The question of whether Americans handle alcohol differently is a multifaceted one, influenced by cultural, social, and even biological factors. American attitudes toward alcohol consumption are shaped by a unique blend of historical temperance movements, diverse cultural backgrounds, and varying regional norms. For instance, while some regions embrace a more relaxed approach to drinking, others maintain stricter attitudes rooted in religious or community values. Additionally, differences in drinking patterns, such as the prevalence of binge drinking among younger demographics, highlight distinct behaviors compared to other cultures. Biological factors, such as genetic variations in alcohol metabolism, may also play a role in how individuals respond to alcohol. Understanding these nuances provides insight into why Americans might handle alcohol differently from their global counterparts.
| Characteristics | Values |
|---|---|
| Metabolism Differences | Americans, particularly those of East Asian descent, often have a genetic variant (ALDH2 deficiency) leading to slower alcohol metabolism and increased acetaldehyde buildup. |
| Tolerance Levels | Genetic factors and cultural drinking habits influence alcohol tolerance; some populations may have lower tolerance due to less exposure or genetic predispositions. |
| Enzyme Activity (ADH & ALDH) | Variations in alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) enzymes affect how quickly alcohol is broken down, with some groups experiencing faster or slower processing. |
| Flush Reaction | Individuals with ALDH2 deficiency often experience facial flushing, nausea, and rapid heartbeat after alcohol consumption due to acetaldehyde accumulation. |
| Cultural Drinking Patterns | American drinking habits vary by ethnicity, with some groups consuming alcohol less frequently or in smaller quantities due to cultural or religious norms. |
| Health Risks | Slower metabolism increases the risk of alcohol-related health issues, such as liver disease, cancer, and cardiovascular problems, in certain populations. |
| Genetic Prevalence | ALDH2 deficiency is more common in East Asian populations (up to 50%) but can also occur in other ethnic groups, albeit less frequently. |
| Behavioral Responses | Genetic factors may influence drinking behavior, with some individuals avoiding alcohol due to unpleasant side effects from inefficient metabolism. |
| Alcohol Consumption Rates | Drinking patterns in the U.S. vary widely by ethnicity, with some groups reporting lower per capita alcohol consumption due to genetic or cultural factors. |
| Public Health Implications | Understanding genetic differences in alcohol metabolism helps tailor public health interventions and alcohol education for specific populations. |
Explore related products






What You'll Learn
- Genetic variations in alcohol metabolism among different ethnic groups in the United States
- Cultural attitudes toward alcohol consumption in various American infant communities
- Impact of socioeconomic status on alcohol handling and consumption patterns in America
- Regional differences in alcohol preferences and consumption habits across the United States
- Health disparities related to alcohol use among diverse American infant populations
![]()
Genetic variations in alcohol metabolism among different ethnic groups in the United States
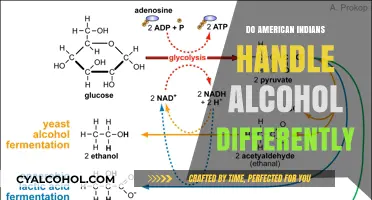
Alcohol metabolism varies significantly across ethnic groups in the United States due to genetic differences, particularly in the enzymes alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH). These enzymes break down alcohol into acetaldehyde and then into acetic acid, which the body can eliminate. East Asian populations, for example, often carry the ALDH2*2 allele, which results in a deficient form of ALDH2. This genetic variant leads to a buildup of toxic acetaldehyde, causing facial flushing, nausea, and rapid heartbeat after even small amounts of alcohol consumption. Studies show that approximately 30-50% of East Asians experience these symptoms, compared to less than 1% of Europeans. This genetic predisposition not only affects tolerance but also influences drinking behavior and alcohol-related health risks.
Consider the practical implications of these genetic variations in social or medical contexts. For instance, healthcare providers should be aware of a patient’s ethnic background when prescribing medications metabolized by the same pathways as alcohol, such as certain sedatives or pain relievers. For individuals of East Asian descent, even moderate alcohol intake (e.g., one standard drink, equivalent to 14 grams of pure alcohol) can trigger adverse reactions. Conversely, some African and Indigenous American populations have higher ADH activity, allowing for faster alcohol breakdown but potentially increasing the risk of dependence due to reduced aversive effects. Understanding these differences can inform personalized health advice and interventions.
From a persuasive standpoint, acknowledging these genetic disparities challenges the one-size-fits-all approach to alcohol guidelines. The current U.S. Dietary Guidelines recommend limiting alcohol to one drink per day for women and two for men, but these thresholds may not account for metabolic variations. For example, a 50-year-old East Asian woman might experience discomfort after half a drink due to ALDH2 deficiency, while a Native American man with high ADH activity could metabolize two drinks quickly but face higher addiction risks. Advocacy for ethnic-specific guidelines could reduce health disparities, particularly in liver disease and cancer rates, which are disproportionately higher in certain groups.
Comparatively, genetic variations in alcohol metabolism also highlight evolutionary adaptations. In populations with a long history of alcohol consumption, such as Europeans, genetic mutations that enhance alcohol breakdown (e.g., ADH1B*2) are more common, providing a survival advantage in regions where fermented beverages were safer to drink than water. In contrast, groups with limited historical exposure to alcohol, like some Indigenous American communities, often lack these protective variants, making them more susceptible to alcohol-related harm. This evolutionary lens underscores the importance of cultural and historical context in shaping genetic traits.
Finally, a descriptive approach reveals the complexity of these genetic interactions. For example, the "Asian glow" phenomenon, caused by ALDH2 deficiency, is not merely a social inconvenience but a biomarker for increased cancer risk. Acetaldehyde, the toxic byproduct, damages DNA and disrupts cell repair mechanisms, elevating the likelihood of esophageal and liver cancers. In the U.S., where alcohol consumption is prevalent across diverse ethnic groups, recognizing these genetic markers could enable early screening and prevention strategies. By integrating genetic testing into routine healthcare, individuals could receive tailored advice, such as avoiding alcohol altogether or limiting intake to negligible amounts, to mitigate long-term health risks.
Prepping Your Canvas for Alcohol Ink: A Beginner's Guide
You may want to see also
Explore related products






![]()
Cultural attitudes toward alcohol consumption in various American infant communities
American infants, by definition, do not consume alcohol. However, cultural attitudes toward alcohol within their communities can shape early perceptions and future behaviors. These attitudes vary widely across different American ethnic, religious, and socioeconomic groups, influencing how alcohol is discussed, normalized, or restricted in the presence of children.
Understanding these nuances is crucial for parents, educators, and healthcare providers aiming to foster healthy relationships with alcohol in the next generation.
Observing Cultural Norms: In some communities, alcohol is seamlessly integrated into daily life and social gatherings. For instance, in many European-American households, wine with dinner or beer at barbecues is commonplace, often with children observing or even being offered sips as a cultural rite of passage. Conversely, in many Muslim-American families, alcohol is strictly prohibited due to religious teachings, creating an environment where children grow up with a clear understanding of its absence. These contrasting norms lay the foundation for vastly different attitudes toward alcohol, even before children reach drinking age.
Impact on Future Behavior: Research suggests that children who grow up in environments where alcohol is consumed moderately and responsibly are less likely to engage in binge drinking or develop alcohol-related problems later in life. Conversely, both strict prohibition and excessive consumption within the home can lead to curiosity, rebellion, or unhealthy patterns.
Navigating Cultural Differences: Parents and caregivers must navigate these cultural differences thoughtfully. For those in communities where alcohol is present, open and honest conversations about responsible drinking, age limits, and potential risks are essential. This includes discussing the legal drinking age of 21 in the United States and the reasons behind it. In communities where alcohol is absent, educating children about its prevalence in society and potential dangers is equally important, preparing them for encounters outside their immediate environment.
Practical Tips: Regardless of cultural background, establishing clear rules and expectations around alcohol is crucial. This includes setting a good example through one's own drinking habits, monitoring children's exposure to alcohol in media and social settings, and fostering open communication about peer pressure and making informed choices.
Choosing the Right Alcohol for Your DIY Alcohol Lamp
You may want to see also
Explore related products


$22.94 $24.29




![]()
Impact of socioeconomic status on alcohol handling and consumption patterns in America
Socioeconomic status (SES) significantly shapes how Americans handle and consume alcohol, influencing everything from drinking habits to health outcomes. Higher SES individuals often engage in moderate, socially acceptable drinking, such as a glass of wine with dinner, while lower SES groups may turn to cheaper, higher-alcohol-content beverages like malt liquor or spirits. This disparity isn’t just about preference—it’s rooted in accessibility, marketing, and environmental factors. For instance, neighborhoods with lower SES often have a higher density of liquor stores and fewer options for fresh, healthy foods, creating an environment where alcohol becomes a more visible and affordable coping mechanism.
Consider the role of stress and coping mechanisms. Lower SES individuals face greater financial instability, job insecurity, and limited access to healthcare, which can lead to higher stress levels. Alcohol, being a readily available and relatively inexpensive substance, often becomes a go-to method for stress relief. Studies show that while higher SES groups may drink more frequently, lower SES groups tend to consume larger quantities per session, increasing the risk of binge drinking. For example, the CDC reports that adults with an annual household income of less than $35,000 are more likely to engage in heavy drinking compared to those earning $75,000 or more.
The health implications of these patterns are stark. Chronic heavy drinking is linked to liver disease, cardiovascular problems, and mental health disorders, all of which disproportionately affect lower SES populations. However, these groups often lack access to quality healthcare, exacerbating the problem. In contrast, higher SES individuals are more likely to have health insurance, access to wellness programs, and the financial means to seek treatment for alcohol-related issues. This creates a cycle where alcohol misuse deepens existing socioeconomic inequalities, making it harder for lower SES individuals to improve their health and financial situations.
To address these disparities, targeted interventions are essential. Public health initiatives should focus on reducing the density of alcohol outlets in low-income neighborhoods and increasing access to affordable mental health resources. Employers can play a role by offering stress management programs and ensuring fair wages to reduce financial pressures. Individuals can take proactive steps, such as setting drinking limits (e.g., no more than one drink per day for women and two for men, as per NIH guidelines) and exploring alternative stress-relief methods like exercise or mindfulness. By acknowledging the socioeconomic roots of alcohol consumption patterns, we can develop strategies that promote healthier drinking habits across all income levels.
Understanding Alcohol Measurements: Grams in a Standard Shot
You may want to see also
Explore related products






![]()
Regional differences in alcohol preferences and consumption habits across the United States
The United States, a vast and culturally diverse nation, exhibits striking regional differences in alcohol preferences and consumption habits. From the craft beer havens of the Pacific Northwest to the whiskey-soaked traditions of the South, these variations reflect historical, economic, and social factors unique to each area. Understanding these differences not only sheds light on local cultures but also offers insights into broader trends in American drinking behavior.
Consider the Northeast, where the urban centers of New York and Boston have long been associated with a preference for cocktails and wine. In New York City, for instance, the cosmopolitan lifestyle fosters a demand for sophisticated drinks, with craft cocktails and imported wines dominating upscale bars. Conversely, in rural areas of New England, hard cider and locally distilled spirits hold a special place, often tied to colonial-era traditions. This duality highlights how even within a single region, consumption habits can diverge sharply based on urban versus rural settings.
In the South, whiskey reigns supreme, with Tennessee and Kentucky serving as the epicenters of American bourbon and rye production. Here, alcohol consumption is deeply intertwined with cultural identity, often enjoyed in social settings like barbecues or tailgates. Interestingly, the South also has some of the highest rates of abstinence due to religious influences, particularly in the Bible Belt. This paradox—a region both celebrated for its spirits and marked by significant temperance—underscores the complex relationship between alcohol and societal norms.
Out West, particularly in California, wine takes center stage, thanks to the world-renowned vineyards of Napa and Sonoma. The culture of wine tasting and pairing has permeated everyday life, with many residents incorporating wine into their meals as a matter of course. Meanwhile, in the Pacific Northwest, the craft beer movement has flourished, with cities like Portland, Oregon, boasting more breweries per capita than nearly anywhere else in the world. This regional pride in local brews has created a culture of experimentation, with IPAs, stouts, and sour beers gaining loyal followings.
Finally, the Midwest presents a unique blend of traditions, with a strong affinity for both beer and whiskey. States like Wisconsin and Minnesota are known for their high per capita beer consumption, often linked to their Germanic and Scandinavian heritage. At the same time, the region’s colder climate has fostered a preference for hearty, warming drinks, making whiskey a popular choice during the long winters. Practical tip: When visiting the Midwest, try a local craft beer or a classic Old Fashioned, a cocktail that originated in Wisconsin and remains a regional favorite.
These regional differences not only reflect local tastes but also influence national trends. For instance, the rise of craft beer in the Pacific Northwest has spurred similar movements across the country. By examining these variations, we gain a richer understanding of how geography, history, and culture shape the way Americans handle alcohol. Whether you’re a casual drinker or an enthusiast, recognizing these nuances can enhance your appreciation of the diverse drinking landscape across the United States.
Understanding the Scope of Alcoholism in the United States Today
You may want to see also
Explore related products






![]()
Health disparities related to alcohol use among diverse American infant populations
Alcohol exposure in utero disproportionately affects infants from marginalized communities, with Native American and African American populations bearing a higher burden of Fetal Alcohol Spectrum Disorders (FASDs). Studies show that socioeconomic factors like limited access to prenatal care and higher stress levels in these communities contribute to increased risk. For instance, Native American women are twice as likely as the general population to report alcohol use during pregnancy, partly due to historical trauma and systemic inequalities. This disparity highlights the need for culturally sensitive interventions that address both individual behaviors and systemic barriers.
Consider the role of healthcare access in exacerbating these disparities. Infants from low-income families, often overrepresented by racial minorities, are less likely to receive early screenings for FASDs. Without timely diagnosis, these children miss critical developmental interventions, such as speech therapy or behavioral support, which could mitigate long-term effects. A 2021 study found that only 10% of children with FASDs from low-income households received a diagnosis before age 6, compared to 30% in higher-income households. To bridge this gap, healthcare providers should implement universal prenatal alcohol screening and offer resources like telehealth consultations for families in underserved areas.
Persuasive arguments for policy change are essential. Legislation like the Affordable Care Act has expanded Medicaid coverage for prenatal care, but more targeted efforts are needed. For example, funding community health workers who speak local languages and understand cultural norms could improve education about alcohol risks during pregnancy. Additionally, policies that address social determinants of health—such as housing instability and food insecurity—could reduce stress-related alcohol use in marginalized populations. Without such systemic changes, health disparities will persist, perpetuating cycles of disadvantage for vulnerable infants.
Comparing outcomes across racial groups reveals stark inequalities. While the overall U.S. rate of FASDs is estimated at 1-5 per 100 live births, rates among Native American populations can soar to 20-50 per 1,000. This discrepancy underscores the failure of one-size-fits-all prevention strategies. Instead, programs should tailor messaging to specific communities. For instance, campaigns in Native American communities might incorporate traditional storytelling or involve tribal leaders to increase trust and relevance. Similarly, initiatives in African American communities could partner with churches or local organizations to disseminate information effectively.
Finally, practical steps can empower families to reduce risks. Pregnant individuals should be advised to avoid all alcohol, as no safe threshold exists. Partners and family members can support this by modeling abstinence during pregnancy. Healthcare providers must also educate patients about the risks of binge drinking, defined as 4 or more drinks in 2 hours for women, which poses a particularly high risk to fetal development. For those struggling with alcohol dependence, providers should offer referrals to specialized treatment programs that accommodate pregnant women. By combining individual action with systemic support, we can begin to close the health disparity gap for America’s most vulnerable infants.
Understanding Retinol: The Alcohol Derivative of Vitamin A Explained
You may want to see also
Frequently asked questions
American infants, like all infants, should never be exposed to alcohol. Their bodies are not equipped to process alcohol, and even small amounts can be toxic, leading to serious health risks or developmental issues.
In the U.S., it is widely understood and recommended that infants should not consume alcohol. Cultural practices do not typically involve giving alcohol to infants, as it is considered harmful and unsafe.
The metabolism of alcohol in infants is consistent across all populations, including American infants. Their livers are underdeveloped and cannot process alcohol effectively, making it dangerous regardless of geographic location.
No, there are no traditional or cultural practices in America that involve giving alcohol to infants. Such practices are strongly discouraged by medical professionals and public health guidelines.