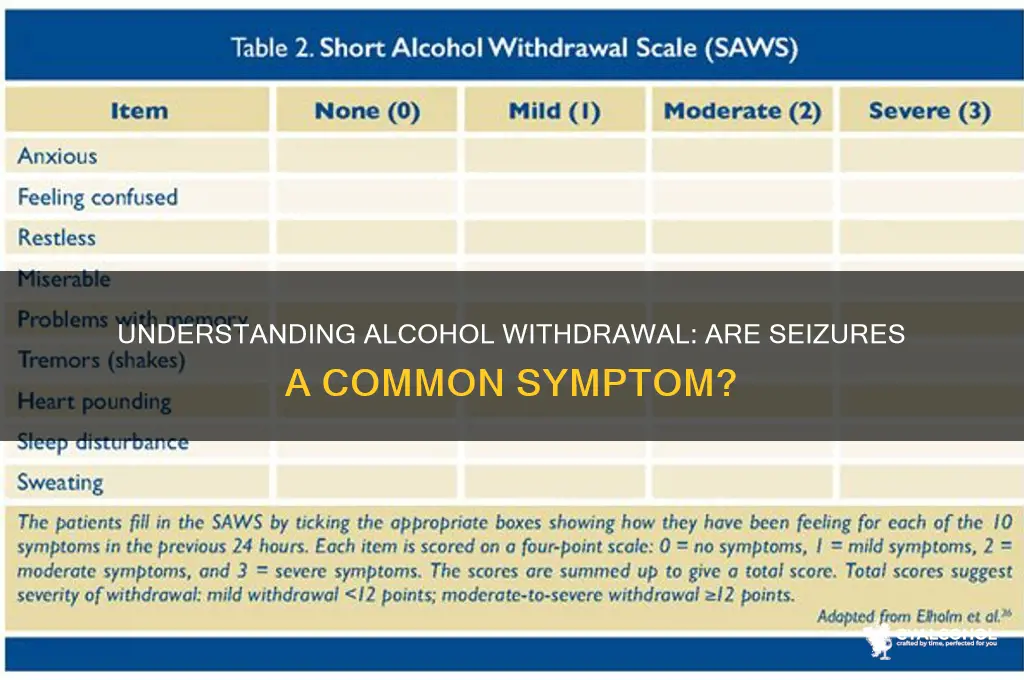
Alcohol withdrawal is a serious and potentially life-threatening condition that occurs when individuals who have been drinking heavily for extended periods suddenly stop or significantly reduce their alcohol intake. One of the most concerning complications of alcohol withdrawal is the occurrence of seizures, which can arise within the first 48 hours after cessation. These seizures, often referred to as withdrawal seizures, are a hallmark of severe alcohol withdrawal syndrome and are estimated to affect approximately 5-10% of individuals undergoing withdrawal. The risk of seizures is particularly high in those with a history of prolonged and heavy alcohol use, as well as in individuals who have experienced previous withdrawal episodes. Understanding the prevalence and risk factors associated with seizures during alcohol withdrawal is crucial for timely intervention and management, as prompt medical treatment can significantly reduce the risk of complications and improve outcomes.
| Characteristics | Values |
|---|---|
| Prevalence of Seizures in Alcohol Withdrawal | Approximately 5-10% of individuals experiencing alcohol withdrawal develop seizures. |
| Timing of Seizures | Typically occur within 6 to 48 hours after the last drink, peaking at 24-36 hours. |
| Type of Seizures | Most commonly generalized tonic-clonic seizures (grand mal seizures). |
| Risk Factors | Prior history of withdrawal seizures, heavy and prolonged alcohol use, concurrent medical conditions, and electrolyte imbalances. |
| Mechanism | Results from abrupt cessation of alcohol, leading to increased neuronal excitability due to GABA receptor downregulation and NMDA receptor upregulation. |
| Prognosis | Usually self-limiting, but recurrent seizures can occur. Mortality is low but increases with complications like aspiration pneumonia or head injury. |
| Treatment | Benzodiazepines (e.g., diazepam, lorazepam) are the first-line treatment to prevent and manage seizures. Anticonvulsants may be used in refractory cases. |
| Prevention | Gradual tapering of alcohol under medical supervision, hydration, and electrolyte correction can reduce seizure risk. |
| Associated Conditions | Often accompanied by other withdrawal symptoms like tremors, anxiety, hallucinations, and delirium tremens (DTs). |
| Long-Term Implications | Recurrent seizures may indicate a higher risk of developing epilepsy or other neurological complications. |
Explore related products






What You'll Learn
- Seizure Risk Factors: High alcohol use, sudden cessation, and personal/family history increase seizure likelihood
- Timeline of Seizures: Typically occur 6-48 hours after last drink during acute withdrawal phase
- Types of Seizures: Most common are generalized tonic-clonic seizures, lasting 1-3 minutes
- Prevention Strategies: Gradual tapering, medical supervision, and benzodiazepines reduce seizure risk significantly
- Treatment Options: Immediate medical intervention, anticonvulsants, and hydration are critical for management
![]()
Seizure Risk Factors: High alcohol use, sudden cessation, and personal/family history increase seizure likelihood
Alcohol withdrawal seizures are a stark reminder of the body's delicate balance, disrupted by prolonged and heavy drinking. These seizures, typically occurring within 6 to 48 hours after the last drink, are a direct consequence of the brain's attempt to recalibrate its chemistry. The risk escalates with the amount and duration of alcohol consumption. For instance, individuals who consume more than 15 standard drinks per day (equivalent to about 12 ounces of regular beer, 5 ounces of wine, or 1.5 ounces of distilled spirits) for several weeks are at a significantly higher risk. This high alcohol intake alters the brain's GABA and glutamate systems, creating a dependency that, when abruptly halted, can lead to hyperexcitability and seizures.
Sudden cessation of alcohol, often in an attempt to quit cold turkey, is a critical risk factor for seizures. The brain, accustomed to the depressant effects of alcohol, struggles to adapt when the substance is removed. This abrupt change can trigger a rebound effect, causing neuronal hyperactivity. Detoxification should ideally be a gradual process, especially for heavy drinkers. Tapering off alcohol under medical supervision can reduce the risk of seizures and other severe withdrawal symptoms. For example, a supervised detox program might start by reducing daily intake by 10-20% every few days, accompanied by medications like benzodiazepines to manage withdrawal symptoms safely.
Personal and family history of seizures or epilepsy further compound the risk during alcohol withdrawal. Genetic predispositions can lower the seizure threshold, making individuals more susceptible. Studies show that a family history of seizures increases the likelihood of alcohol withdrawal seizures by up to 30%. Similarly, individuals with a personal history of seizures, whether alcohol-related or not, are at heightened risk. This underscores the importance of disclosing medical history to healthcare providers when seeking treatment for alcohol dependence. Tailored interventions, such as lower tapering rates or prophylactic anticonvulsant medications, can be implemented to mitigate risks.
Practical steps can be taken to minimize seizure risk during alcohol withdrawal. First, avoid quitting alcohol abruptly if you’ve been a heavy drinker. Instead, consult a healthcare professional to devise a safe tapering plan. Second, monitor for early withdrawal symptoms like tremors, anxiety, or insomnia, as these can precede seizures. Third, stay hydrated and maintain electrolyte balance, as dehydration can exacerbate neurological instability. Finally, consider joining support groups or seeking counseling to address the psychological aspects of alcohol dependence, which can indirectly reduce the risk of severe withdrawal complications.
In conclusion, understanding the interplay of high alcohol use, sudden cessation, and personal/family history is crucial for managing seizure risk during withdrawal. By adopting a proactive and informed approach, individuals can navigate the challenges of alcohol detoxification more safely, reducing the likelihood of seizures and other life-threatening complications.
Unveiling Europe's Historic Hallucinogenic Alcoholic Beverage: A Cultural Journey
You may want to see also
Explore related products






![]()
Timeline of Seizures: Typically occur 6-48 hours after last drink during acute withdrawal phase
Seizures during alcohol withdrawal are a critical concern, typically emerging within a specific timeframe: 6 to 48 hours after the last drink. This window falls squarely within the acute withdrawal phase, a period marked by the body’s abrupt readjustment to the absence of alcohol. Understanding this timeline is crucial for anyone managing or witnessing withdrawal, as seizures can escalate rapidly from a minor tremor to a life-threatening event.
Consider the mechanism at play: chronic alcohol use depresses the central nervous system, and sudden cessation triggers a rebound hyperexcitability. This neurological imbalance manifests as seizures, often beginning as myoclonic jerks or generalized tonic-clonic seizures. For individuals with a history of heavy drinking—defined as more than 15 drinks per week for men or 8 for women—the risk is exponentially higher. Age and overall health further modulate this risk, with older adults and those with pre-existing liver or neurological conditions being particularly vulnerable.
To mitigate risks during this critical 6-48 hour window, proactive monitoring is essential. Keep the individual in a safe environment, free of sharp objects or hard surfaces. If a seizure occurs, time its duration; anything exceeding five minutes warrants immediate medical attention, as prolonged seizures can lead to brain damage or death. Benzodiazepines, such as diazepam or lorazepam, are the first-line treatment, administered under medical supervision to stabilize the nervous system.
Comparatively, seizures during alcohol withdrawal differ from those in epilepsy or other neurological disorders. They are often self-limiting, resolving within the acute withdrawal phase, but their unpredictability demands vigilance. Unlike epileptic seizures, which may have identifiable triggers or patterns, alcohol withdrawal seizures are directly tied to the cessation timeline, making them both preventable and treatable with timely intervention.
In practical terms, anyone supporting someone through withdrawal should maintain a log of symptoms, noting the time of the last drink and any signs of agitation, tremors, or confusion. Hydration and electrolyte balance are critical, as dehydration can exacerbate neurological instability. Avoid caffeine and other stimulants, which can heighten anxiety and seizure risk. Finally, educate yourself on the signs of delirium tremens (DTs), a severe form of withdrawal that often accompanies seizures and requires hospitalization.
By recognizing the 6-48 hour seizure timeline and taking proactive steps, caregivers and individuals can navigate the acute withdrawal phase with greater safety and preparedness. This knowledge transforms a potentially chaotic experience into a manageable process, reducing the risk of complications and paving the way for recovery.
Alcohol and Belly Bloat: Quick Tips for Relief
You may want to see also
Explore related products






![]()
Types of Seizures: Most common are generalized tonic-clonic seizures, lasting 1-3 minutes
Seizures are a well-documented complication of alcohol withdrawal, particularly in individuals with a history of chronic, heavy drinking. Among the various types of seizures, generalized tonic-clonic seizures are the most common during this process, typically occurring within 6 to 48 hours after the last drink. These seizures are characterized by a sudden loss of consciousness, followed by stiffening of the body (tonic phase) and rhythmic jerking movements (clonic phase), lasting between 1 to 3 minutes. Understanding this specific type of seizure is crucial for recognizing and managing alcohol withdrawal effectively.
From an analytical perspective, the occurrence of generalized tonic-clonic seizures during alcohol withdrawal is linked to the brain’s attempt to regain equilibrium after prolonged exposure to alcohol. Chronic alcohol use suppresses neuronal activity, and abrupt cessation leads to a rebound excitation, often manifesting as seizures. Studies show that individuals who consume more than 15 standard drinks per day (for men) or 8 per day (for women) are at higher risk. Recognizing this mechanism underscores the importance of medically supervised detoxification, especially for heavy drinkers.
Practically speaking, if you or someone you know is experiencing alcohol withdrawal, it’s essential to monitor for signs of seizures, particularly within the first two days. Key indicators include sudden collapse, muscle rigidity, and convulsions. If a tonic-clonic seizure occurs, ensure the person’s safety by clearing the area of sharp objects, placing them on their side to prevent choking, and timing the seizure. Seizures lasting longer than 5 minutes or recurring without full recovery in between are medical emergencies requiring immediate intervention.
Comparatively, while other types of seizures, such as focal seizures, can occur during withdrawal, tonic-clonic seizures are more alarming due to their intensity and potential for complications like injury or aspiration. Unlike focal seizures, which may involve localized symptoms like twitching or confusion, tonic-clonic seizures are impossible to miss and demand immediate attention. This distinction highlights why medical professionals prioritize monitoring for this specific type during detoxification.
In conclusion, generalized tonic-clonic seizures are a hallmark of severe alcohol withdrawal, typically lasting 1 to 3 minutes and occurring within the first 48 hours of abstinence. Their prevalence among heavy drinkers underscores the need for proactive management, including medical supervision and education on seizure recognition. By understanding this specific type of seizure, individuals and caregivers can take critical steps to ensure safety and seek timely medical intervention when necessary.
Conquer Shyness Without Alcohol: Embrace Your True Self
You may want to see also
Explore related products





![]()
Prevention Strategies: Gradual tapering, medical supervision, and benzodiazepines reduce seizure risk significantly
Seizures are a significant risk during alcohol withdrawal, particularly in individuals with a history of heavy, prolonged drinking. The abrupt cessation of alcohol can lead to a hyperexcitable state in the brain, increasing the likelihood of seizures, which can be life-threatening. However, this risk is not inevitable. Strategic prevention measures, such as gradual tapering, medical supervision, and the use of benzodiazepines, can dramatically reduce the incidence of seizures, offering a safer path to recovery.
Gradual Tapering: A Controlled Approach
Tapering alcohol consumption rather than quitting abruptly is a cornerstone of seizure prevention. This method involves reducing alcohol intake in a structured, stepwise manner, typically over days to weeks. For example, a person consuming 20 drinks per day might decrease by 2–4 drinks daily, adjusting based on tolerance and withdrawal symptoms. Tapering allows the central nervous system to adapt slowly, minimizing the risk of hyperexcitability that triggers seizures. However, self-tapering requires discipline and honesty about consumption levels; underestimating intake can undermine the process. For heavy drinkers, tapering should ideally be guided by a healthcare professional to ensure safety and effectiveness.
Medical Supervision: Expert Oversight Matters
Withdrawal seizures are not just a physical challenge but a medical emergency. Professional supervision provides continuous monitoring of vital signs, symptom severity, and neurological status, enabling prompt intervention if seizures occur. Inpatient detox programs are often recommended for individuals at high risk, such as those with a history of withdrawal seizures, concurrent medical conditions, or severe alcohol dependence. Outpatient management, while possible for milder cases, requires strict adherence to a tapering plan and regular check-ins with a healthcare provider. Medical teams can also address complications like dehydration, electrolyte imbalances, or co-occurring infections that exacerbate seizure risk.
Benzodiazepines: The Gold Standard in Prevention
Benzodiazepines, such as diazepam, lorazepam, or chlordiazepoxide, are the first-line pharmacological agents for preventing alcohol withdrawal seizures. These medications modulate GABA receptors, counteracting the brain’s hyperexcitability during withdrawal. Dosing is tailored to the individual’s needs, often starting with a moderate dose (e.g., 10–20 mg of diazepam every 6–8 hours) and adjusted based on symptom severity. Long-acting benzodiazepines are preferred for their sustained effect, reducing the risk of breakthrough seizures. However, these drugs must be administered under medical supervision due to their potential for dependence and respiratory depression, particularly in older adults or those with liver impairment.
Practical Tips for Implementation
For those considering tapering at home, keep a detailed log of daily alcohol consumption and withdrawal symptoms to track progress and identify triggers. Stay hydrated and maintain a balanced diet to support overall health during the process. If opting for medical supervision, be transparent about your drinking history and any previous withdrawal experiences to guide treatment planning. When prescribed benzodiazepines, take them exactly as directed and avoid alcohol or other sedatives, which can potentiate their effects. Finally, have an emergency plan in place, including access to medical care, in case of severe withdrawal symptoms or seizures.
By combining gradual tapering, medical oversight, and benzodiazepine therapy, individuals can significantly reduce the risk of seizures during alcohol withdrawal. While the journey is challenging, these strategies provide a structured, evidence-based approach to safer detoxification, paving the way for long-term recovery.
Painkiller Safety: Alcohol with Tylenol or Hydrocodone?
You may want to see also
Explore related products






![]()
Treatment Options: Immediate medical intervention, anticonvulsants, and hydration are critical for management
Seizures are a severe and potentially life-threatening complication of alcohol withdrawal, occurring in approximately 5-10% of individuals undergoing detoxification. When they strike, immediate medical intervention is non-negotiable. Time is of the essence, as untreated seizures can lead to status epilepticus, a medical emergency with a high mortality rate. The first step is to ensure the individual’s airway, breathing, and circulation are stable, often requiring hospitalization. Benzodiazepines, such as diazepam or lorazepam, are the cornerstone of acute treatment, administered intravenously to rapidly control seizure activity. Dosages are titrated based on response, with continuous monitoring to prevent oversedation or respiratory depression. This swift action not only halts the seizure but also stabilizes the patient for further management.
Anticonvulsants play a pivotal role in preventing recurrent seizures during alcohol withdrawal. While benzodiazepines are the first-line treatment, adjunctive medications like carbamazepine, valproate, or phenytoin may be used in refractory cases or as prophylaxis. For instance, carbamazepine 200 mg every 6-8 hours has been shown to reduce seizure risk, though it requires careful monitoring for bone marrow suppression. Valproate, dosed at 15-30 mg/kg/day, is another option, particularly in patients with liver dysfunction. However, these medications are not without risks—hepatic toxicity, hematologic abnormalities, and drug interactions necessitate close supervision. Anticonvulsants should be initiated early in high-risk individuals, such as those with a history of withdrawal seizures or severe alcohol dependence, to mitigate the likelihood of recurrence.
Hydration and electrolyte balance are often overlooked but critical components of managing alcohol withdrawal seizures. Chronic alcohol use disrupts fluid and electrolyte homeostasis, leading to hypomagnesemia, hypokalemia, and dehydration—all of which lower the seizure threshold. Intravenous fluids, typically normal saline or lactated Ringer’s solution, are administered to correct dehydration and support organ function. Magnesium sulfate, dosed at 2-4 grams intravenously, is particularly effective in patients with hypomagnesemia, as magnesium deficiency is a known trigger for seizures. Oral electrolyte supplements may be used in milder cases, but severe imbalances require prompt intravenous correction. This simple yet vital intervention can prevent seizures and stabilize patients before more targeted therapies take effect.
In practice, the management of alcohol withdrawal seizures demands a multifaceted approach tailored to the individual’s needs. Immediate medical intervention, including benzodiazepines, is the first line of defense, while anticonvulsants provide a safety net for high-risk patients. Hydration and electrolyte correction address underlying metabolic derangements, reducing the risk of further seizures. For example, a 45-year-old man with a history of daily alcohol consumption and prior withdrawal seizures would benefit from hospitalization, lorazepam 2 mg IV for acute control, carbamazepine 200 mg three times daily for prophylaxis, and intravenous fluids with magnesium supplementation. This comprehensive strategy not only treats the immediate crisis but also lays the groundwork for long-term recovery, emphasizing the importance of early, evidence-based intervention.
Robitussin vs. Alcohol: Which Substance Poses Greater Health Risks?
You may want to see also
Frequently asked questions
Seizures are a potential complication of alcohol withdrawal, particularly in individuals with a history of heavy or prolonged alcohol use. They typically occur within 6 to 48 hours after the last drink but can happen up to 5 days later.
Individuals with a history of severe alcohol dependence, previous withdrawal seizures, or co-occurring medical conditions are at higher risk. Those who consume large amounts of alcohol daily or have a history of multiple withdrawal episodes are also more susceptible.
Yes, seizures can often be prevented with proper medical management. Medications such as benzodiazepines are commonly used to taper alcohol use and reduce the risk of withdrawal complications, including seizures.
Seizures during alcohol withdrawal are typically treated with benzodiazepines, such as diazepam or lorazepam, to control the seizure activity and prevent further episodes. Immediate medical attention is essential to ensure safety and proper care.
While not all seizures are life-threatening, they can be dangerous, especially if they occur repeatedly or lead to complications like injuries or aspiration. Prompt medical intervention is crucial to minimize risks and ensure a safe recovery.































