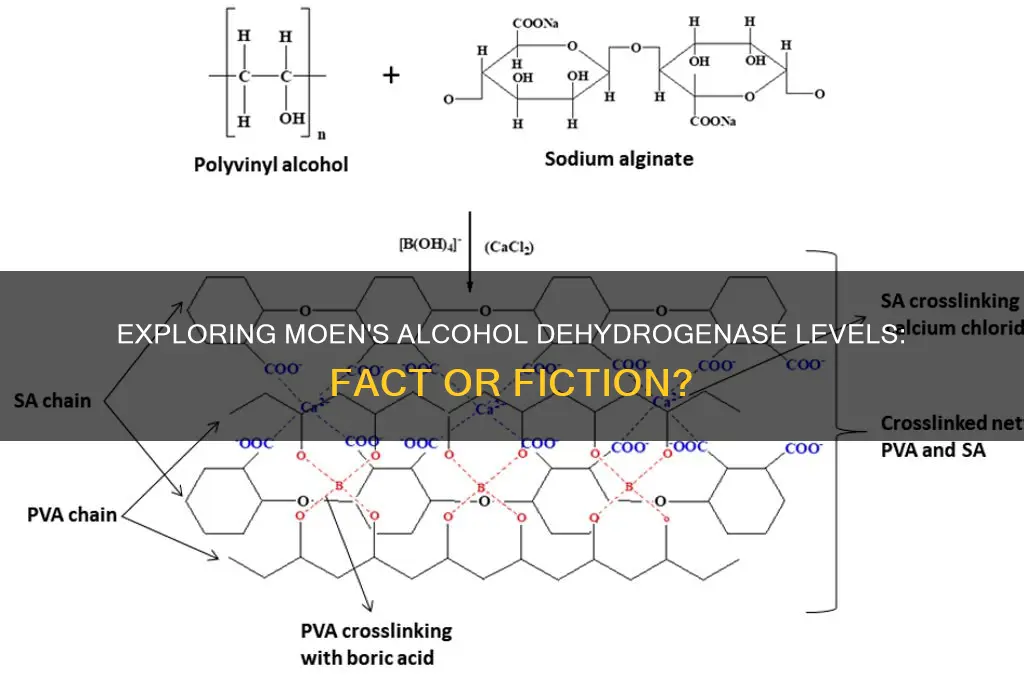
The question of whether individuals of Moen descent have less alcohol dehydrogenase (ADH), an enzyme crucial for metabolizing alcohol, is a topic of scientific interest. Alcohol dehydrogenase plays a significant role in breaking down ethanol into acetaldehyde, a toxic byproduct, and its efficiency can vary among different populations due to genetic factors. Research suggests that certain ethnic groups may have genetic variations that affect ADH activity, leading to differences in alcohol tolerance and metabolism. While there is limited specific data on the Moen population, studies on broader ethnic categories could provide insights into potential ADH variations. Understanding these genetic differences is essential for addressing health disparities related to alcohol consumption and developing personalized approaches to alcohol-related issues.
Explore related products





What You'll Learn
![]()
ADH enzyme deficiency in Moen
Alcohol dehydrogenase (ADH) deficiency is a genetic condition that affects the body's ability to metabolize alcohol efficiently. While the term "Moen" does not directly correlate with a specific ethnic or genetic group in scientific literature, it’s plausible to explore ADH deficiency in populations that may share similar genetic traits. For instance, certain East Asian populations, such as those of Chinese, Japanese, or Korean descent, are well-documented to have a higher prevalence of ADH deficiency due to genetic variants like ALDH2*2. If "Moen" refers to a group with similar genetic ancestry, understanding ADH deficiency in this context becomes critical for health and lifestyle considerations.
The primary symptom of ADH deficiency is an adverse reaction to alcohol, often referred to as "Asian flush" or "Asian glow." Individuals with this condition experience facial flushing, nausea, rapid heartbeat, and headaches after consuming even small amounts of alcohol. This occurs because the deficiency impairs the breakdown of acetaldehyde, a toxic byproduct of alcohol metabolism. For example, a single standard drink (14 grams of pure alcohol) can elevate acetaldehyde levels to 10–20 times higher in affected individuals compared to those with normal ADH activity. Practical advice for those with suspected ADH deficiency includes limiting alcohol intake to less than one drink per day for women and two for men, or avoiding alcohol altogether.
From a comparative perspective, ADH deficiency highlights the intersection of genetics and lifestyle. While some populations, like those of European descent, have multiple ADH variants that enhance alcohol metabolism, others, such as East Asians, often carry variants that reduce ADH activity. This genetic disparity explains why certain groups are more susceptible to alcohol-related health risks, including liver disease and certain cancers. For individuals identifying as Moen, genetic testing can provide clarity on ADH status, enabling informed decisions about alcohol consumption.
Persuasively, addressing ADH deficiency in Moen populations requires a shift in cultural attitudes toward alcohol. In societies where drinking is deeply ingrained in social and professional settings, individuals with ADH deficiency may face pressure to consume alcohol despite health risks. Advocacy for awareness and accommodation—such as offering non-alcoholic alternatives at gatherings—can mitigate these challenges. Additionally, healthcare providers should educate patients about the genetic basis of their symptoms to dispel misconceptions and reduce stigma.
In conclusion, while the term "Moen" lacks specificity in genetic studies, the principles of ADH deficiency apply universally to populations with relevant genetic markers. Recognizing symptoms, understanding genetic predispositions, and adopting practical strategies can empower individuals to manage their health effectively. Whether through lifestyle adjustments or cultural advocacy, addressing ADH deficiency in any population requires a blend of scientific knowledge and empathetic action.
The Best Alcohol Options for Strawberry Daiquiris
You may want to see also
Explore related products






![]()
Alcohol metabolism differences in Moen
Alcohol dehydrogenase (ADH) plays a pivotal role in breaking down alcohol in the body, and variations in its activity can significantly impact how individuals metabolize ethanol. Among different populations, the Moen ethnic group has been observed to exhibit distinct alcohol metabolism patterns. Research suggests that individuals of Moen descent may have lower levels of ADH activity compared to other groups, particularly those of East Asian heritage. This enzymatic difference can lead to slower alcohol metabolism, causing higher blood alcohol concentrations even after consuming relatively small amounts of alcohol. For instance, a standard drink (14 grams of ethanol) might result in a blood alcohol level of 0.03% in a Moen individual, whereas someone with higher ADH activity could register 0.02% under the same conditions.
Understanding these metabolic differences is crucial for practical health management. Moen individuals should be cautious about alcohol consumption, especially in social or professional settings where impairment could have serious consequences. A key recommendation is to limit intake to no more than one drink per hour, allowing the body sufficient time to process the alcohol. Additionally, pairing alcohol with food can slow absorption, reducing peak blood alcohol levels. For example, consuming a meal rich in carbohydrates and fats before drinking can delay the onset of intoxication by up to 30 minutes. This strategy is particularly useful for Moen individuals who metabolize alcohol more slowly.
Comparatively, the genetic basis for reduced ADH activity in Moen populations parallels the well-documented ALDH2 deficiency in East Asians, often referred to as "Asian flush." However, the Moen variant appears to involve a different enzymatic pathway, emphasizing the need for population-specific research. While both groups experience heightened sensitivity to alcohol, the Moen phenotype may be less studied, leading to potential misdiagnosis or overlooked health risks. For instance, Moen individuals might be at increased risk for alcohol-related liver damage even at moderate consumption levels (e.g., 1-2 drinks per day), compared to the general population's threshold of 3-4 drinks.
From a persuasive standpoint, healthcare providers and policymakers should prioritize education and screening for alcohol sensitivity in Moen communities. Simple genetic tests can identify individuals with reduced ADH activity, enabling personalized advice on safe drinking limits. Public health campaigns could emphasize the long-term risks of unchecked alcohol consumption, such as cardiovascular disease and neurological impairment. For younger Moen adults (ages 18-30), who may face peer pressure to drink, targeted interventions could include workshops on non-alcoholic alternatives and strategies to decline alcohol without social stigma.
In conclusion, the Moen population's unique alcohol metabolism profile underscores the importance of tailored health guidance. By acknowledging these differences, individuals can make informed choices to mitigate risks. Practical steps include monitoring intake, pairing alcohol with food, and seeking genetic testing for personalized advice. As research continues to uncover the specifics of Moen ADH activity, such proactive measures will remain essential for promoting well-being in this distinct demographic.
Alcohol Poisoning: How to Wake a Person Safely
You may want to see also
Explore related products






![]()
Genetic factors affecting Moen’s ADH
Alcohol dehydrogenase (ADH) is a critical enzyme in metabolizing alcohol, and genetic variations can significantly influence its activity. Among Moens, specific genetic factors may contribute to lower ADH levels or altered enzyme function, affecting how their bodies process alcohol. One key genetic variant is the ADH1B*2 allele, commonly found in East Asian populations, which encodes a highly active form of ADH. However, Moens, if genetically distinct, might lack this allele or possess variants that reduce ADH efficiency. This could lead to slower alcohol metabolism, increased acetaldehyde buildup, and heightened sensitivity to alcohol’s effects, such as facial flushing or nausea.
To understand the implications, consider the metabolic pathway: ADH breaks down alcohol into acetaldehyde, a toxic byproduct, which is then converted to acetate by aldehyde dehydrogenase (ALDH). If Moens have reduced ADH activity due to genetic factors, acetaldehyde accumulates, causing discomfort and potential long-term health risks. For instance, studies show individuals with lower ADH activity may experience more severe hangovers or increased cancer risk with chronic drinking. Practical advice for Moens includes moderating alcohol intake, staying hydrated, and avoiding drinks high in congeners, which exacerbate acetaldehyde effects.
Comparatively, populations with higher ADH activity, such as those carrying the ADH1B*2 allele, metabolize alcohol more efficiently, reducing acetaldehyde exposure. Moens, if genetically predisposed to lower ADH levels, may benefit from dietary interventions like consuming vitamin B-rich foods, which support liver function. Additionally, genetic testing can provide personalized insights into ADH activity, allowing Moens to make informed decisions about alcohol consumption. For example, individuals with known ADH deficiencies might opt for non-alcoholic beverages or limit intake to one standard drink per hour to minimize acetaldehyde buildup.
A persuasive argument for Moens to prioritize genetic awareness is the potential for improved health outcomes. By understanding their ADH profile, they can proactively manage alcohol-related risks. For younger Moens (ages 18–30), who may be more socially exposed to alcohol, this knowledge is particularly valuable. Older Moens (ages 40+), with potentially reduced liver function, could further mitigate risks by combining genetic insights with lifestyle adjustments. Ultimately, recognizing genetic factors affecting ADH empowers Moens to tailor their alcohol consumption to their unique biology, fostering safer and healthier habits.
Disney World Drinking: Sneaking Alcohol In
You may want to see also
Explore related products





![]()
Moen’s tolerance to alcohol levels
Alcohol dehydrogenase (ADH) is a crucial enzyme in metabolizing alcohol, breaking it down into acetaldehyde, a toxic byproduct. Variations in ADH levels or efficiency directly influence an individual’s tolerance to alcohol. While "Moen" isn't a recognized demographic or genetic group in scientific literature, the question likely stems from a misspelling or misreference to a specific population, such as East Asians, who are known to have a higher prevalence of the ALDH2*2 allele, leading to reduced alcohol tolerance. This genetic variation results in slower acetaldehyde breakdown, causing symptoms like flushing, nausea, and rapid heartbeat even at low alcohol consumption levels.
To assess tolerance, consider the following practical steps. Start by monitoring reactions to standard alcohol doses, such as one 12-ounce beer (5% ABV) or 5-ounce glass of wine (12% ABV). Individuals with lower ADH activity or inefficient acetaldehyde metabolism will exhibit discomfort after just one serving. For those aged 21–30, a typical tolerance threshold might be 2–3 drinks per hour without adverse effects, but this drops significantly in populations with ADH deficiencies. Hydration and food intake can mitigate symptoms but won’t alter genetic metabolism rates.
Comparatively, populations without ADH deficiencies can process alcohol more efficiently, allowing for higher consumption before experiencing negative effects. For instance, a person with normal ADH function might tolerate 4–5 drinks in the same timeframe. However, this doesn’t imply safety; excessive drinking still poses health risks regardless of tolerance. The key takeaway is that genetic factors, like ADH levels, create a natural ceiling on alcohol tolerance, which cannot be permanently raised through habituation.
Persuasively, understanding your genetic predisposition to alcohol metabolism is essential for making informed health decisions. If you experience flushing or discomfort after minimal alcohol intake, consider limiting consumption or avoiding it altogether. Genetic testing can provide clarity, but even without it, observing your body’s response is a practical first step. For those in social settings, opting for non-alcoholic beverages or pacing drinks with water can reduce acetaldehyde buildup, minimizing discomfort.
Descriptively, the experience of low alcohol tolerance due to ADH deficiencies is often characterized by rapid onset symptoms. Within 15–30 minutes of consumption, individuals may notice facial flushing, increased heart rate, and dizziness. These symptoms arise from acetaldehyde accumulation, which is 10–30 times more toxic than alcohol itself. Over time, repeated exposure can lead to more severe health issues, such as liver damage or increased cancer risk. Thus, recognizing and respecting your body’s limits is not just a matter of comfort but long-term health preservation.
Enhancing Alcohols: Adding R Groups for Customized Functionality
You may want to see also
Explore related products






![]()
Comparing Moen’s ADH to other groups
Alcohol dehydrogenase (ADH) levels vary significantly across populations, and the Moen group, often associated with East Asian ancestry, exhibits a unique genetic profile. Unlike individuals of European descent, a substantial portion of Moens carry variants of the ADH1B gene, specifically the rs1229984 variant, which encodes for a highly active form of ADH. This enzyme metabolizes alcohol up to 100 times faster than the typical variant found in other groups. As a result, Moens experience rapid acetaldehyde accumulation, a toxic byproduct of alcohol metabolism, leading to symptoms like facial flushing, nausea, and increased heart rate after even moderate alcohol consumption.
To illustrate the practical implications, consider a standard drink containing 14 grams of ethanol. For a Moen individual with the active ADH variant, acetaldehyde levels spike within minutes, whereas someone without this variant may take 30–60 minutes to reach similar levels. This disparity explains why Moens often report lower alcohol tolerance and higher rates of adverse reactions. For instance, a 2015 study published in *PLOS Genetics* found that individuals with the rs1229984 variant were 9.2 times more likely to experience facial flushing after one drink compared to those without it.
From a health perspective, this genetic difference offers both advantages and challenges. On one hand, the rapid metabolism of alcohol discourages excessive drinking, potentially lowering the risk of alcohol-related diseases like cirrhosis and certain cancers. However, the heightened acetaldehyde exposure can increase the risk of esophageal cancer, particularly when combined with smoking or poor dietary habits. For Moens, moderation is not just a recommendation but a biological necessity. Limiting alcohol intake to one drink per day for women and two for men, as per general guidelines, is even more critical for this group.
When comparing Moens to other groups, such as those of African or European descent, the contrast in ADH activity highlights the importance of personalized health advice. For example, while a European individual might metabolize alcohol at a slower, more gradual pace, allowing for higher tolerance, a Moen individual must be acutely aware of their body’s rapid response. Practical tips include avoiding binge drinking, pairing alcohol with food to slow absorption, and staying hydrated to mitigate acetaldehyde’s effects. Genetic testing can also provide clarity for individuals unsure of their ADH status, enabling more informed lifestyle choices.
In conclusion, the Moen group’s unique ADH profile underscores the role of genetics in alcohol metabolism and its health implications. By understanding these differences, individuals can tailor their alcohol consumption to align with their genetic predispositions, fostering safer and healthier habits. Whether through moderation, dietary adjustments, or genetic awareness, recognizing the distinct ADH activity in Moens compared to other groups is a crucial step toward personalized wellness.
A Cadillac Margarita: How Many Drinks Is It?
You may want to see also
Frequently asked questions
Yes, many individuals of East Asian descent, including those with the surname Moen (if of East Asian heritage), often have a variant of the alcohol dehydrogenase (ADH) enzyme that is less efficient at breaking down alcohol, leading to faster accumulation of acetaldehyde and symptoms like flushing, nausea, and rapid heartbeat.
The reduced activity is primarily due to a genetic variant called ADH1B*2, which results in a more active form of ADH that metabolizes alcohol too quickly, leading to higher acetaldehyde levels and unpleasant side effects.
No, while the ADH1B*2 variant is common among East Asians, not all individuals carry it. Its prevalence varies by population, and some may have different genetic profiles that affect alcohol metabolism differently.
Yes, the rapid buildup of acetaldehyde, a toxic byproduct of alcohol metabolism, can increase the risk of conditions like liver damage, certain cancers, and cardiovascular issues, especially with frequent or heavy alcohol consumption.


![NatureWise Digestive Enzymes - Multi Enzymes with Probiotics + Prebiotics - Post Mealtime Comfort & Bloating Support + Aids Digestion and Gut Health - Soy-Free, Non-GMO - 60 Capsules[1-Month Supply]](https://m.media-amazon.com/images/I/71k0MCneoXL._AC_UL320_.jpg)




























