Alcohol consumption has been widely studied for its effects on various organ systems, including the kidneys. Nephrosis, a condition characterized by significant proteinuria, edema, and hypoalbuminemia, is often associated with kidney damage. While chronic alcohol use is known to contribute to kidney dysfunction through mechanisms such as dehydration, electrolyte imbalances, and direct toxicity to renal cells, its role in inducing nephrosis specifically remains a topic of debate. Research suggests that excessive alcohol intake may exacerbate underlying kidney conditions or interact with other risk factors, potentially leading to nephrotic syndrome. However, the direct causative link between alcohol and nephrosis is not yet fully established, necessitating further investigation to clarify the relationship and its clinical implications.
| Characteristics | Values |
|---|---|
| Definition | Nephrosis refers to a condition characterized by significant proteinuria, hypoalbuminemia, and edema, often associated with kidney damage. |
| Alcohol and Nephrosis | Chronic heavy alcohol consumption is associated with an increased risk of developing nephrosis. |
| Mechanism | Alcohol can induce nephrosis through direct toxicity to kidney cells, oxidative stress, inflammation, and disruption of the glomerular filtration barrier. |
| Risk Factors | Prolonged heavy drinking, malnutrition (common in alcoholics), and concurrent liver disease (e.g., alcoholic liver disease) exacerbate the risk. |
| Symptoms | Edema (swelling), proteinuria (excess protein in urine), hypoalbuminemia (low blood albumin), fatigue, and foamy urine. |
| Diagnosis | Urine tests for proteinuria, blood tests for albumin levels, kidney function tests (e.g., creatinine, eGFR), and sometimes kidney biopsy. |
| Treatment | Abstinence from alcohol, dietary modifications (low protein, low sodium), diuretics, and management of underlying conditions (e.g., liver disease). |
| Prognosis | Reversible in early stages with alcohol cessation and proper treatment; chronic alcohol-induced nephrosis may lead to irreversible kidney damage or failure. |
| Prevention | Moderate alcohol consumption, balanced diet, and regular health check-ups to monitor kidney function. |
| Latest Research | Studies highlight the role of alcohol-induced mitochondrial dysfunction and apoptosis in kidney cells as key mechanisms in nephrosis development. |
Explore related products






What You'll Learn
![]()
Alcohol's direct kidney toxicity
Excessive alcohol consumption can directly damage the kidneys, leading to a condition known as alcoholic nephropathy. This occurs when the toxic byproducts of alcohol metabolism accumulate, causing inflammation and oxidative stress in renal tissues. Unlike other forms of kidney damage, alcoholic nephropathy is primarily driven by the direct toxicity of alcohol and its metabolites, rather than secondary effects like hypertension or dehydration. Studies show that heavy drinking, defined as more than 4 drinks per day for men and 3 for women, significantly increases the risk of developing this condition.
To understand the mechanism, consider how alcohol metabolism generates acetaldehyde and free radicals, which impair kidney function. Acetaldehyde, a highly reactive compound, disrupts cellular membranes and reduces the kidneys’ ability to filter waste. Simultaneously, free radicals deplete antioxidants, exacerbating tissue damage. Chronic exposure to these toxins can lead to fibrosis, where scar tissue replaces healthy kidney cells, progressively reducing organ function. This process is often irreversible, making early intervention critical.
Practical steps to mitigate alcohol-induced kidney toxicity include moderating intake and staying hydrated. Limiting alcohol to recommended guidelines—up to 2 drinks per day for men and 1 for women—can reduce the risk. Pairing alcohol with water helps flush toxins from the kidneys, minimizing damage. For those with pre-existing kidney conditions or a family history of renal disease, complete abstinence may be advisable. Regular kidney function tests, such as serum creatinine and urine albumin levels, can detect early signs of damage in at-risk individuals.
Comparatively, alcohol’s direct kidney toxicity differs from other causes like diabetes or high blood pressure, which indirectly harm the kidneys through systemic effects. Alcohol’s impact is more localized, targeting the renal tubules and glomeruli directly. This distinction highlights the need for targeted interventions, such as antioxidant therapy or medications that reduce acetaldehyde production. However, such treatments remain experimental, emphasizing the importance of prevention through lifestyle changes.
In conclusion, alcohol’s direct kidney toxicity is a preventable yet underrecognized threat. By understanding the mechanisms and adopting practical strategies, individuals can protect their renal health. Moderation, hydration, and regular monitoring are key to avoiding the irreversible damage of alcoholic nephropathy. For heavy drinkers, reducing intake or seeking professional help can be life-saving steps toward preserving kidney function.
Eggnog Safety: Why Refrigeration Matters for Alcoholic Eggnog
You may want to see also
Explore related products






![]()
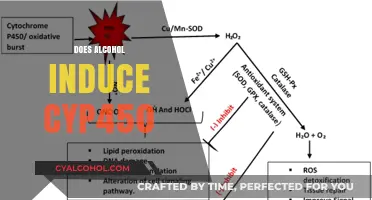
Role of oxidative stress in nephrosis
Alcohol consumption, particularly chronic and excessive intake, has been linked to kidney damage, with oxidative stress emerging as a key player in this process. Oxidative stress occurs when there is an imbalance between the production of reactive oxygen species (ROS) and the body's antioxidant defense mechanisms. In the context of alcohol-induced nephrosis, this imbalance can lead to cellular damage, inflammation, and ultimately, kidney dysfunction.
Consider the mechanism: when alcohol is metabolized, it generates ROS, including superoxide anions, hydrogen peroxide, and hydroxyl radicals. These highly reactive molecules can damage cellular components such as lipids, proteins, and DNA, particularly in the kidney's proximal tubules, which are highly susceptible to oxidative injury. For instance, a study published in the *Journal of Renal Nutrition* found that chronic alcohol consumption in rats led to a significant increase in lipid peroxidation and a decrease in antioxidant enzyme activities, such as superoxide dismutase (SOD) and glutathione peroxidase (GPx), in renal tissues. This suggests that alcohol exacerbates oxidative stress by both increasing ROS production and impairing the body's natural antioxidant defenses.
To mitigate the risk of alcohol-induced nephrosis, practical steps can be taken. Limiting alcohol intake to moderate levels—defined as up to one drink per day for women and up to two drinks per day for men—can reduce oxidative stress and kidney damage. Additionally, incorporating antioxidants into the diet, such as vitamins C and E, selenium, and polyphenols found in fruits and vegetables, can help neutralize ROS and protect renal cells. For example, a clinical trial in *Alcoholism: Clinical and Experimental Research* demonstrated that supplementation with vitamin E significantly reduced markers of oxidative stress in heavy drinkers. However, it’s crucial to avoid excessive supplementation, as high doses of antioxidants can have adverse effects.
Comparatively, the role of oxidative stress in nephrosis is not unique to alcohol consumption; other conditions like diabetes and hypertension also contribute to ROS-mediated kidney damage. However, alcohol’s direct metabolic effects and its ability to impair antioxidant systems make it a distinct risk factor. For individuals with pre-existing kidney conditions or those in older age categories (over 60), even moderate alcohol consumption may exacerbate oxidative stress and accelerate nephrosis. Regular monitoring of kidney function, such as serum creatinine and urine albumin levels, is advisable for heavy drinkers or those at risk.
In conclusion, oxidative stress is a critical mediator of alcohol-induced nephrosis, driven by increased ROS production and compromised antioxidant defenses. By understanding this mechanism, individuals can take proactive steps to reduce their risk, such as moderating alcohol intake and enhancing dietary antioxidants. For those with existing kidney vulnerabilities, avoiding alcohol altogether may be the safest approach. This targeted focus on oxidative stress not only highlights the dangers of excessive drinking but also provides actionable strategies for kidney health preservation.
Alcohol and Cancer Risk: Uncovering Hidden Carcinogens in Your Drink
You may want to see also
Explore related products






![]()
Impact on glomerular filtration rate
Excessive alcohol consumption can disrupt the glomerular filtration rate (GFR), a key marker of kidney function. Studies show that acute alcohol intake, particularly in binge-drinking scenarios (defined as 4-5 drinks within 2 hours for most adults), can lead to a transient increase in GFR. This initial spike, however, is followed by a compensatory decrease, potentially straining the kidneys. Chronic alcohol use, especially at levels exceeding 40 grams of ethanol daily (roughly 3-4 standard drinks), has been associated with sustained reductions in GFR, signaling progressive renal impairment.
Consider the mechanism: alcohol-induced vasodilation and increased renal blood flow initially elevate GFR, but prolonged exposure leads to oxidative stress and inflammation, damaging the glomeruli. For instance, a 2018 study in *Alcoholism: Clinical and Experimental Research* found that heavy drinkers (averaging 6 drinks/day) exhibited a 15-20% lower GFR compared to moderate drinkers (1 drink/day). Age compounds this risk; individuals over 50 with a history of heavy drinking are particularly vulnerable due to age-related declines in kidney function.
To mitigate risks, limit alcohol intake to recommended guidelines: up to 1 drink/day for women and 2 drinks/day for men. Hydration is critical; alternating alcoholic beverages with water can reduce the concentration of toxins reaching the kidneys. Regular monitoring of GFR through blood tests is advisable for those with a history of heavy drinking, especially if accompanied by symptoms like swelling, fatigue, or changes in urination. Early intervention, such as reducing alcohol consumption or adopting a low-sodium diet, can prevent irreversible damage.
Comparatively, while moderate drinking may have minimal impact on GFR, the threshold for harm is lower than often assumed. For example, a 2020 meta-analysis in *The Lancet* suggested that even 2-3 drinks/day could accelerate GFR decline in predisposed individuals, such as those with hypertension or diabetes. This underscores the importance of individualized risk assessment, particularly for older adults or those with comorbidities.
In conclusion, alcohol’s impact on GFR is dose-dependent and cumulative. While occasional moderate drinking may pose little risk, chronic or excessive consumption can lead to significant renal dysfunction. Practical steps, such as adhering to intake limits, staying hydrated, and regular health screenings, are essential for preserving kidney health in the face of alcohol exposure.
Prohibition of Alcohol: A Social Movement or Political Strategy?
You may want to see also
Explore related products






![]()
Alcohol-induced hypertension and kidneys
Chronic alcohol consumption is a known risk factor for hypertension, a condition that significantly impacts kidney health. The relationship between alcohol-induced hypertension and kidney damage is a critical aspect of understanding how alcohol can lead to nephrosis. When blood pressure remains elevated due to excessive drinking, the kidneys, which are highly vascular organs, bear the brunt of this stress. Over time, the constant pressure can damage the delicate glomeruli—the tiny filters in the kidneys—leading to proteinuria, a hallmark of nephrotic syndrome. Studies indicate that heavy drinking, defined as more than 14 drinks per week for men and 7 for women, accelerates this process, particularly in individuals over 40 whose vascular systems are less resilient.
Consider the mechanism: alcohol disrupts the renin-angiotensin-aldosterone system (RAAS), a key regulator of blood pressure and fluid balance. Excessive alcohol intake increases renin secretion, leading to higher angiotensin II levels, which constrict blood vessels and elevate blood pressure. Simultaneously, alcohol impairs the kidneys’ ability to excrete sodium, further exacerbating hypertension. This dual assault on the kidneys not only damages their filtration units but also reduces their overall function, setting the stage for nephrosis. For those with pre-existing kidney conditions, even moderate drinking (up to 7 drinks per week for women and 14 for men) can worsen outcomes, underscoring the need for strict moderation or abstinence.
Practical steps to mitigate alcohol-induced hypertension and protect kidney health include monitoring blood pressure regularly, especially if you consume alcohol frequently. Limiting daily intake to one drink for women and two for men, as per dietary guidelines, can significantly reduce risk. Incorporating potassium-rich foods like bananas, spinach, and sweet potatoes can help counteract sodium retention, though individuals with advanced kidney disease should consult a dietitian to avoid hyperkalemia. Additionally, staying hydrated with water rather than alcohol aids in flushing toxins and reducing vascular strain. For heavy drinkers, gradual reduction under medical supervision is advised to avoid withdrawal complications that could further stress the kidneys.
Comparatively, while alcohol’s direct toxicity to kidney cells is less understood than its hypertensive effects, the indirect damage via hypertension remains a primary concern. Unlike acute kidney injury from binge drinking, which may be reversible, chronic hypertension from sustained alcohol use often leads to irreversible nephrosclerosis—a fibrosis of kidney tissue. This distinction highlights why managing blood pressure is paramount for kidney preservation in drinkers. Medications like ACE inhibitors or ARBs, which target the RAAS system, are often prescribed to hypertensive drinkers, but their efficacy is diminished if alcohol consumption continues unchecked.
In conclusion, alcohol-induced hypertension is a preventable yet underrecognized driver of kidney damage. By understanding the interplay between alcohol, blood pressure, and kidney function, individuals can take proactive steps to safeguard their renal health. Whether through dietary adjustments, lifestyle modifications, or medical intervention, addressing hypertension in the context of alcohol consumption is essential to preventing nephrosis and its complications. For those struggling with alcohol dependency, seeking support from healthcare professionals or addiction specialists is a critical step toward protecting both cardiovascular and renal health.
Does Gojo Drink Alcohol? Exploring the Truth Behind the Rumors
You may want to see also
Explore related products






![]()
Link between cirrhosis and nephrosis
Alcohol consumption, particularly in excess, is a well-documented risk factor for cirrhosis, a chronic liver disease characterized by the replacement of healthy liver tissue with scar tissue. However, the relationship between alcohol-induced cirrhosis and nephrosis—a kidney disorder marked by proteinuria and edema—is less straightforward but equally critical. Nephrosis can develop as a complication of cirrhosis, a condition often referred to as hepatorenal syndrome (HRS). This syndrome highlights the intricate interplay between liver and kidney function, where severe liver damage disrupts systemic circulation, leading to reduced renal blood flow and subsequent kidney dysfunction. Understanding this link is essential for clinicians and patients alike, as early detection and management can mitigate the progression of both conditions.
From an analytical perspective, the pathophysiology of hepatorenal syndrome provides insight into how cirrhosis precipitates nephrosis. In cirrhosis, portal hypertension and splanchnic vasodilation trigger systemic vasodilation, activating compensatory mechanisms such as the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system. Over time, these mechanisms lead to renal vasoconstriction, reducing glomerular filtration rate (GFR) and causing sodium and water retention. This cascade results in oliguria, azotemia, and edema—hallmarks of nephrosis. Notably, HRS is categorized into two types: Type 1, characterized by rapid kidney function decline, and Type 2, marked by more gradual deterioration. Both types underscore the severity of liver-kidney interaction in cirrhosis patients, particularly those with advanced disease or refractory ascites.
For individuals at risk, practical steps can be taken to monitor and prevent the progression from cirrhosis to nephrosis. Regular assessment of renal function, including serum creatinine and urine protein levels, is crucial for cirrhosis patients, especially those with a history of heavy alcohol use. Limiting alcohol intake to recommended guidelines—up to one drink per day for women and two for men—can reduce the risk of cirrhosis and its complications. Additionally, managing comorbid conditions such as hypertension and diabetes is essential, as these can exacerbate renal stress in cirrhosis patients. Diuretic therapy, often used to manage ascites, must be carefully titrated to avoid precipitating HRS, particularly in patients with low GFR.
A comparative analysis of treatment strategies reveals the challenges in managing hepatorenal syndrome. While Type 1 HRS often requires urgent interventions such as vasoconstrictor therapy (e.g., terlipressin) combined with albumin, Type 2 HRS may respond to volume expansion and diuretic adjustments. In severe cases, liver transplantation remains the definitive treatment, offering potential reversal of both cirrhosis and associated nephrosis. However, the scarcity of donor organs and the complexity of transplantation underscore the importance of preventive measures. Notably, emerging therapies like aquaporin modulators and renal replacement therapies are being explored, though their efficacy in alcohol-induced cirrhosis remains under investigation.
In conclusion, the link between cirrhosis and nephrosis is a critical consideration in the management of alcohol-related liver disease. By recognizing the mechanisms driving hepatorenal syndrome and implementing targeted interventions, healthcare providers can improve outcomes for at-risk patients. For individuals, moderation in alcohol consumption and proactive monitoring of liver and kidney health are key to preventing this devastating complication. The interplay between these organs serves as a reminder of the systemic impact of alcohol abuse and the need for holistic approaches to treatment.
Social Factors Leading to Alcoholism
You may want to see also
Frequently asked questions
Alcohol itself does not directly cause nephrosis, but chronic heavy drinking can lead to kidney damage, including conditions like alcoholic nephropathy, which may resemble nephrosis.
Moderate alcohol consumption is generally not associated with nephrosis. However, individual susceptibility and underlying kidney conditions may increase risk, so moderation is key.
Alcohol can exacerbate kidney damage, potentially leading to nephrotic syndrome in individuals with pre-existing kidney issues or those who consume alcohol excessively over time.
Alcohol-related kidney damage, such as alcoholic nephropathy, involves direct harm to the kidneys due to alcohol toxicity, whereas nephrosis is a broader term for kidney damage characterized by proteinuria, edema, and hypoalbuminemia, which can have multiple causes.