve as a marker for alcohol-related liver disease or iron dysregulation. |
| Latest Research Findings | Recent studies reinforce the positive correlation between alcohol consumption and ferritin levels, emphasizing the need for moderation and monitoring. |
Explore related products






What You'll Learn
![]()
Alcohol's Impact on Iron Absorption
Alcohol consumption, even in moderate amounts, can significantly disrupt the delicate balance of iron metabolism in the body. Studies indicate that chronic alcohol use impairs the intestinal absorption of iron, a critical process for maintaining healthy ferritin levels. This disruption occurs through multiple mechanisms: alcohol damages the intestinal lining, reducing its capacity to absorb nutrients, and it interferes with the production of gastroduodenal mucosal cells, which play a key role in iron uptake. For instance, individuals consuming more than 60 grams of alcohol daily (roughly equivalent to 4–5 standard drinks) are at higher risk for iron deficiency anemia, despite potentially elevated ferritin levels due to liver inflammation.
While the relationship between alcohol and ferritin levels may seem counterintuitive, it’s essential to distinguish between ferritin as an iron storage protein and its role as an acute-phase reactant. Alcohol-induced liver damage triggers inflammation, which can falsely elevate ferritin levels as part of the body’s stress response. This increase does not reflect improved iron status but rather systemic inflammation. For example, a study published in the *Journal of Hepatology* found that heavy drinkers often exhibit high ferritin levels alongside low serum iron, a paradoxical condition known as "anemia of chronic disease."
To mitigate alcohol’s impact on iron absorption, practical steps can be taken. First, limit alcohol intake to recommended guidelines: up to one drink per day for women and two for men. Second, pair alcohol consumption with iron-rich foods like spinach, lentils, or red meat, but avoid simultaneous intake of iron supplements, as alcohol can hinder their absorption. Third, incorporate vitamin C-rich foods (e.g., oranges, bell peppers) into meals, as vitamin C enhances non-heme iron absorption. For those with concerns about iron status, consulting a healthcare provider for a comprehensive blood panel, including ferritin, transferrin saturation, and liver enzymes, is crucial.
Comparatively, the effects of alcohol on iron metabolism differ from those of other substances. For instance, caffeine in coffee or tea can inhibit iron absorption when consumed in large amounts, but unlike alcohol, it does not cause systemic inflammation or liver damage. Similarly, while calcium supplements can reduce iron absorption, they do not disrupt intestinal function or induce chronic inflammation. Alcohol’s dual role in impairing absorption and causing inflammation makes it uniquely detrimental to iron homeostasis, particularly in heavy drinkers or those with pre-existing liver conditions.
In conclusion, while alcohol may elevate ferritin levels due to inflammation, it simultaneously undermines iron absorption and utilization. This dual effect highlights the complexity of alcohol’s impact on the body’s iron stores. For individuals concerned about their iron status, reducing alcohol intake, adopting a balanced diet, and seeking medical advice are proactive steps to maintain optimal health. Understanding this nuanced relationship is key to addressing misconceptions and promoting informed decisions about alcohol consumption and iron management.
Rosacea-Friendly Alcohol Choices: Best Drinks to Minimize Flare-Ups
You may want to see also
Explore related products





![]()
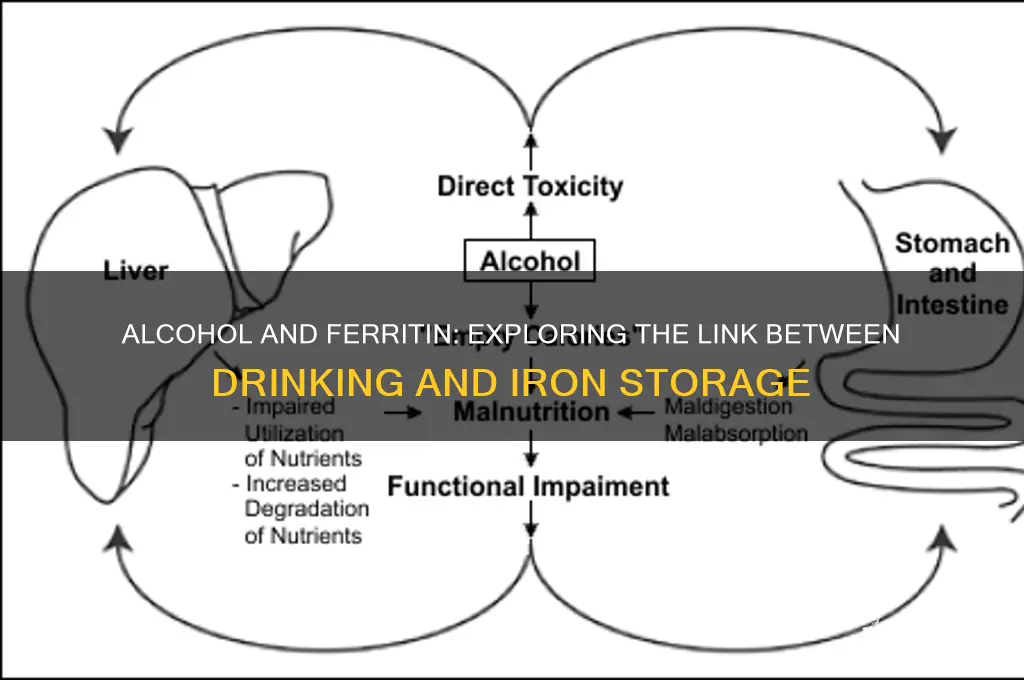
Liver Function and Ferritin Production
Alcohol consumption, even in moderate amounts, can significantly impact liver function, which in turn affects ferritin production and regulation. The liver plays a pivotal role in iron metabolism, storing and releasing ferritin—a protein that binds iron—to maintain systemic iron balance. Chronic alcohol use disrupts this process by inducing hepatic inflammation and oxidative stress, leading to increased ferritin levels. This elevation is not a sign of improved iron status but rather a marker of liver damage, as the organ struggles to manage iron effectively.
To understand this relationship, consider the liver’s dual role in ferritin production and iron storage. Normally, the liver synthesizes ferritin to sequester excess iron, preventing it from causing cellular damage. However, alcohol-induced liver injury impairs this regulatory mechanism. Studies show that heavy drinkers (defined as >60g of alcohol/day for men and >40g/day for women) often exhibit elevated serum ferritin levels, even in the absence of iron overload disorders like hemochromatosis. This is because alcohol metabolites, such as acetaldehyde, promote the release of pro-inflammatory cytokines, which stimulate ferritin synthesis as a protective response to oxidative stress.
Practical tips for managing this risk include limiting alcohol intake to recommended guidelines (up to 14 units/week for adults, spread over several days) and monitoring liver health through regular blood tests, including ferritin and liver enzyme levels. For individuals with pre-existing liver conditions or iron disorders, complete abstinence from alcohol may be advised. Additionally, incorporating antioxidants like vitamin E and selenium into the diet can help mitigate alcohol-induced oxidative damage, though these measures should complement, not replace, reduced alcohol consumption.
Comparatively, non-alcoholic fatty liver disease (NAFLD) also elevates ferritin levels, but the mechanism differs. In NAFLD, insulin resistance drives increased iron absorption and ferritin synthesis, whereas alcohol directly damages hepatocytes. This distinction highlights the importance of identifying the root cause of elevated ferritin—whether alcohol-related or not—to tailor interventions effectively. For instance, while lifestyle changes like weight loss benefit NAFLD, alcohol cessation is non-negotiable for reversing alcohol-induced liver damage.
In conclusion, the link between alcohol usage and ferritin levels underscores the liver’s central role in iron homeostasis. Elevated ferritin in the context of alcohol consumption is a red flag for liver dysfunction, not a benign finding. By understanding this relationship, individuals can take proactive steps to protect liver health, ensuring ferritin serves its intended purpose—safeguarding the body from iron toxicity—rather than becoming a marker of harm.
Guayaki Yerba Mate Alcohol Content: Facts and Misconceptions Explained
You may want to see also
Explore related products
![Ecological Formulas - Ferritin Fe 5 mg 60 caps [Health and Beauty]](https://m.media-amazon.com/images/I/710LgacTtiL._AC_UY218_.jpg)





![]()
Inflammation and Ferritin Levels
Alcohol consumption is known to induce inflammation, a response that can significantly impact ferritin levels. Ferritin, an iron-storage protein, is not merely a marker of iron status but also an acute-phase reactant, meaning its levels rise during inflammatory processes. When alcohol is metabolized, it triggers the release of pro-inflammatory cytokines, such as TNF-alpha and IL-6, which stimulate the liver to produce more ferritin. This mechanism explains why even moderate alcohol intake (e.g., 1-2 drinks per day) can lead to elevated ferritin levels, often misinterpreted as a sign of iron overload.
To understand the practical implications, consider a scenario where a 45-year-old individual with no history of liver disease consumes 30 grams of alcohol daily (approximately 2 standard drinks). Over time, this habit could lead to chronic inflammation, causing ferritin levels to rise above the normal range (typically 30–400 ng/mL for men and 15–150 ng/mL for women). Clinicians must differentiate between inflammation-induced ferritin elevation and true iron overload, as misdiagnosis could lead to unnecessary phlebotomy or iron chelation therapy. A key differentiator is the absence of elevated transferrin saturation in inflammatory cases.
From a preventive perspective, reducing alcohol intake is a straightforward strategy to mitigate inflammation-driven ferritin increases. For instance, limiting alcohol to 14 units per week (as recommended by many health guidelines) can help maintain ferritin levels within a healthy range. Additionally, incorporating anti-inflammatory foods such as turmeric, ginger, and omega-3 fatty acids may counteract alcohol-induced inflammation. Regular monitoring of ferritin levels, particularly in individuals with a history of heavy drinking, is essential to detect early signs of dysregulation.
Comparatively, non-alcoholic fatty liver disease (NAFLD) also elevates ferritin due to inflammation, but the absence of alcohol consumption makes the diagnostic pathway clearer. In contrast, alcohol-related inflammation complicates the picture, often requiring additional tests like liver enzymes (AST, ALT) and imaging to assess liver health. This highlights the importance of a detailed patient history, including alcohol consumption patterns, when interpreting ferritin results. By addressing both alcohol usage and inflammation, individuals can better manage their ferritin levels and overall health.
Pink Whitney's Secret: Unveiling the Alcohol in This Popular Drink
You may want to see also
Explore related products






![]()
Alcohol-Induced Hemolysis Effects
Alcohol consumption, particularly in excess, can trigger a cascade of physiological responses, one of which is alcohol-induced hemolysis. This process involves the premature destruction of red blood cells (RBCs), leading to the release of hemoglobin and subsequent iron overload in the body. While the relationship between alcohol and ferritin levels is complex, hemolysis plays a pivotal role in this dynamic. When RBCs rupture, the iron they carry is released into the bloodstream, often binding to ferritin—a protein that stores iron—as a protective mechanism against free radical damage. Chronic alcohol users, especially those consuming more than 60 grams of alcohol per day (approximately 4-5 standard drinks), are at higher risk of experiencing this phenomenon.
Hemolysis induced by alcohol can occur through multiple mechanisms. Direct toxicity to RBC membranes, oxidative stress, and the activation of the immune system all contribute to cellular breakdown. For instance, acetaldehyde, a metabolite of alcohol, can bind to RBC membranes, making them more susceptible to rupture. Additionally, alcohol-induced deficiencies in nutrients like folate and vitamin B12 further compromise RBC integrity. Individuals with pre-existing conditions such as glucose-6-phosphate dehydrogenase (G6PD) deficiency are particularly vulnerable, as their RBCs are already predisposed to hemolysis under stress.
The implications of alcohol-induced hemolysis extend beyond immediate symptoms like fatigue or jaundice. Over time, the excess iron released from hemolyzed RBCs can lead to elevated ferritin levels, a condition known as hyperferritinemia. While ferritin is essential for iron storage, chronically high levels can contribute to systemic inflammation and organ damage, particularly in the liver. This is especially concerning for heavy drinkers, as the liver is already under strain from alcohol metabolism. Monitoring ferritin levels in this population is crucial, as it can serve as an early indicator of both hemolysis and potential iron overload disorders.
Practical steps can mitigate the risk of alcohol-induced hemolysis and its consequences. Limiting alcohol intake to moderate levels—up to one drink per day for women and two for men—is a foundational recommendation. Supplementing with antioxidants like vitamin C and E can help counteract oxidative stress, while ensuring adequate intake of folate and B12 supports RBC health. Regular blood tests to monitor ferritin and liver function are essential for chronic drinkers, particularly those over 40, whose bodies may be less resilient to alcohol’s effects. For those with G6PD deficiency or other hemolytic conditions, complete abstinence from alcohol may be necessary to prevent complications.
In summary, alcohol-induced hemolysis is a significant yet often overlooked consequence of excessive drinking. Its role in elevating ferritin levels underscores the intricate relationship between alcohol, RBC health, and iron metabolism. By understanding the mechanisms and risks, individuals can take proactive steps to protect their health, ensuring that occasional indulgence does not become a chronic hazard.
Exploring the Sober-Curious Trend: Why People Are Cutting Back
You may want to see also
Explore related products
![Iron Deficiency Test Kit for Home Use [1 Pack] – Rapid & Accurate Ferritin Test for Adults, Children, Men & Women | at-Home Anemia Screening with 99.5% Accuracy](https://m.media-amazon.com/images/I/61LULXJWLwL._AC_UL320_.jpg)




![]()
Chronic Drinking and Iron Overload
Chronic alcohol consumption is a known risk factor for iron overload, a condition where excess iron accumulates in the body, often reflected in elevated ferritin levels. Ferritin, a protein that stores iron, serves as a biomarker for iron status, and its elevation can indicate both acute and chronic issues. Studies have shown that heavy drinkers, defined as those consuming more than 60 grams of alcohol daily (approximately 4-5 standard drinks), are particularly susceptible to this phenomenon. The liver, a primary site of iron metabolism and alcohol processing, becomes compromised under the dual stress of ethanol and iron accumulation, leading to conditions like alcoholic liver disease (ALD) and hemochromatosis.
The mechanism linking alcohol to iron overload involves both increased intestinal absorption of iron and impaired iron regulation. Alcohol disrupts the gut barrier, allowing more dietary iron to enter the bloodstream, while simultaneously inhibiting hepcidin, a hormone that regulates iron release from cells. This double-edged effect results in a surplus of iron that the body cannot efficiently expel. For instance, a study published in *Gastroenterology* found that chronic drinkers had ferritin levels up to 50% higher than non-drinkers, with the most significant increases observed in individuals with pre-existing liver damage. This highlights the compounding risks for those already vulnerable.
Practical steps to mitigate iron overload in chronic drinkers include dietary modifications and medical monitoring. Reducing red meat and iron-fortified foods can lower dietary iron intake, while increasing consumption of foods rich in polyphenols (e.g., green tea, berries) may inhibit iron absorption. Clinicians often recommend regular blood tests to monitor ferritin and transferrin saturation levels, particularly for individuals over 40 or those with a family history of hemochromatosis. In severe cases, therapeutic phlebotomy—the removal of blood to reduce iron stores—may be necessary, though this is typically reserved for patients with ferritin levels exceeding 1,000 ng/mL.
A comparative analysis reveals that while moderate drinkers (up to 14 grams of alcohol daily) do not typically experience significant iron overload, the threshold for risk escalates sharply beyond this limit. For example, a 2019 study in *Alcoholism: Clinical and Experimental Research* demonstrated that individuals consuming 80 grams of alcohol daily had a threefold higher risk of developing iron overload compared to moderate drinkers. This underscores the importance of moderation, particularly for those genetically predisposed to iron-related disorders.
In conclusion, chronic drinking and iron overload are intricately linked through mechanisms involving gut permeability, hepcidin suppression, and liver dysfunction. Awareness of this relationship is critical for both healthcare providers and individuals at risk, as early intervention can prevent severe complications such as cirrhosis and cardiovascular disease. By combining lifestyle adjustments with medical oversight, the adverse effects of alcohol-induced iron overload can be effectively managed, offering a pathway to better health for those affected.
Is Alcoholism a Disability? Understanding Legal and Medical Perspectives
You may want to see also
Frequently asked questions
Yes, chronic alcohol consumption can lead to increased ferritin levels due to liver inflammation and damage, which disrupts iron metabolism.
Short-term alcohol use typically does not significantly impact ferritin levels, as it requires prolonged consumption to cause noticeable changes in iron storage.
Moderate alcohol consumption is less likely to raise ferritin levels, but individual responses vary, and factors like liver health and diet also play a role.