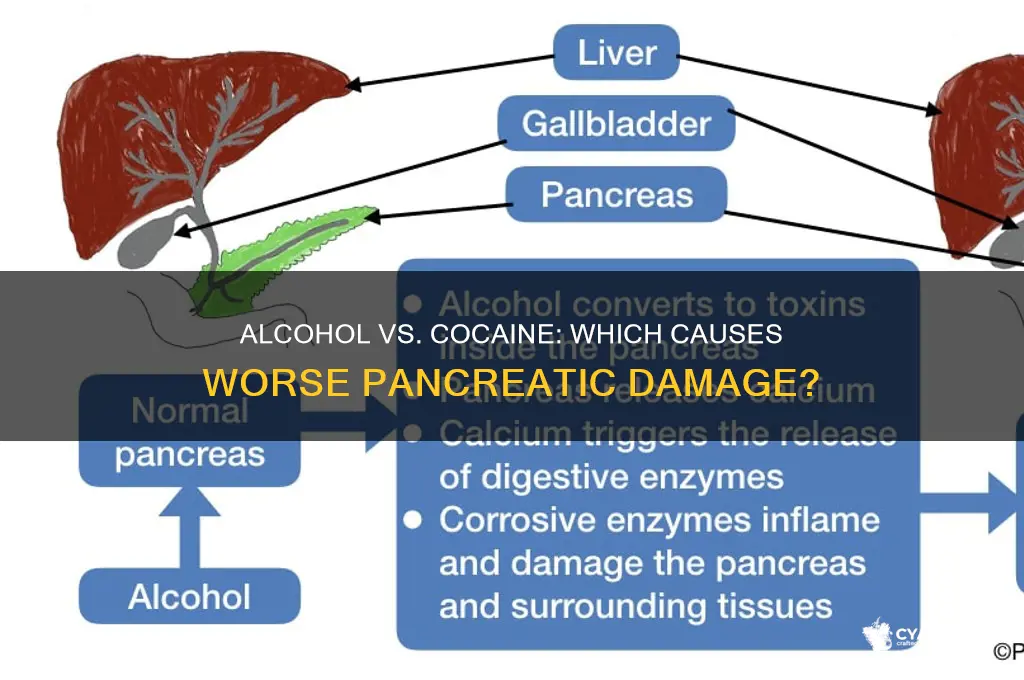
The impact of substance abuse on the pancreas is a critical yet often overlooked area of study, particularly when examining the effects of alcohol and cocaine. Both substances have been linked to pancreatic damage, albeit through different mechanisms. Chronic alcohol consumption can lead to pancreatitis, an inflammation of the pancreas, by causing premature activation of digestive enzymes within the organ, leading to self-digestion and tissue damage. On the other hand, cocaine use is associated with vasoconstriction, reducing blood flow to the pancreas and potentially causing ischemia, which can result in acute pancreatitis. Understanding the distinct pathways through which these substances harm the pancreas is essential for developing targeted interventions and raising awareness about the long-term health risks associated with their use.
| Characteristics | Values |
|---|---|
| Alcohol and Pancreas | Chronic alcohol use is a leading cause of pancreatitis, both acute and chronic. Alcohol-induced pancreatitis is associated with inflammation and damage to pancreatic tissue. |
| Mechanism of Alcohol Damage | Alcohol metabolites (e.g., acetaldehyde) directly toxic to pancreatic cells. Increased pancreatic duct pressure and activation of digestive enzymes within the pancreas contribute to tissue damage. |
| Risk Factors for Alcohol-Induced Pancreatitis | Heavy, long-term alcohol consumption; genetic predisposition; smoking; and poor nutrition. |
| Cocaine and Pancreas | Cocaine use is associated with acute pancreatitis, often through vasoconstriction (reduced blood flow) and increased catecholamine levels, leading to pancreatic ischemia and inflammation. |
| Mechanism of Cocaine Damage | Cocaine causes vasospasm in pancreatic arteries, reducing blood flow and oxygen supply. Increased stress hormones (e.g., norepinephrine) further exacerbate pancreatic injury. |
| Risk Factors for Cocaine-Induced Pancreatitis | Concurrent alcohol or opioid use; high-dose or frequent cocaine consumption; and pre-existing vascular conditions. |
| Comparative Risk | Alcohol is a more established and common cause of chronic pancreatitis, while cocaine is more strongly linked to acute pancreatitis episodes. |
| Long-Term Effects | Alcohol: Chronic pancreatitis, pancreatic insufficiency, and increased risk of pancreatic cancer. Cocaine: Recurrent acute pancreatitis and potential for pancreatic fibrosis. |
| Treatment and Management | Both require cessation of substance use. Alcohol-induced pancreatitis may require dietary changes and enzyme replacement. Cocaine-induced cases focus on symptom management and addressing complications. |
| Prevention | Limiting alcohol intake and avoiding cocaine use are key preventive measures. |
Explore related products





What You'll Learn
![]()
Alcohol-induced pancreatitis risks
Excessive alcohol consumption is a well-documented risk factor for pancreatitis, a painful and potentially life-threatening inflammation of the pancreas. The pancreas, a vital organ responsible for producing digestive enzymes and regulating blood sugar, can become severely damaged when exposed to chronic alcohol abuse. Studies show that heavy drinking, defined as consuming more than 4-5 alcoholic beverages per day for men and 3 per day for women, significantly increases the likelihood of developing acute or chronic pancreatitis. The mechanism involves alcohol metabolites triggering inflammation and disrupting the normal function of pancreatic cells, leading to enzyme activation within the pancreas itself, causing autodigestion and tissue damage.
Consider the case of a 45-year-old man who consumes 6-8 beers daily for over a decade. Despite appearing otherwise healthy, he begins experiencing severe abdominal pain, nausea, and unexplained weight loss. These symptoms, classic indicators of pancreatitis, often go unrecognized until the condition has progressed. Diagnosis typically involves blood tests to measure elevated pancreatic enzymes (amylase and lipase) and imaging studies like CT scans or ultrasounds to assess pancreatic damage. Early intervention is critical, as untreated pancreatitis can lead to complications such as pancreatic necrosis, pseudocysts, or even organ failure.
Preventing alcohol-induced pancreatitis requires a proactive approach. For individuals at risk, reducing alcohol intake is paramount. Guidelines suggest limiting consumption to no more than 2 drinks per day for men and 1 for women. However, complete abstinence is recommended for those with a history of pancreatitis or heavy drinking. Incorporating a low-fat diet can also alleviate stress on the pancreas, as high-fat meals stimulate enzyme production. Regular medical check-ups, particularly for liver and pancreatic function, are essential for early detection and management of alcohol-related damage.
Comparatively, while cocaine use is also associated with pancreatitis, the mechanisms differ. Cocaine-induced pancreatitis often occurs acutely due to vasoconstriction and ischemia, whereas alcohol’s effects are cumulative and dose-dependent. Unlike cocaine, alcohol’s impact on the pancreas is reversible in the early stages if consumption is halted. However, chronic alcohol abuse can lead to irreversible damage, such as chronic pancreatitis, which increases the risk of pancreatic cancer and diabetes. This distinction underscores the importance of addressing alcohol use specifically when discussing pancreatitis prevention.
In conclusion, alcohol-induced pancreatitis is a preventable yet serious condition linked to prolonged heavy drinking. By understanding the risks, recognizing symptoms, and adopting healthier habits, individuals can protect their pancreatic health. For those struggling with alcohol dependence, seeking professional help is crucial. Programs combining behavioral therapy, medication, and support groups have proven effective in reducing alcohol consumption and mitigating associated health risks. Prioritizing pancreatic health today can prevent debilitating complications tomorrow.
Air France: Alcohol Availability on International Flights
You may want to see also
Explore related products

$17.24 $22.33





![]()
Cocaine’s impact on pancreatic function
Cocaine, a potent stimulant, exerts profound and multifaceted effects on the pancreas, often leading to acute and chronic complications. One of the most immediate risks is acute pancreatitis, a sudden inflammation of the pancreas that can occur even after a single high-dose use (typically 1.5–2 grams or more in a short period). This condition is characterized by severe abdominal pain, nausea, and elevated levels of pancreatic enzymes like amylase and lipase. The mechanism involves cocaine-induced vasoconstriction, which restricts blood flow to the pancreas, causing tissue ischemia and necrosis. Chronic cocaine users, particularly those who consume the drug via smoking or injection, face a 5–10 times higher risk of pancreatitis compared to non-users, according to studies published in the *Journal of Addiction Medicine*.
Beyond acute episodes, cocaine disrupts normal pancreatic function by interfering with its endocrine and exocrine roles. The drug stimulates excessive dopamine release, which indirectly affects insulin secretion, leading to pancreatic beta-cell dysfunction. This can result in hyperglycemia or, paradoxically, hypoglycemia due to erratic insulin production. Long-term users often exhibit insulin resistance, a precursor to type 2 diabetes. For individuals aged 25–45, who represent the highest demographic of cocaine users, this means an accelerated risk of metabolic disorders, even in the absence of obesity or familial predisposition.
A lesser-known but critical consequence is cocaine-induced pancreatic fibrosis, a scarring process that impairs the organ’s ability to produce digestive enzymes. This occurs due to repeated episodes of inflammation and oxidative stress, which cocaine exacerbates by depleting antioxidant defenses. Over time, fibrosis can progress to pancreatic insufficiency, where the body cannot properly digest fats and proteins, leading to malnutrition and weight loss. Users who combine cocaine with alcohol—a common practice—experience compounded damage, as alcohol independently harms the pancreas, creating a synergistic effect that accelerates tissue degradation.
Practical steps to mitigate cocaine’s pancreatic impact include hydration, as dehydration worsens vasoconstriction, and avoiding binge patterns of use, which spike toxicity levels. For those in recovery, monitoring pancreatic enzyme levels and undergoing regular glucose tolerance tests can detect early damage. However, the most effective strategy remains abstinence, as even moderate cocaine use (e.g., 0.5–1 gram weekly) can cumulatively stress the pancreas over months or years. For healthcare providers, recognizing pancreatitis in cocaine users requires a low threshold for diagnostic imaging and enzyme testing, as symptoms are often attributed to other causes, delaying treatment.
In summary, cocaine’s impact on the pancreas is both immediate and long-lasting, ranging from acute inflammation to chronic metabolic dysfunction. Its ability to disrupt blood flow, insulin regulation, and tissue integrity underscores the urgency of addressing cocaine use as a public health priority. While damage may not always be reversible, early intervention and lifestyle modifications can prevent irreversible harm, offering a pathway to recovery for affected individuals.
Diagnosing Fetal Alcohol Syndrome in Adults: What to Know
You may want to see also
Explore related products






![]()
Chronic alcohol vs. pancreas health
Chronic alcohol consumption is a well-documented risk factor for pancreatic damage, with long-term heavy drinking leading to a spectrum of pancreatic disorders. The pancreas, a vital organ responsible for producing digestive enzymes and regulating blood sugar, is particularly vulnerable to the toxic effects of alcohol. Studies show that individuals who consume more than 4-5 standard drinks per day (approximately 50-60 grams of ethanol) over several years are at significantly higher risk of developing pancreatitis, a painful inflammation of the pancreas. This condition can progress to chronic pancreatitis, characterized by irreversible damage, fibrosis, and loss of pancreatic function. Unlike acute pancreatitis, which can sometimes resolve with abstinence, chronic pancreatitis often requires lifelong management and can lead to complications like diabetes and pancreatic cancer.
The mechanism behind alcohol-induced pancreatic damage is multifaceted. Alcohol metabolism in the pancreas generates toxic byproducts, such as acetaldehyde and free radicals, which directly injure pancreatic cells. Additionally, alcohol disrupts the normal flow of pancreatic enzymes, causing them to activate prematurely within the pancreas instead of the small intestine. This leads to autodigestion, where the pancreas essentially begins to digest itself. Heavy drinking also impairs the body’s antioxidant defenses, exacerbating oxidative stress and inflammation. Notably, the risk of pancreatic damage is dose-dependent, meaning the more alcohol consumed, the greater the likelihood of harm. Even individuals with a genetic predisposition to pancreatic disease, such as carriers of the PRSS1 mutation, face accelerated deterioration when they consume alcohol regularly.
To mitigate the risk of alcohol-related pancreatic damage, practical steps can be taken. First, limit daily alcohol intake to no more than 1-2 standard drinks for women and 2-3 for men, as recommended by health guidelines. For those with a history of pancreatitis or pancreatic disease, complete abstinence is strongly advised. Incorporating a diet rich in antioxidants (e.g., fruits, vegetables, and nuts) can help counteract oxidative stress caused by alcohol. Regular monitoring of pancreatic enzymes (amylase and lipase) and blood sugar levels is essential for heavy drinkers, especially those over 40, as age increases susceptibility to pancreatic issues. Finally, seeking support for alcohol reduction or cessation, such as through counseling or support groups, can be a critical step in preserving pancreatic health.
Comparatively, while cocaine use is also associated with acute pancreatitis, its impact on the pancreas differs from that of chronic alcohol consumption. Cocaine-induced pancreatitis is often linked to ischemia (reduced blood flow) and vasoconstriction, rather than direct toxic effects on pancreatic tissue. Unlike alcohol, cocaine’s pancreatic damage is typically reversible if use is discontinued promptly. However, combining cocaine with alcohol—a common practice—amplifies the risk of pancreatitis, as alcohol enhances cocaine’s vasoconstrictive effects. This highlights the importance of addressing polysubstance use in pancreatic health management. While both substances harm the pancreas, chronic alcohol use poses a more persistent and progressive threat, making it a primary focus for long-term pancreatic care.
In conclusion, chronic alcohol consumption is a major driver of pancreatic damage, with heavy drinking significantly increasing the risk of pancreatitis, fibrosis, and pancreatic insufficiency. The dose-dependent nature of this risk underscores the importance of moderation or abstinence. Practical measures, such as dietary adjustments and regular health monitoring, can help mitigate damage, but the most effective strategy remains reducing alcohol intake. While cocaine also harms the pancreas, its effects are generally less chronic and more reversible compared to alcohol. Prioritizing awareness and intervention for alcohol-related pancreatic issues is essential for preventing irreversible harm and improving long-term health outcomes.
Massachusetts Alcohol Tax: What You Need to Know About Excise Duties
You may want to see also
Explore related products






![]()
Cocaine-related pancreatic inflammation
Cocaine use, even in small doses, can trigger acute pancreatitis, a sudden inflammation of the pancreas that requires immediate medical attention. Unlike chronic pancreatitis, which develops over time, acute cases linked to cocaine are often severe and unpredictable. Studies show that even a single use of cocaine, particularly in doses exceeding 1 gram, can lead to pancreatic damage. The mechanism involves vasoconstriction—cocaine narrows blood vessels, reducing blood flow to the pancreas and causing tissue death. This condition is not limited to long-term users; even first-time or occasional users are at risk, especially when combined with alcohol or other stimulants.
Recognizing the symptoms of cocaine-induced pancreatitis is critical for timely intervention. Common signs include severe abdominal pain, nausea, vomiting, and a rapid heartbeat. The pain often radiates to the back and worsens after eating. If these symptoms appear after cocaine use, seek emergency care immediately. Delaying treatment can lead to complications like pancreatic necrosis, pseudocysts, or systemic organ failure. Healthcare providers may use blood tests to detect elevated levels of amylase and lipase, enzymes indicative of pancreatic inflammation.
Preventing cocaine-related pancreatic inflammation begins with abstaining from cocaine use. However, for those struggling with addiction, harm reduction strategies can mitigate risks. Avoid mixing cocaine with alcohol, as this combination significantly increases the likelihood of pancreatitis. Stay hydrated, as dehydration exacerbates vasoconstriction. If you or someone you know uses cocaine, educate them about the risks and encourage regular health check-ups to monitor pancreatic function. Rehabilitation programs and support groups can provide the necessary tools to quit cocaine and protect long-term health.
Comparing cocaine-induced pancreatitis to alcohol-related cases highlights the unique dangers of cocaine. While alcohol typically causes chronic pancreatitis after years of heavy drinking (defined as >4-5 drinks daily for men and >3 for women), cocaine can damage the pancreas after a single use. Alcohol’s effects are dose-dependent and cumulative, whereas cocaine’s impact is immediate and often irreversible. This distinction underscores the urgency of addressing cocaine use, especially among younger adults aged 18–35, who represent the majority of cocaine-related pancreatitis cases.
In conclusion, cocaine-related pancreatic inflammation is a severe, preventable condition that demands awareness and action. Understanding the risks, recognizing symptoms, and adopting harm reduction strategies can save lives. Whether you’re a healthcare provider, user, or concerned friend, prioritizing education and intervention is key to combating this dangerous consequence of cocaine use.
Alcohol and Skin Hydration: Uncovering the Truth Behind Dehydration Myths
You may want to see also
Explore related products





![]()
Combined effects of alcohol and cocaine
Both alcohol and cocaine independently pose significant risks to pancreatic health, but their combined effects create a uniquely dangerous synergy. When alcohol, a known pancreatic toxin, is mixed with cocaine, a potent vasoconstrictor, the pancreas faces a dual assault. Alcohol disrupts pancreatic function by inducing inflammation and impairing enzyme secretion, while cocaine reduces blood flow to the organ, exacerbating tissue damage. This combination amplifies the risk of acute pancreatitis, a condition where the pancreas becomes severely inflamed, potentially leading to life-threatening complications. Studies show that individuals who use both substances are at a substantially higher risk compared to those who use either alone.
Consider the metabolic pathways involved. Cocaine increases dopamine levels, which can heighten alcohol cravings, leading to heavier drinking. For instance, a person consuming 4–5 standard alcoholic drinks (14 grams of pure alcohol each) while using cocaine may inadvertently double their risk of pancreatic damage. The liver metabolizes both substances, producing toxic byproducts like acetaldehyde from alcohol and cocaethylene from cocaine and alcohol. Cocaethylene, in particular, is more toxic than cocaine itself and prolongs the drug’s effects, further straining the pancreas. This metabolic overload can trigger oxidative stress, damaging pancreatic cells and impairing their ability to regulate insulin and digest food.
Practical precautions are essential for harm reduction. If you or someone you know uses these substances, limit alcohol intake to 1–2 drinks per day (if at all) and avoid binge drinking, defined as 4 drinks for women or 5 for men within 2 hours. Stay hydrated, as dehydration from alcohol and cocaine use can worsen pancreatic stress. Monitor for early signs of pancreatitis, such as severe abdominal pain, nausea, or fever, and seek medical attention immediately if symptoms arise. For those in recovery, combining therapy with medications like naltrexone (for alcohol) or contingency management (for cocaine) can reduce relapse risk and protect pancreatic health.
Comparatively, the combined effects of alcohol and cocaine on the pancreas are more severe than those of either substance alone. While alcohol-induced pancreatitis typically requires chronic heavy drinking (e.g., 5+ drinks daily for years), cocaine can trigger acute pancreatitis even in first-time users. When used together, the threshold for damage drops significantly. For example, a 30-year-old occasional cocaine user who drinks moderately may still face pancreatic issues due to the synergistic toxicity. This highlights the need for targeted education, especially among younger adults, who often underestimate the risks of polydrug use.
In conclusion, the combined effects of alcohol and cocaine on the pancreas are a critical public health concern. Their interaction exacerbates inflammation, reduces blood flow, and produces harmful metabolites, increasing the likelihood of acute pancreatitis and long-term damage. By understanding these risks and adopting harm reduction strategies, individuals can mitigate the dangers of this dangerous combination. Awareness, moderation, and early intervention are key to protecting pancreatic health in the face of these potent substances.
Does God Forbid Alcohol? Exploring Biblical Views on Drinking
You may want to see also
Frequently asked questions
Yes, excessive alcohol consumption can lead to pancreatitis, an inflammation of the pancreas. Chronic alcohol use is a major risk factor for both acute and chronic pancreatitis, which can cause severe abdominal pain, digestive issues, and long-term damage to the pancreas.
Yes, cocaine use can harm the pancreas by causing vasoconstriction (narrowing of blood vessels), which reduces blood flow to the organ. This can lead to ischemia (lack of oxygen) and potentially result in acute pancreatitis, a serious and painful condition.
While alcohol and cocaine are not direct causes of pancreatic cancer, chronic alcohol abuse and cocaine use can increase the risk of pancreatitis, which is a known risk factor for pancreatic cancer. Both substances also weaken overall health, potentially contributing to cancer development indirectly.
Quitting alcohol and cocaine can prevent further damage to the pancreas and reduce the risk of complications like pancreatitis. However, the extent of reversibility depends on the severity of the damage. Early cessation improves the chances of recovery, but chronic or severe damage may have lasting effects.