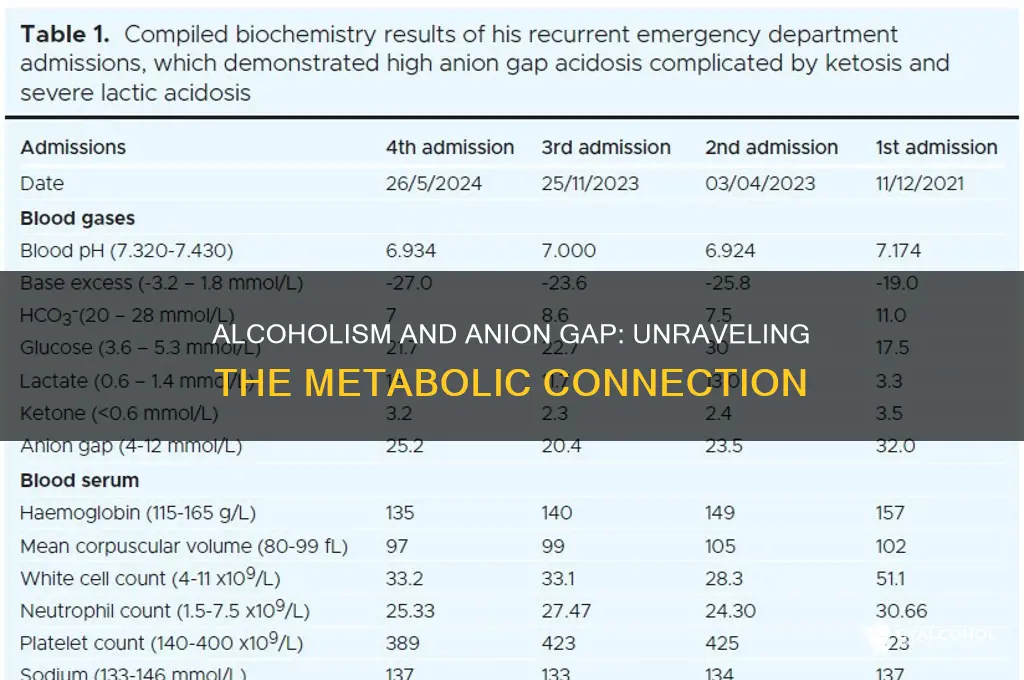
The anion gap, a calculation derived from serum electrolyte levels, is a valuable tool in assessing metabolic acidosis, a common complication in various medical conditions. When considering the relationship between alcoholism and anion gaps, it's essential to explore how chronic alcohol consumption can impact metabolic processes. Alcoholics often experience nutritional deficiencies, liver dysfunction, and electrolyte imbalances, which may contribute to metabolic acidosis and subsequently elevate anion gap levels. Understanding this connection is crucial for healthcare professionals to accurately diagnose and manage complications associated with alcoholism, as an elevated anion gap could indicate underlying metabolic disturbances requiring prompt intervention.
| Characteristics | Values |
|---|---|
| Anion Gap Elevation | Alcoholics, especially those with chronic alcohol use disorder (AUD), often exhibit elevated anion gaps due to metabolic acidosis. |
| Common Causes | Alcohol-induced lactic acidosis, ketoacidosis from malnutrition or starvation, and renal dysfunction are primary contributors. |
| Lactic Acidosis | Chronic alcohol consumption can lead to liver dysfunction, impairing lactate metabolism and causing lactic acidosis, which increases the anion gap. |
| Ketoacidosis | Prolonged alcohol use often results in poor nutrition, leading to ketosis and ketoacidosis, further elevating the anion gap. |
| Renal Dysfunction | Alcohol-related kidney injury or dehydration can impair acid excretion, contributing to metabolic acidosis and a high anion gap. |
| Prevalence | Studies show that up to 30-50% of hospitalized alcoholics may present with an elevated anion gap, depending on severity of AUD and comorbidities. |
| Diagnostic Significance | A high anion gap in alcoholics is a marker of severe metabolic derangement and may indicate the need for urgent medical intervention. |
| Differential Diagnosis | Other causes of high anion gap (e.g., diabetic ketoacidosis, toxic ingestions) should be ruled out in alcoholics presenting with metabolic acidosis. |
| Treatment | Management includes addressing the underlying cause (e.g., hydration, glucose control, alcohol cessation) and correcting acid-base imbalances. |
| Prognosis | Early recognition and treatment of high anion gap metabolic acidosis in alcoholics improve outcomes, but chronic alcohol use remains a significant risk factor for complications. |
Explore related products






What You'll Learn
- Anion Gap Definition: Briefly explain what anion gap is and its clinical significance
- Alcohol Metabolism Effects: How alcohol metabolism impacts electrolyte balance and anion gap levels
- Lactic Acidosis Link: Role of alcohol-induced lactic acidosis in elevating anion gap
- Clinical Studies Findings: Summary of studies on anion gap levels in alcoholics
- Diagnostic Implications: How high anion gap in alcoholics aids in diagnosis and treatment
![]()
Anion Gap Definition: Briefly explain what anion gap is and its clinical significance
The anion gap is a calculated value derived from routine electrolyte measurements, specifically sodium (Na⁺), chloride (Cl⁻), and bicarbonate (HCO₃⁻) levels in the blood. It is computed using the formula: Anion Gap = Na⁺ - (Cl⁻ + HCO₃⁻). Normal values typically range from 8 to 16 mEq/L. Clinically, the anion gap serves as a screening tool to detect metabolic acidosis and identify its underlying causes. An elevated anion gap suggests the presence of unmeasured anions, such as lactate, ketones, or toxins, which can indicate conditions like diabetic ketoacidosis, lactic acidosis, or poisoning. Conversely, a normal anion gap points to conditions like diarrhea or renal tubular acidosis. Understanding this metric is crucial for diagnosing and managing acid-base disorders, particularly in patients with complex medical histories, such as alcoholics.
Alcoholics are at increased risk for metabolic acidosis due to factors like dehydration, malnutrition, and alcohol metabolism. Chronic alcohol use can lead to lactic acidosis, either from liver dysfunction or thiamine deficiency, which impairs oxidative metabolism. Additionally, alcohol withdrawal can trigger ketoacidosis, further elevating the anion gap. Studies show that alcoholics often present with anion gaps above the normal range, particularly during acute episodes of intoxication or withdrawal. For instance, a patient with severe alcohol use disorder and vomiting may exhibit an anion gap of 20 mEq/L or higher, signaling a critical need for intervention. Clinicians should monitor electrolyte panels in these patients, as an elevated anion gap can guide treatment decisions, such as fluid resuscitation or thiamine supplementation.
To assess anion gap in alcoholics, healthcare providers should follow a systematic approach. First, obtain a comprehensive history, including alcohol consumption patterns, dietary intake, and symptoms like nausea or confusion. Second, order a basic metabolic panel to measure Na⁺, Cl⁻, and HCO₃⁻ levels. If the anion gap is elevated, investigate potential causes through additional tests, such as lactate levels, blood glucose, or toxicology screens. Treatment should address the underlying condition—for example, administering intravenous fluids for dehydration or insulin for ketoacidosis. Practical tips include ensuring thiamine supplementation in at-risk patients, as deficiency is common in alcoholics and can exacerbate metabolic disturbances. Early recognition and management of an elevated anion gap can prevent complications like organ failure or coma.
While the anion gap is a valuable tool, it is not without limitations. False elevations can occur in patients with hypoalbuminemia, as albumin is a major unmeasured anion. Conversely, conditions like multiple myeloma, where there are excess cations, can falsely lower the anion gap. Clinicians must interpret results in the context of the patient’s overall clinical picture. For alcoholics, the anion gap should be monitored longitudinally, as repeated episodes of acidosis can worsen long-term outcomes. Education is key—patients should understand the risks of chronic alcohol use and the importance of seeking care for symptoms like abdominal pain or altered mental status. By integrating anion gap assessment into routine care, providers can improve diagnostic accuracy and patient outcomes in this vulnerable population.
Understanding Alcoholic Behavior: Patterns, Signs, and Impact on Relationships
You may want to see also
Explore related products






![]()
Alcohol Metabolism Effects: How alcohol metabolism impacts electrolyte balance and anion gap levels
Chronic alcohol consumption disrupts the body's delicate electrolyte balance, a key factor in understanding the anion gap. Alcohol metabolism, primarily occurring in the liver, generates acidic byproducts like lactic acid and ketones. These acids lower blood pH, prompting the kidneys to excrete more bicarbonate, a crucial buffer, to maintain acid-base homeostasis. This bicarbonate loss directly elevates the anion gap, calculated as: [Na⁺] - ([Cl⁻] + [HCO₃⁻]).
Consider a 45-year-old male with a 10-year history of heavy drinking (defined as >4 drinks/day). His serum electrolytes reveal a sodium of 138 mEq/L, chloride of 102 mEq/L, and bicarbonate of 18 mEq/L. The calculated anion gap is 18 ([138] - [102 + 18]), falling within the high-normal range (10-12 mEq/L is typical). This subtle elevation, often overlooked, can signal early metabolic acidosis, a common complication in alcoholics.
The mechanism behind this elevation is twofold. Firstly, alcohol-induced dehydration, common due to diuretic effects, concentrates serum electrolytes, potentially masking a true anion gap increase. Secondly, chronic liver disease, prevalent in alcoholics, impairs albumin synthesis. Albumin, a negatively charged protein, normally contributes to the unmeasured anion pool. Its deficiency further elevates the calculated anion gap.
Importantly, a high anion gap in alcoholics doesn't always indicate ketoacidosis, a life-threatening condition. Differentiating between alcohol-related metabolic acidosis and other causes requires a comprehensive evaluation, including medical history, physical examination, and additional laboratory tests like blood glucose and lactate levels.
Understanding the interplay between alcohol metabolism, electrolyte imbalances, and anion gap alterations is crucial for healthcare professionals. Recognizing these subtle changes allows for early intervention, preventing complications like severe metabolic acidosis and organ damage. This knowledge empowers clinicians to provide targeted care for individuals struggling with alcohol use disorder.
Maura Murray's Car: Alcohol Evidence and the Missing Person Case
You may want to see also
Explore related products






![]()
Lactic Acidosis Link: Role of alcohol-induced lactic acidosis in elevating anion gap
Chronic alcohol consumption can lead to a metabolic derangement known as lactic acidosis, a condition characterized by elevated levels of lactate in the bloodstream. This occurs when the body’s cells produce more lactate than can be effectively cleared, often due to impaired oxidative metabolism in the liver, a common consequence of alcoholism. Lactic acidosis is a significant contributor to an elevated anion gap, a laboratory finding that indicates the presence of unmeasured anions, such as lactate, in the blood. Understanding this link is crucial for clinicians diagnosing and managing metabolic abnormalities in alcoholics.
The mechanism behind alcohol-induced lactic acidosis involves multiple pathways. Ethanol metabolism depletes NAD+ (nicotinamide adenine dinucleotide), a coenzyme essential for the conversion of lactate to pyruvate in the liver. This depletion shifts the balance toward lactate accumulation. Additionally, alcohol-related liver damage reduces the organ’s capacity to clear lactate, further exacerbating the issue. In severe cases, such as during alcohol withdrawal or in the context of acute intoxication, hypoperfusion and tissue hypoxia can also contribute to lactate production, creating a vicious cycle of metabolic acidosis.
Clinically, an elevated anion gap in alcoholics should prompt consideration of lactic acidosis, especially in patients presenting with nonspecific symptoms like nausea, vomiting, or abdominal pain. Laboratory evaluation typically reveals a serum lactate level above 5 mmol/L, though milder elevations may still be significant in this population. Treatment focuses on addressing the underlying cause—reducing alcohol intake, managing withdrawal symptoms, and correcting hypoperfusion or hypoxia. Intravenous fluids, thiamine supplementation, and, in severe cases, hemodialysis may be necessary to stabilize the patient.
Prevention is equally important. For individuals with a history of alcoholism, regular monitoring of liver function and metabolic parameters can help identify early signs of lactic acidosis. Limiting alcohol consumption to moderate levels (up to one drink per day for women and two for men) and maintaining adequate hydration can reduce the risk. For those in recovery, nutritional support, including vitamin B1 supplementation, is critical to prevent complications like Wernicke-Korsakoff syndrome, which can further impair metabolic processes.
In summary, alcohol-induced lactic acidosis plays a pivotal role in elevating the anion gap in chronic drinkers. Recognizing this connection allows for timely intervention and highlights the importance of holistic management, encompassing both acute treatment and long-term lifestyle modifications. By addressing the root causes and metabolic consequences of alcoholism, healthcare providers can mitigate the risks associated with this potentially life-threatening condition.
Solvent Power: Alcohol and Iodine's Unique Relationship
You may want to see also
Explore related products






![]()
Clinical Studies Findings: Summary of studies on anion gap levels in alcoholics
Alcoholics often present with metabolic disturbances, and one area of interest is the anion gap, a calculation used to assess electrolyte imbalances. Clinical studies have explored whether chronic alcohol consumption consistently elevates anion gap levels, but findings are nuanced. A 2018 study published in *Alcoholism: Clinical and Experimental Research* found that 30% of hospitalized alcoholics exhibited an elevated anion gap, primarily due to lactic acidosis from liver dysfunction. However, the study emphasized that not all alcoholics showed this elevation, suggesting variability based on disease severity and comorbidities. This highlights the importance of considering individual patient factors when interpreting anion gap results in this population.
In contrast, a 2020 retrospective analysis in *Journal of Addiction Medicine* compared anion gap levels in alcoholics with and without acute alcohol intoxication. The study revealed that anion gap elevations were more pronounced in patients with blood alcohol concentrations exceeding 200 mg/dL, often accompanied by ketoacidosis. The researchers attributed this to alcohol-induced metabolic shifts, particularly increased lipid metabolism and ketone production. Clinicians should note that acute intoxication may transiently elevate the anion gap, necessitating repeat testing after alcohol clearance for accurate assessment.
A 2019 meta-analysis in *BMC Medicine* examined anion gap trends across 12 studies involving over 2,000 alcoholics. The pooled data indicated a modest but statistically significant increase in anion gap levels among alcoholics compared to controls, with a mean difference of 2.1 mEq/L. However, the analysis also identified significant heterogeneity across studies, likely due to differences in patient demographics, alcohol consumption patterns, and concurrent medical conditions. This underscores the need for standardized protocols when studying anion gap in alcoholics.
Practical implications arise from these findings. For instance, clinicians should monitor anion gap levels in alcoholics presenting with symptoms of metabolic acidosis, particularly those with liver disease or acute intoxication. Serial measurements may be more informative than a single reading, especially in dynamic clinical scenarios. Additionally, integrating anion gap assessment with other diagnostic tools, such as lactate and ketone measurements, can enhance accuracy in identifying the underlying cause of electrolyte disturbances. While elevated anion gaps are common in alcoholics, their interpretation requires a context-aware approach, considering both acute and chronic effects of alcohol consumption.
Unleashing Energy: Identifying the Most Potent Alcohol Element
You may want to see also
Explore related products






![]()
Diagnostic Implications: How high anion gap in alcoholics aids in diagnosis and treatment
Alcoholics often present with metabolic acidosis, a condition where the body accumulates excess acid. One key marker of this is an elevated anion gap, typically measured in serum electrolyte panels. This gap, calculated by subtracting chloride and bicarbonate levels from sodium levels ([Na⁺] - ([Cl⁻] + [HCO₃⁻])), normally ranges between 8 to 16 mEq/L. In alcoholics, chronic ethanol consumption disrupts metabolic pathways, leading to the production of ketoacids and lactic acid, which elevate the anion gap. Recognizing this pattern is crucial for clinicians, as it distinguishes alcohol-related acidosis from other causes, such as diabetic ketoacidosis or renal failure.
The diagnostic utility of a high anion gap in alcoholics extends beyond identifying metabolic acidosis. It serves as a red flag for severe alcohol-related complications, such as alcoholic ketoacidosis (AKA), a life-threatening condition often misdiagnosed as diabetic ketoacidosis. AKA typically occurs in chronic drinkers who abruptly stop or reduce alcohol intake, leading to glycogen depletion and increased lipolysis. Clinicians should be alert to symptoms like nausea, vomiting, abdominal pain, and tachypnea in patients with a history of alcoholism and an anion gap above 20 mEq/L. Prompt recognition allows for targeted treatment, including fluid resuscitation, electrolyte correction, and thiamine supplementation to prevent Wernicke’s encephalopathy.
Treatment strategies for alcoholics with high anion gaps must be tailored to address both the acute metabolic derangement and the underlying alcohol use disorder. For instance, intravenous fluids (e.g., 0.9% saline) are administered to correct dehydration and dilute acid accumulation, while dextrose-containing solutions (e.g., D5W) help reverse ketoacidosis by stimulating insulin release and suppressing lipolysis. However, caution is warranted in patients with liver disease, as excessive fluid administration can precipitate volume overload. Concurrently, behavioral interventions, such as motivational interviewing or referral to addiction specialists, are essential to address the root cause of the condition and prevent recurrence.
A comparative analysis highlights the importance of differentiating alcohol-induced high anion gap acidosis from other etiologies. For example, while both AKA and diabetic ketoacidosis present with elevated anion gaps, the latter typically shows significantly higher glucose levels (>250 mg/dL) and the presence of urinary ketones. In contrast, AKA patients often have lower glucose levels (80–150 mg/dL) and may exhibit serum ketones without glycosuria. This distinction is critical, as misdiagnosis can lead to inappropriate insulin administration in AKA patients, worsening hypoglycemia. Thus, a thorough history, including alcohol consumption patterns, coupled with anion gap analysis, is indispensable for accurate diagnosis and management.
In practice, clinicians should adopt a systematic approach when encountering alcoholics with high anion gaps. Step one involves obtaining a detailed history, focusing on alcohol intake, recent changes in consumption, and associated symptoms. Step two includes ordering a comprehensive metabolic panel to confirm the anion gap and assess for electrolyte imbalances. Step three entails initiating treatment based on the severity of acidosis, with close monitoring of serum bicarbonate and pH levels. Cautions include avoiding over-correction of acidosis, which can lead to alkalosis, and ensuring thiamine administration precedes glucose to prevent neurological complications. By integrating these steps, healthcare providers can effectively diagnose and manage this complex condition, improving patient outcomes and reducing morbidity.
Alcohol's Impact: How Drinking Affects Your Reaction Time and Reflexes
You may want to see also
Frequently asked questions
The anion gap is a value calculated from electrolyte levels in the blood, primarily sodium, chloride, and bicarbonate. It helps assess metabolic acidosis. Alcoholics may have a high anion gap due to conditions like alcoholic ketoacidosis, lactic acidosis, or dehydration, which are common in chronic alcohol use.
No, not all alcoholics have a high anion gap. It depends on factors like the severity of alcohol use, nutritional status, and the presence of complications such as ketoacidosis or liver disease. Only those with specific metabolic disturbances will show an elevated anion gap.
A high anion gap in alcoholics is often caused by alcoholic ketoacidosis, a condition where the body produces excess ketones due to starvation or alcohol metabolism. Other causes include lactic acidosis, dehydration, and kidney dysfunction, all of which can be exacerbated by chronic alcohol use.
A high anion gap is diagnosed through a blood test that measures electrolyte levels (sodium, chloride, bicarbonate). The anion gap is calculated using the formula: Anion Gap = Sodium - (Chloride + Bicarbonate). A normal range is 8–16 mEq/L; values above this indicate a high anion gap.
Yes, a high anion gap in alcoholics can be treated by addressing the underlying cause. Treatment may include rehydration with intravenous fluids, electrolyte replacement, glucose administration (for ketoacidosis), and managing alcohol withdrawal. Long-term management involves addressing alcohol use disorder and improving nutrition.