Alcohol consumption is known to interfere with the body's ability to absorb and utilize essential nutrients, including thiamine (vitamin B1), a critical vitamin for energy metabolism and proper nervous system function. Chronic alcohol use can lead to thiamine deficiency, as alcohol impairs its absorption in the gastrointestinal tract and disrupts its storage and activation in the liver. This depletion is particularly concerning because thiamine deficiency can result in severe health conditions such as Wernicke-Korsakoff syndrome, a neurological disorder characterized by confusion, memory loss, and coordination problems. Understanding the relationship between alcohol and thiamine is crucial for addressing the nutritional risks associated with excessive drinking and preventing related complications.
| Characteristics | Values |
|---|---|
| Does alcohol deplete thiamine? | Yes, chronic alcohol consumption is strongly associated with thiamine deficiency. |
| Mechanism of depletion | 1. Impaired absorption: Alcohol interferes with thiamine uptake in the intestines. 2. Reduced storage: Alcohol decreases thiamine storage in the liver. 3. Increased excretion: Alcohol increases thiamine loss through urine. 4. Interference with activation: Alcohol disrupts the conversion of thiamine to its active form (thiamine pyrophosphate). |
| Populations at risk | Chronic alcohol users, especially those with poor nutrition or liver disease. |
| Consequences of thiamine deficiency | Wernicke-Korsakoff syndrome (WKS), beriberi, neurological damage, cardiovascular issues, and weakened immune function. |
| Prevention and treatment | Thiamine supplementation, improved nutrition, and alcohol cessation are key interventions. |
| Recommended thiamine intake for alcohol users | Higher than the general population; consult a healthcare provider for personalized advice. |
| Latest research findings | Studies continue to emphasize the critical link between alcohol use and thiamine deficiency, highlighting the need for early intervention in at-risk populations. |
Explore related products






What You'll Learn
- Thiamine Absorption Inhibition: Alcohol disrupts stomach lining, reducing thiamine absorption in the intestines
- Increased Excretion: Alcohol accelerates thiamine loss through urine, depleting body stores faster
- Liver Function Impact: Chronic alcohol use damages liver, impairing thiamine storage and release
- Poor Diet Connection: Alcoholics often have nutrient-deficient diets, worsening thiamine depletion risk
- Wernicke-Korsakoff Syndrome: Severe thiamine deficiency from alcohol causes brain disorders like Wernicke-Korsakoff
![]()
Thiamine Absorption Inhibition: Alcohol disrupts stomach lining, reducing thiamine absorption in the intestines
Alcohol's impact on the body extends beyond its immediate effects, particularly when it comes to nutrient absorption. One critical yet often overlooked consequence is its disruption of the stomach lining, which plays a pivotal role in thiamine (vitamin B1) absorption. The stomach lining, or mucosa, is essential for initiating the breakdown of nutrients, including thiamine, before they move to the intestines for further absorption. Chronic alcohol consumption damages this delicate lining, impairing its ability to function effectively. This damage reduces the bioavailability of thiamine, even if dietary intake remains adequate, setting the stage for deficiencies that can have far-reaching health implications.
The mechanism behind this inhibition is both complex and insidious. Alcohol irritates the stomach lining, leading to inflammation and, in severe cases, gastritis or ulcers. This inflammation hampers the secretion of hydrochloric acid and digestive enzymes, both of which are crucial for liberating thiamine from food. Additionally, alcohol interferes with the transport proteins responsible for carrying thiamine across the intestinal wall. Studies show that individuals who consume more than 60 grams of alcohol daily (roughly 4-5 standard drinks) are at significantly higher risk of thiamine deficiency due to these absorption issues. For context, a standard drink is equivalent to 14 grams of pure alcohol, such as a 12-ounce beer, 5-ounce glass of wine, or 1.5-ounce shot of distilled spirits.
The consequences of thiamine deficiency are severe, particularly for heavy drinkers. Thiamine is vital for energy metabolism and proper nerve function. Its depletion can lead to conditions like Wernicke-Korsakoff syndrome, a neurological disorder characterized by confusion, memory loss, and coordination problems. Early symptoms of deficiency include fatigue, irritability, and muscle weakness, which are often mistaken for the effects of alcohol itself. This misdiagnosis can delay treatment, exacerbating the condition. For those at risk, practical steps include limiting alcohol intake, consuming thiamine-rich foods (such as whole grains, legumes, and nuts), and considering supplementation under medical supervision.
Comparatively, non-drinkers or moderate drinkers typically absorb 90-95% of dietary thiamine in the small intestine, while heavy drinkers may absorb as little as 50-70%. This disparity underscores the need for targeted interventions. For instance, individuals with alcohol use disorder should aim for a daily thiamine intake of 1.2 mg (the recommended dietary allowance for adults) but may require higher doses to compensate for absorption issues. Healthcare providers often recommend 50-100 mg of thiamine daily for those at risk, administered orally or via injection in severe cases. Pairing thiamine supplementation with a balanced diet and reduced alcohol consumption can mitigate the risk of deficiency and its associated complications.
In summary, alcohol’s disruption of the stomach lining creates a cascade of events that inhibit thiamine absorption, even when dietary intake is sufficient. This inhibition is not merely a side effect but a direct consequence of alcohol’s toxic impact on the gastrointestinal tract. Recognizing the signs of thiamine deficiency and taking proactive steps—such as moderating alcohol intake, prioritizing nutrient-rich foods, and seeking medical advice—can prevent long-term health issues. For those struggling with alcohol use, addressing both the habit and its nutritional consequences is essential for recovery and overall well-being.
Convenient Alcohol Delivery: Exploring Services That Bring Drinks to Your Door
You may want to see also
Explore related products






![]()
Increased Excretion: Alcohol accelerates thiamine loss through urine, depleting body stores faster
Alcohol consumption triggers a cascade of events that significantly impact thiamine levels in the body, with increased urinary excretion playing a pivotal role. Research indicates that alcohol interferes with the kidneys' ability to reabsorb thiamine, leading to its excessive loss through urine. This process is particularly concerning because thiamine, also known as vitamin B1, is a water-soluble vitamin that the body cannot store in large amounts. As a result, regular alcohol intake can rapidly deplete thiamine reserves, leaving individuals vulnerable to deficiencies. For instance, studies have shown that chronic alcohol users may excrete up to 50% more thiamine in their urine compared to non-drinkers, highlighting the direct correlation between alcohol consumption and accelerated thiamine loss.
Understanding the mechanism behind this increased excretion is crucial for addressing the issue effectively. When alcohol is metabolized, it produces compounds that disrupt the normal functioning of the kidneys, impairing their ability to retain essential nutrients like thiamine. This disruption is exacerbated by the diuretic effect of alcohol, which increases urine production and further contributes to nutrient loss. For individuals who consume alcohol regularly, especially in moderate to high amounts (defined as more than 14 drinks per week for men and 7 for women), this process can lead to a chronic thiamine deficiency over time. Such deficiencies are not only detrimental to overall health but also particularly harmful to the nervous system, cardiovascular function, and energy metabolism.
Practical steps can be taken to mitigate the risk of thiamine depletion caused by increased urinary excretion. First, moderating alcohol intake is the most direct approach. Reducing consumption to within recommended limits can significantly decrease the burden on the kidneys and slow the rate of thiamine loss. Second, incorporating thiamine-rich foods into the diet, such as whole grains, legumes, and lean meats, can help replenish depleted stores. For those at higher risk, such as heavy drinkers or individuals with pre-existing nutritional deficiencies, supplementation may be necessary. A daily dose of 50–100 mg of thiamine, as recommended by healthcare professionals, can help maintain adequate levels. However, it’s essential to consult a doctor before starting any supplementation regimen, as individual needs may vary.
Comparatively, the impact of alcohol on thiamine excretion is more pronounced in certain demographics, such as older adults and individuals with compromised kidney function. Aging kidneys are less efficient at retaining nutrients, making older drinkers particularly susceptible to thiamine loss. Similarly, those with pre-existing kidney conditions may experience exacerbated effects due to alcohol’s interference with renal function. In these cases, proactive measures, including regular health check-ups and tailored dietary adjustments, are critical. For example, older adults might benefit from reducing alcohol intake to fewer than 7 drinks per week, while also focusing on thiamine-rich foods to counteract increased excretion.
In conclusion, alcohol’s role in accelerating thiamine loss through urine is a significant yet often overlooked consequence of regular consumption. By understanding the mechanisms at play and taking targeted steps to mitigate this effect, individuals can better protect their thiamine levels and overall health. Whether through moderation, dietary adjustments, or supplementation, addressing this issue requires a proactive and informed approach. For those concerned about their thiamine status, monitoring alcohol intake and prioritizing nutrient-rich foods are simple yet effective strategies to combat the detrimental effects of increased excretion.
Exploring the Chemistry of Nitroalkanes and B-Nitro Alcohols
You may want to see also
Explore related products






![]()
Liver Function Impact: Chronic alcohol use damages liver, impairing thiamine storage and release
Chronic alcohol consumption wreaks havoc on the liver, a vital organ responsible for storing and releasing thiamine, a critical B vitamin. This damage disrupts the liver's ability to manage thiamine levels effectively, leading to a cascade of health issues. Studies show that up to 80% of individuals with alcohol use disorder (AUD) suffer from thiamine deficiency, often due to liver dysfunction. The liver normally stores about 30-50 mg of thiamine, enough to sustain the body for 18 days under normal conditions. However, prolonged alcohol intake reduces this reserve, as the liver prioritizes metabolizing alcohol over its other functions, including thiamine storage and release.
The mechanism behind this impairment is twofold. First, alcohol-induced liver damage, such as fatty liver disease or cirrhosis, compromises the organ's structural integrity. Second, alcohol interferes with the transport proteins responsible for moving thiamine from the liver to the bloodstream. For instance, the high-affinity thiamine transporter 2 (THTR2) is downregulated in the presence of alcohol, limiting the body's access to this essential nutrient. This dual assault on liver function exacerbates thiamine deficiency, which can manifest as symptoms like fatigue, confusion, and, in severe cases, Wernicke-Korsakoff syndrome—a neurological disorder linked to thiamine depletion.
To mitigate these risks, individuals with chronic alcohol use should adopt a two-pronged approach. First, reducing alcohol intake is paramount. Even cutting back from heavy drinking (defined as >14 drinks/week for men and >7 for women) to moderate levels can improve liver function and thiamine metabolism. Second, supplementing with thiamine can help restore depleted levels. The recommended daily allowance (RDA) for thiamine is 1.2 mg for men and 1.1 mg for women, but those with AUD may require higher doses, up to 50-100 mg daily under medical supervision. Pairing thiamine supplements with vitamin B-complex ensures synergistic absorption and utilization.
A comparative analysis highlights the stark difference between individuals with and without AUD. Non-drinkers typically maintain stable thiamine levels through a balanced diet, as the liver efficiently stores and releases the vitamin as needed. In contrast, chronic drinkers face a vicious cycle: alcohol damages the liver, reducing thiamine storage capacity, while simultaneously increasing thiamine excretion through urine. This double jeopardy underscores the urgency of addressing both alcohol consumption and nutritional deficiencies in at-risk populations.
Practically, incorporating thiamine-rich foods like whole grains, legumes, and lean pork can complement supplementation efforts. However, dietary changes alone may not suffice for those with severe liver damage. Regular liver function tests and monitoring of thiamine levels are essential for early intervention. For example, a serum thiamine level below 20 nmol/L indicates deficiency, warranting immediate action. By understanding the liver's role in thiamine management and the impact of alcohol, individuals can take proactive steps to safeguard their health and prevent long-term complications.
Confronting a Loved One's Alcohol Problem: A Guide
You may want to see also
Explore related products






![]()
Poor Diet Connection: Alcoholics often have nutrient-deficient diets, worsening thiamine depletion risk
Alcohol consumption, particularly in excess, is a known contributor to thiamine (vitamin B1) deficiency, a condition that can lead to serious health issues such as Wernicke-Korsakoff syndrome. However, the relationship between alcohol and thiamine depletion is not solely due to the direct effects of ethanol on the body. A critical yet often overlooked factor is the poor dietary habits commonly associated with alcoholism, which exacerbate the risk of thiamine deficiency. Alcoholics frequently consume diets low in essential nutrients, including thiamine, due to irregular eating patterns, limited food variety, and a preference for calorie-dense but nutrient-poor foods. This dietary inadequacy compounds the thiamine depletion caused by alcohol’s interference with absorption, metabolism, and storage of the vitamin.
Consider the typical diet of someone struggling with alcoholism: high in processed foods, sugary snacks, and fast food, but low in whole grains, lean proteins, and fresh fruits and vegetables—all of which are rich sources of thiamine. For instance, a diet lacking in thiamine-dense foods like pork, sunflower seeds, or fortified cereals can leave an individual with a daily intake far below the recommended dietary allowance (RDA) of 1.1 mg for women and 1.2 mg for men. When alcohol is introduced, it further diminishes thiamine levels by impairing intestinal absorption and increasing urinary excretion, creating a double-edged sword for depletion. Chronic alcohol use also damages the gastrointestinal tract, reducing the body’s ability to absorb nutrients, even if thiamine-rich foods are consumed.
The consequences of this nutrient-deficient diet are particularly severe for heavy drinkers, who often prioritize alcohol over food, sometimes skipping meals entirely. Studies show that up to 80% of alcoholics have thiamine deficiency, with symptoms ranging from fatigue and confusion to more severe neurological impairments. For example, Wernicke’s encephalopathy, characterized by confusion, ataxia, and ophthalmoplegia, is a direct result of thiamine deficiency and is often seen in alcoholics with poor dietary habits. Without intervention, this can progress to Korsakoff syndrome, a chronic condition marked by memory loss and confabulation. Addressing thiamine depletion in alcoholics, therefore, requires not only reducing alcohol intake but also improving dietary quality.
Practical steps to mitigate thiamine depletion in alcoholics include incorporating thiamine-rich foods into daily meals, such as whole grains, legumes, and nuts. For those with severe deficiency, supplementation may be necessary, with doses ranging from 50 to 100 mg daily under medical supervision. Additionally, alcoholics should focus on reestablishing regular eating patterns, ensuring meals are balanced and nutrient-dense. For caregivers or healthcare providers, educating patients about the importance of diet in thiamine maintenance can be a powerful tool in preventing deficiency-related complications. While abstaining from alcohol is the most effective way to halt thiamine depletion, improving dietary habits is a critical complementary strategy that cannot be overlooked.
In comparison to non-alcoholics, who can typically meet their thiamine needs through a varied diet, alcoholics face unique challenges that require targeted interventions. The interplay between alcohol’s physiological effects and poor dietary choices creates a vicious cycle that accelerates thiamine depletion. Breaking this cycle demands a holistic approach, addressing both alcohol consumption and nutritional deficiencies. By focusing on diet as a modifiable risk factor, individuals and healthcare providers can take proactive steps to reduce the risk of thiamine deficiency and its associated health complications. Ultimately, recognizing the poor diet connection in alcoholism is essential for developing effective strategies to combat thiamine depletion and improve overall health outcomes.
Preserving Snakes: Alcohol Immersion Techniques at the Smithsonian
You may want to see also
Explore related products





![]()
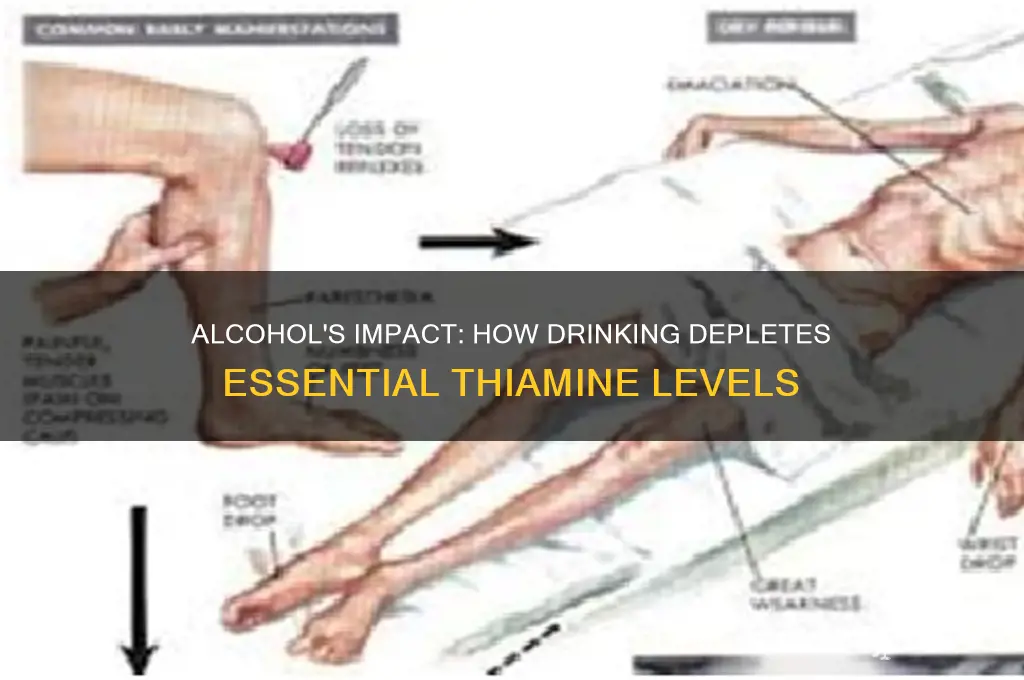
Wernicke-Korsakoff Syndrome: Severe thiamine deficiency from alcohol causes brain disorders like Wernicke-Korsakoff
Chronic alcohol consumption disrupts thiamine absorption and utilization, setting the stage for Wernicke-Korsakoff Syndrome (WKS), a devastating neurological disorder. Alcohol interferes with the active transport of thiamine in the intestines, reduces its activation to its biologically active form (thiamine pyrophosphate), and impairs its storage in the liver. This triple threat leads to a severe deficiency, particularly in heavy drinkers who often have poor diets lacking thiamine-rich foods like whole grains, legumes, and nuts.
WKS manifests in two distinct but interconnected phases. Wernicke’s encephalopathy, the acute phase, presents with a classic triad: confusion, ataxia (unsteady gait), and ophthalmoplegia (paralysis of eye muscles). Left untreated, it progresses to Korsakoff’s psychosis, characterized by severe memory impairment, confabulation (fabricating memories), and disorientation. This chronic phase often results in permanent brain damage, highlighting the urgency of early intervention.
Diagnosis relies on clinical suspicion, as laboratory tests for thiamine deficiency are unreliable. Any individual with a history of chronic alcohol use presenting with neurological symptoms should raise red flags. Treatment is straightforward but time-sensitive: immediate administration of high-dose thiamine, typically 500 mg intravenously or intramuscularly daily for 3-5 days, followed by oral supplementation. Concurrent management of alcohol withdrawal and nutritional support are crucial for optimal outcomes.
Preventing WKS hinges on addressing the root cause: alcohol misuse. However, for those struggling with addiction, ensuring adequate thiamine intake through diet or supplementation is vital. Fortified foods, thiamine-rich meals, and multivitamins can help bridge the gap. Early recognition of WKS symptoms and prompt treatment can prevent irreversible brain damage, emphasizing the need for increased awareness among healthcare professionals and individuals at risk.
Alcohol Edu: UArk's Mandatory Course?
You may want to see also
Frequently asked questions
Yes, chronic alcohol consumption can lead to thiamine depletion due to poor dietary intake, impaired absorption, and increased excretion.
Alcohol damages the lining of the stomach and intestines, reducing the body’s ability to absorb thiamine from food.
Symptoms include fatigue, confusion, muscle weakness, and in severe cases, Wernicke-Korsakoff syndrome, a neurological disorder.
While moderate drinking is less likely to cause thiamine depletion, chronic even moderate consumption can still impact thiamine levels over time.
Prevention includes reducing alcohol intake, eating a thiamine-rich diet (e.g., whole grains, nuts, legumes), and considering thiamine supplements under medical guidance.