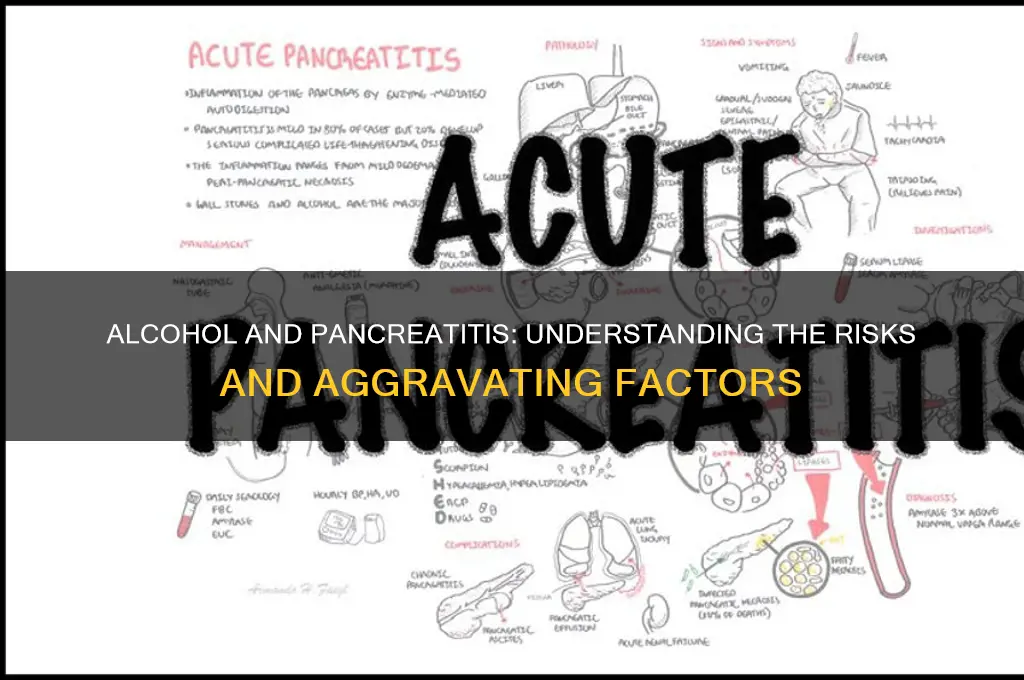
Alcohol consumption is a well-established risk factor for pancreatitis, a condition characterized by inflammation of the pancreas. Chronic and heavy alcohol use can directly damage pancreatic cells, leading to both acute and chronic forms of the disease. While acute pancreatitis can occur after a single episode of excessive drinking, chronic pancreatitis often develops in individuals with long-term alcohol abuse. The mechanism involves alcohol-induced metabolic changes, activation of digestive enzymes within the pancreas, and increased permeability of the pancreatic ducts, all of which contribute to inflammation and tissue damage. Therefore, alcohol not only increases the risk of developing pancreatitis but can also exacerbate existing pancreatic conditions, making it a critical factor to address in the management and prevention of the disease.
| Characteristics | Values |
|---|---|
| Direct Toxicity | Alcohol (ethanol) and its metabolite acetaldehyde directly damage pancreatic acinar cells, leading to inflammation and cell death. |
| Oxidative Stress | Chronic alcohol consumption increases oxidative stress in the pancreas, exacerbating inflammation and tissue damage. |
| Activation of Digestive Enzymes | Alcohol disrupts the normal function of pancreatic enzymes, causing premature activation within the pancreas, leading to autodigestion. |
| Increased Permeability | Alcohol weakens the pancreatic duct lining, allowing enzymes to leak into surrounding tissues and trigger inflammation. |
| Impaired Autophagy | Alcohol interferes with the pancreas's ability to clear damaged cellular components, contributing to inflammation and cell injury. |
| Risk of Acute Pancreatitis | Heavy alcohol use is a leading cause of acute pancreatitis, with a dose-dependent relationship. |
| Risk of Chronic Pancreatitis | Long-term alcohol abuse significantly increases the risk of developing chronic pancreatitis, a progressive and irreversible condition. |
| Worsening of Existing Pancreatitis | Alcohol consumption can aggravate symptoms and complications in individuals with pre-existing pancreatitis. |
| Delayed Healing | Alcohol impairs the pancreas's ability to recover from injury, prolonging inflammation and tissue damage. |
| Increased Risk of Complications | Alcohol-induced pancreatitis is associated with higher risks of complications like pancreatic necrosis, pseudocysts, and organ failure. |
| Synergistic Effects with Other Factors | Alcohol's effects on the pancreas are compounded by factors like smoking, obesity, and genetic predisposition. |
| Recommendations | Complete abstinence from alcohol is strongly recommended for individuals with pancreatitis or at high risk of developing it. |
Explore related products






What You'll Learn
![]()
Alcohol’s role in pancreatic inflammation
Alcohol's direct toxicity to pancreatic acinar cells is a key mechanism in the development and exacerbation of pancreatitis. These cells, responsible for producing digestive enzymes, are particularly vulnerable to the metabolic byproducts of alcohol. When alcohol is metabolized, it generates acetaldehyde and free radicals, which can damage cellular membranes and DNA. This cellular stress triggers the premature activation of digestive enzymes within the pancreas, leading to self-digestion of pancreatic tissue—a hallmark of acute pancreatitis. Chronic alcohol consumption further exacerbates this process by increasing the production of pro-inflammatory cytokines, creating a cycle of inflammation and tissue damage.
Consider the dosage: studies show that consuming more than 4–5 standard drinks per day significantly elevates the risk of pancreatitis. A standard drink is defined as 14 grams of pure alcohol, equivalent to a 12-ounce beer, 5-ounce glass of wine, or 1.5-ounce shot of distilled spirits. Individuals aged 40–60, particularly men, are more susceptible due to cumulative alcohol exposure and age-related metabolic changes. For those with a history of pancreatic issues, even moderate drinking (1–2 drinks daily) can aggravate inflammation, as the pancreas may already be compromised.
To mitigate alcohol-induced pancreatic inflammation, practical steps include limiting daily intake to no more than 1–2 standard drinks for women and 2–3 for men, with at least 2 alcohol-free days per week. Hydration is critical, as alcohol dehydrates the body and thickens pancreatic secretions, increasing the risk of duct obstruction. Pairing alcohol with food slows absorption, reducing peak blood alcohol levels and associated metabolic stress. For individuals with recurrent pancreatitis, abstinence is strongly recommended, as even small amounts of alcohol can reignite inflammation.
Comparatively, alcohol’s role in pancreatic inflammation contrasts with other causes like gallstones, which are mechanical in nature. While gallstones cause acute blockage and immediate inflammation, alcohol’s damage is cumulative, often leading to chronic pancreatitis over years. Unlike gallstone-induced pancreatitis, which may resolve with surgical intervention, alcohol-related cases require lifestyle changes and long-term management. This distinction highlights the need for targeted prevention strategies, such as screening heavy drinkers for early pancreatic dysfunction and educating at-risk populations about the irreversible nature of alcohol-induced damage.
Descriptively, the pancreas under chronic alcohol assault becomes a battleground of inflammation and fibrosis. Acinar cells, once orderly and functional, degenerate into fatty deposits and necrotic tissue. The surrounding stroma thickens, compressing ducts and impairing enzyme flow. This architectural distortion not only perpetuates inflammation but also reduces the pancreas’s ability to regulate blood sugar and digest nutrients, leading to complications like diabetes and malnutrition. Imaging studies often reveal a shrunken, calcified organ—a stark visual reminder of alcohol’s destructive power. Reversing this damage is nearly impossible, underscoring the urgency of early intervention and abstinence.
Alcohol Consumption: Dietary Guidelines and Recommendations
You may want to see also
Explore related products




![]()
Acute vs. chronic pancreatitis risks
Alcohol's role in pancreatitis is a critical factor, but the risks differ sharply between acute and chronic forms. Acute pancreatitis often arises from a sudden, heavy alcohol intake—typically defined as consuming 4-5 drinks in a single session for men, or 3-4 for women. This binge-drinking pattern triggers an inflammatory response, causing the pancreas to digest itself, a condition that can be life-threatening if not promptly treated. In contrast, chronic pancreatitis develops over years of consistent, heavy drinking, usually exceeding 5-7 drinks daily for men and 3-4 for women. The cumulative damage leads to irreversible pancreatic tissue scarring, impairing digestion and often resulting in persistent pain and malnutrition.
Understanding the distinct mechanisms of alcohol-induced pancreatitis is key to prevention. Acute pancreatitis is primarily driven by toxic metabolites produced during alcohol breakdown, which directly injure pancreatic cells. Chronic pancreatitis, however, involves repeated episodes of subclinical inflammation, fibrosis, and ductal obstruction, exacerbated by alcohol’s interference with pancreatic enzyme secretion. For instance, alcohol disrupts the balance of digestive enzymes, causing them to activate prematurely within the pancreas rather than the intestine, a hallmark of chronic damage. This distinction underscores why even moderate drinkers are not entirely safe—sporadic heavy drinking can still trigger acute episodes, while consistent consumption accelerates chronic progression.
Practical risk mitigation strategies vary depending on the type of pancreatitis. For acute pancreatitis, the most effective approach is to avoid binge drinking altogether. Limiting alcohol intake to 1-2 drinks per day, if consumed at all, significantly reduces the risk. For those with a history of acute pancreatitis, complete abstinence is advised, as recurrence can lead to chronic complications. In chronic pancreatitis, cessation of alcohol use is non-negotiable. Even small amounts can exacerbate symptoms and accelerate pancreatic failure. Patients should also adopt a low-fat, high-protein diet and consider enzyme replacement therapy to manage digestive issues.
Age and genetic predisposition further complicate the risk landscape. Younger individuals, particularly those under 30, are more susceptible to acute pancreatitis due to binge-drinking trends, while chronic pancreatitis predominantly affects those over 40 with a long history of alcohol abuse. Genetic factors, such as mutations in the *PRSS1* or *SPINK1* genes, can lower the threshold for alcohol-induced damage, making some individuals more vulnerable even at lower consumption levels. Screening for these mutations in heavy drinkers can help tailor preventive measures, emphasizing the need for personalized risk assessment.
In summary, while alcohol aggravates both acute and chronic pancreatitis, the risks and preventive strategies diverge significantly. Acute pancreatitis demands immediate behavioral changes to avoid binge drinking, whereas chronic pancreatitis requires total abstinence and long-term management. Recognizing these differences empowers individuals to make informed choices, potentially preventing severe complications and improving quality of life. Whether through moderation, cessation, or medical intervention, addressing alcohol’s role is paramount in combating pancreatitis.
Effective Strategies to Safely Plug Alcohol for Responsible Consumption
You may want to see also
Explore related products





![]()
Mechanism of alcohol-induced damage
Chronic alcohol consumption is a well-established risk factor for pancreatitis, but the mechanism by which it inflicts damage is multifaceted. One primary pathway involves the metabolism of alcohol in the pancreas. When alcohol is consumed, it is broken down by enzymes such as alcohol dehydrogenase (ADH) and cytochrome P450 2E1 (CYP2E1). This process generates acetaldehyde, a toxic byproduct, and free radicals, which are highly reactive molecules that can damage pancreatic cells. Over time, this oxidative stress leads to inflammation and cell death, contributing to the development of pancreatitis. For instance, studies show that heavy drinking, defined as more than 4-5 drinks per day for men and 3 drinks per day for women, significantly increases the risk of pancreatic damage due to this metabolic process.
Another critical mechanism is the activation of digestive enzymes within the pancreas itself. Normally, these enzymes are produced in an inactive form and are only activated in the small intestine to aid digestion. However, alcohol disrupts this process by causing premature activation of enzymes like trypsinogen, which then begin digesting the pancreas itself—a phenomenon known as autodigestion. This internal destruction triggers a cascade of inflammation and tissue damage, hallmark features of acute and chronic pancreatitis. Research indicates that even a single binge-drinking episode, consuming 4-5 drinks in 2 hours, can precipitate this harmful activation in susceptible individuals.
Alcohol also exacerbates pancreatic injury by impairing the organ’s blood flow. Chronic alcohol use leads to vasoconstriction, reducing blood supply to the pancreas and creating a hypoxic environment. This ischemia further stresses pancreatic cells, making them more vulnerable to damage from toxins and inflammation. Additionally, alcohol interferes with the pancreas’s ability to repair itself by inhibiting the production of growth factors and promoting fibrosis, or scarring, which compromises its function over time. For those with pre-existing pancreatic conditions, even moderate alcohol intake (1-2 drinks daily) can accelerate this fibrotic process, worsening outcomes.
A less obvious but equally important mechanism is alcohol’s impact on the gut microbiome and intestinal barrier function. Chronic drinking alters the balance of gut bacteria, leading to increased intestinal permeability, or "leaky gut." This allows bacteria and toxins to enter the bloodstream and reach the pancreas, triggering inflammation and immune responses. Such systemic effects compound the local damage caused by alcohol metabolism, creating a dual assault on pancreatic health. Practical advice for mitigating this risk includes limiting alcohol consumption and incorporating probiotics or fiber-rich foods to support gut integrity.
In summary, alcohol-induced pancreatic damage operates through metabolic toxicity, enzyme activation, vascular compromise, and gut-related pathways. Understanding these mechanisms underscores the importance of moderation or abstinence, particularly for individuals at risk. For heavy drinkers, reducing intake to below recommended thresholds (no more than 2 drinks per day for men and 1 for women) can significantly lower the risk of pancreatitis. For those with existing pancreatic issues, complete abstinence is often advised to prevent further harm. This knowledge empowers individuals to make informed choices to protect their pancreatic health.
Does a Pina Colada Contain Alcohol? The Tropical Cocktail Truth
You may want to see also
Explore related products






![]()
Impact on pancreatic enzymes
Alcohol's direct toxicity to pancreatic acinar cells disrupts enzyme production and secretion, a critical factor in pancreatitis exacerbation. These cells, responsible for synthesizing digestive enzymes like amylase, lipase, and proteases, are particularly vulnerable to ethanol and its metabolite, acetaldehyde. Chronic alcohol consumption leads to intracellular accumulation of these enzymes, causing premature activation and autodigestion of the pancreas. For instance, studies show that alcohol-induced oxidative stress increases the expression of cationic green protein (CGP), a marker of acinar cell injury, by up to 40% in animal models. This enzymatic imbalance not only triggers inflammation but also perpetuates tissue damage, creating a vicious cycle of pancreatic dysfunction.
Consider the enzymatic cascade: normally, pancreatic enzymes are secreted in an inactive form to prevent self-digestion. Alcohol disrupts this mechanism by promoting the activation of trypsinogen to trypsin within the acinar cells. A single binge-drinking episode (defined as 4–5 drinks in 2 hours for men, 3–4 for women) can elevate serum amylase and lipase levels by 2–3 times the upper limit of normal, signaling acute pancreatic injury. Over time, repeated episodes lead to chronic pancreatitis, where enzyme insufficiency becomes irreversible. Patients with this condition often require pancreatic enzyme replacement therapy (PERT) to aid digestion, highlighting the long-term consequences of alcohol-induced enzyme derangement.
From a preventive standpoint, limiting alcohol intake is paramount. For individuals at risk, adhering to moderate drinking guidelines—up to 1 drink per day for women and 2 for men—can mitigate enzymatic stress. However, abstinence is recommended for those with pre-existing pancreatic conditions. Incorporating antioxidants like vitamin C and E may help counteract alcohol-induced oxidative damage, though this should not replace abstinence. For example, a study in *Gut* (2018) found that patients who abstained from alcohol for 6 months showed a 50% reduction in pancreatic enzyme abnormalities compared to those who continued drinking.
Comparatively, alcohol’s impact on pancreatic enzymes is more severe than other dietary factors. While high-fat diets or gallstones can cause transient enzyme elevations, alcohol’s direct cytotoxicity and metabolic byproducts create sustained damage. Unlike dietary triggers, alcohol’s effects are dose-dependent and cumulative, with even moderate long-term consumption increasing pancreatitis risk by 3–5 times. This distinction underscores why alcohol cessation is the cornerstone of pancreatitis management, whereas dietary modifications alone are often insufficient for alcohol-induced cases.
Descriptively, the pancreas under chronic alcohol assault resembles a factory in chaos. Enzymes meant for external digestion turn inward, dissolving the very tissue that produces them. Microscopic examination reveals acinar cell vacuolization, fat necrosis, and inflammatory infiltrates—hallmarks of alcohol-induced pancreatitis. Clinically, this manifests as severe abdominal pain, nausea, and steatorrhea, symptoms directly linked to enzymatic dysfunction. Reversing this damage requires not just enzyme supplementation but also addressing the root cause: alcohol abstinence. Without it, the pancreas remains trapped in a cycle of injury and repair, ultimately leading to organ failure.
Gargling Alcohol Mouthwash for Sore Throat: Safe or Risky Remedy?
You may want to see also
Explore related products
![McKesson Isopropyl Rubbing Alcohol 70% [1 Count] USP First Aid Antiseptic, 32 oz](https://m.media-amazon.com/images/I/61lYiXl9g9L._AC_UL320_.jpg)





![]()
Alcohol cessation benefits for pancreatitis
Alcohol consumption is a well-established risk factor for pancreatitis, with chronic drinking significantly increasing the likelihood of developing this painful and potentially life-threatening condition. For individuals diagnosed with pancreatitis, whether acute or chronic, the question of alcohol's role in disease progression is critical. The answer is unequivocal: alcohol does aggravate pancreatitis, and its cessation is a cornerstone of management. This is not merely a theoretical recommendation but a practical, evidence-based intervention that can halt disease progression, alleviate symptoms, and improve quality of life.
Consider the mechanism: alcohol metabolization produces toxic byproducts that directly injure pancreatic cells, triggering inflammation and impairing the organ’s ability to function. Even moderate drinking can exacerbate existing pancreatic damage, leading to recurrent acute episodes or accelerating the transition to chronic pancreatitis. For instance, studies show that individuals with chronic pancreatitis who continue drinking are three times more likely to experience complications such as pancreatic calcification, pseudocysts, or diabetes compared to those who abstain. The dosage effect is clear—the more alcohol consumed, the greater the risk of worsening the condition.
From a practical standpoint, alcohol cessation is not just beneficial; it is essential. For patients with acute pancreatitis, abstaining from alcohol during recovery prevents recurrence and allows the pancreas to heal. For those with chronic pancreatitis, quitting alcohol is the single most effective measure to slow disease progression and reduce pain episodes. A study published in *Gut* found that patients with chronic pancreatitis who stopped drinking experienced a 50% reduction in pain-related hospitalizations within the first year of cessation. This underscores the immediate and tangible benefits of quitting alcohol.
However, cessation is not without challenges. Alcohol dependence is common among pancreatitis patients, and quitting often requires a structured approach. Behavioral therapy, support groups like Alcoholics Anonymous, and medications such as naltrexone or acamprosate can aid in maintaining sobriety. Practical tips include avoiding triggers, replacing drinking habits with healthier activities, and seeking professional help early. For example, a 45-year-old patient with chronic pancreatitis might start by setting a quit date, removing alcohol from their home, and engaging in daily exercise to manage cravings.
In comparison to other interventions, such as dietary modifications or enzyme replacement therapy, alcohol cessation stands out for its profound impact on disease trajectory. While a low-fat diet and pancreatic enzymes address symptoms, quitting alcohol targets the root cause of ongoing damage. This makes it a non-negotiable step in pancreatitis management, particularly for alcohol-induced cases. The takeaway is clear: for pancreatitis patients, alcohol cessation is not optional—it is a critical, life-altering decision that can prevent irreversible harm and pave the way for recovery.
Hand Sanitizer Alcohol: Types, Uses, and Safety Concerns Explained
You may want to see also
Frequently asked questions
Yes, alcohol consumption can significantly aggravate pancreatitis. Chronic alcohol use is a leading cause of pancreatitis and can lead to repeated episodes or chronic pancreatitis, causing long-term damage to the pancreas.
While moderate alcohol intake may not directly cause pancreatitis in everyone, it can still irritate the pancreas and worsen symptoms in individuals already diagnosed with the condition. It’s best to avoid alcohol entirely if you have pancreatitis.
Improvement in pancreatitis symptoms after quitting alcohol varies, but many people notice a reduction in inflammation and pain within weeks to months. However, long-term damage from chronic pancreatitis may not be fully reversible.
No, it is not safe to drink alcohol after recovering from pancreatitis. Even small amounts of alcohol can trigger a recurrence or worsen the condition, especially in individuals with a history of alcohol-induced pancreatitis.








![McKesson Isopropyl Rubbing Alcohol 70% [12 Count] USP First Aid Antiseptic, 16 oz](https://m.media-amazon.com/images/I/614SGew9G8L._AC_UL320_.jpg)





















