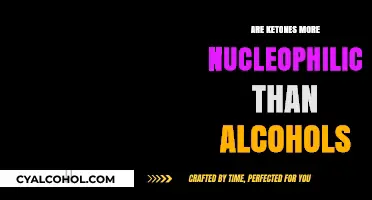
Heroin and alcohol withdrawal, though stemming from different substances, share striking similarities in their physical and psychological symptoms due to their impact on the central nervous system. Both substances create dependence by altering brain chemistry, leading to severe withdrawal effects when use is abruptly stopped. Common symptoms include anxiety, insomnia, nausea, sweating, and tremors, with more severe cases involving seizures or hallucinations. However, the intensity and duration of withdrawal can differ; heroin withdrawal often peaks within 24–48 hours and lasts 5–10 days, while alcohol withdrawal may escalate to life-threatening delirium tremens within 48–72 hours. Despite these differences, both conditions require medical supervision and tailored treatment to manage symptoms and prevent complications, highlighting the complex nature of addiction and recovery.
Explore related products





What You'll Learn
- Symptoms Comparison: Physical vs. psychological symptoms of heroin and alcohol withdrawal
- Timeline Differences: Duration and intensity of withdrawal for both substances
- Medical Risks: Potential health complications during heroin and alcohol detox
- Treatment Approaches: Medications and therapies used for each withdrawal type
- Relapse Factors: Common triggers for relapse in heroin and alcohol withdrawal
![]()
Symptoms Comparison: Physical vs. psychological symptoms of heroin and alcohol withdrawal
Heroin and alcohol withdrawal share some striking similarities, yet their symptoms diverge in ways that demand tailored approaches to management. Both substances, when abruptly discontinued, unleash a cascade of physical and psychological challenges, but the intensity and nature of these symptoms vary significantly. Understanding these differences is crucial for anyone navigating the complexities of withdrawal, whether personally or in supporting a loved one.
Physical Symptoms: A Battle of the Body
Heroin withdrawal is notorious for its severe physical symptoms, which often begin within 6–12 hours of the last dose. Users may experience muscle aches, sweating, nausea, vomiting, and diarrhea. The body’s dependence on opioids creates a heightened sensitivity to pain, making even minor discomfort feel unbearable. Alcohol withdrawal, on the other hand, typically starts 6–24 hours after the last drink, with symptoms like tremors, rapid heartbeat, and high blood pressure. In severe cases, alcohol withdrawal can lead to delirium tremens (DTs), a life-threatening condition characterized by seizures, confusion, and fever. While both substances cause profound physical distress, alcohol withdrawal poses a higher risk of fatal complications, especially without medical supervision.
Psychological Symptoms: The Mind’s Struggle
Psychologically, heroin withdrawal manifests as intense cravings, anxiety, and depression. The brain’s reward system, hijacked by prolonged opioid use, struggles to function without the drug, leading to profound emotional turmoil. Users often describe feeling a deep sense of emptiness or hopelessness, which can persist for weeks. Alcohol withdrawal, meanwhile, triggers anxiety, irritability, and mood swings. In severe cases, hallucinations and paranoia may occur, particularly during DTs. While both substances induce psychological distress, heroin withdrawal tends to focus on cravings and emotional voids, whereas alcohol withdrawal often includes more acute psychotic features.
Practical Tips for Managing Symptoms
For heroin withdrawal, gradual tapering under medical supervision can reduce physical discomfort, though this approach is rarely feasible for those seeking immediate cessation. Medications like methadone or buprenorphine can alleviate symptoms and cravings, while over-the-counter remedies like ibuprofen may help with muscle aches. Staying hydrated and consuming small, frequent meals can ease gastrointestinal distress. For alcohol withdrawal, medical detox is essential, especially for heavy drinkers (defined as more than 15 drinks per week for men or 8 for women). Benzodiazepines are commonly prescribed to prevent seizures and manage anxiety. Avoiding caffeine and maintaining a calm environment can also reduce psychological agitation.
Takeaway: Context Matters
While heroin and alcohol withdrawal share commonalities, such as anxiety and physical discomfort, their distinct profiles require individualized care. Heroin withdrawal is more protracted and emotionally draining, while alcohol withdrawal carries a higher risk of medical emergencies. Recognizing these differences empowers individuals and caregivers to seek appropriate treatment, whether through medication-assisted therapy, inpatient detox, or supportive care. Ultimately, both journeys demand compassion, patience, and a commitment to long-term recovery.
Cu-Zn's Role in Alcohol Formation Explained
You may want to see also
Explore related products






![]()
Timeline Differences: Duration and intensity of withdrawal for both substances
Heroin withdrawal typically begins within 6 to 12 hours after the last dose, peaking in intensity between 24 and 48 hours. Symptoms include muscle aches, insomnia, diarrhea, and intense cravings. The acute phase lasts about 5 to 7 days, though psychological symptoms like anxiety and depression can persist for weeks. For heavy users (those consuming 1-2 grams daily), the timeline may extend, with physical symptoms lingering up to 10 days. Protracted withdrawal, marked by fatigue and mood swings, can last months without treatment.
Alcohol withdrawal, in contrast, starts 6 to 24 hours after the last drink, depending on the individual’s tolerance and consumption level. For moderate drinkers (3-4 drinks daily), mild symptoms like tremors and anxiety emerge first. Heavy drinkers (6+ drinks daily) face a more severe timeline, with hallucinations appearing within 12-24 hours and seizures or delirium tremens (DTs) possible after 48 hours. The acute phase lasts 5-7 days, but post-acute withdrawal syndrome (PAWS), characterized by insomnia and irritability, can persist for months. Unlike heroin, alcohol withdrawal carries a higher risk of life-threatening complications, especially in long-term users.
Comparing the two, heroin withdrawal is often described as more physically agonizing but less medically dangerous than alcohol withdrawal. Heroin’s timeline is more predictable, with symptoms peaking early and subsiding within a week. Alcohol withdrawal, however, escalates rapidly and unpredictably, particularly in heavy users. For instance, DTs occur in 3-5% of alcohol withdrawal cases, requiring immediate medical intervention. Heroin users can often manage withdrawal with medications like methadone or buprenorphine, while alcohol withdrawal frequently demands hospitalization for benzodiazepines and hydration support.
Practical tips for managing these timelines differ. Heroin users should seek medication-assisted treatment (MAT) early to ease cravings and physical discomfort. Over-the-counter pain relievers and hydration can help manage minor symptoms. For alcohol withdrawal, tapering under medical supervision is safer than quitting cold turkey, especially for heavy drinkers. Home management is risky; instead, inpatient care with benzodiazepines and monitoring for seizures is recommended. Both groups benefit from counseling and support groups, but alcohol users must prioritize medical oversight due to the higher risk of complications.
In summary, while both heroin and alcohol withdrawal share symptoms like anxiety and insomnia, their timelines and risks diverge sharply. Heroin withdrawal is shorter and more physically intense but less life-threatening, whereas alcohol withdrawal is longer, more unpredictable, and carries higher medical risks. Understanding these differences is crucial for tailoring treatment strategies and ensuring safety during detoxification.
Safely Cutting Back: A Guide to Reducing Alcohol Intake
You may want to see also
Explore related products






![]()
Medical Risks: Potential health complications during heroin and alcohol detox
Heroin and alcohol withdrawal share some similarities, but the medical risks during detox can vary significantly, making it crucial to understand the unique challenges each presents. Both substances lead to physical dependence, and abrupt cessation triggers withdrawal symptoms, yet the intensity and nature of these symptoms differ, as do the potential health complications.
The Cardiovascular Strain: A Hidden Danger
Alcohol withdrawal, particularly in chronic users, can induce severe complications like delirium tremens (DTs), characterized by hallucinations, seizures, and rapid heart rate. For instance, a 40-year-old with a decade-long alcohol dependency faces a 5-10% risk of DTs, which can be fatal without medical intervention. Heroin withdrawal, while less likely to cause seizures, often leads to severe dehydration and electrolyte imbalances due to vomiting and diarrhea. This can result in hypovolemia, a condition where blood volume decreases, straining the cardiovascular system. For someone detoxing from heroin, oral rehydration solutions with electrolytes (e.g., 1 liter of water with 6 teaspoons of sugar and ½ teaspoon of salt) can mitigate this risk, but medical monitoring is essential.
Neurological Risks: Seizures and Beyond
Alcohol withdrawal poses a higher risk of seizures, especially within 48 hours of the last drink. Benzodiazepines like diazepam are often prescribed to taper alcohol use, reducing seizure risk by stabilizing GABA receptors in the brain. Heroin withdrawal, on the other hand, primarily affects the brain’s opioid receptors, leading to symptoms like anxiety, insomnia, and muscle aches. While seizures are rare, the psychological distress can exacerbate underlying conditions like hypertension or heart disease. For example, a 25-year-old heroin user with undiagnosed high blood pressure may experience a hypertensive crisis during detox, requiring immediate medical attention.
Psychological Complications: The Overlooked Threat
Both detox processes can trigger severe psychological distress, but the nature of this distress differs. Alcohol withdrawal often causes anxiety and depression, which can persist for weeks. Heroin withdrawal, however, is notorious for its intense cravings and dysphoria, increasing the risk of relapse. A 30-year-old with a history of depression may experience suicidal ideation during heroin detox, necessitating psychiatric support. Cognitive-behavioral therapy (CBT) and medications like buprenorphine can reduce cravings and stabilize mood, but these interventions must be tailored to the individual’s history and needs.
Practical Tips for Safer Detox
Detoxing from heroin or alcohol should never be attempted alone. Medical supervision is critical, especially for those with co-occurring conditions like liver disease or cardiovascular issues. For alcohol detox, tapering with a benzodiazepine under a doctor’s guidance reduces the risk of DTs. Heroin detox benefits from medications like methadone or buprenorphine, which ease withdrawal symptoms and reduce relapse risk. Additionally, maintaining a balanced diet, staying hydrated, and engaging in light physical activity (e.g., walking for 20 minutes daily) can support the body’s recovery. Always consult a healthcare provider to create a personalized detox plan, as self-managed detox can lead to life-threatening complications.
In summary, while heroin and alcohol withdrawal share commonalities, their medical risks during detox are distinct. Understanding these differences ensures safer, more effective treatment, emphasizing the need for individualized care and professional oversight.
Alcohol and Baking Soda: Unveiling Their Surprising Chemical Reaction
You may want to see also
Explore related products






![]()
Treatment Approaches: Medications and therapies used for each withdrawal type
Heroin and alcohol withdrawal, though distinct in their mechanisms, share a critical need for tailored treatment approaches to manage symptoms and prevent relapse. Medications and therapies play pivotal roles in both, yet their applications differ significantly based on the substance and the individual’s needs.
For heroin withdrawal, medications like methadone, buprenorphine, and naltrexone are cornerstone treatments. Methadone, a long-acting opioid agonist, is often administered in doses ranging from 20 to 120 mg daily, depending on the severity of dependence. Buprenorphine, a partial opioid agonist, is typically started at 4–8 mg sublingually on the first day, with maintenance doses up to 24 mg daily. Naltrexone, an opioid antagonist, is used after detoxification, with a standard dose of 50 mg daily. These medications stabilize brain chemistry, reduce cravings, and prevent relapse. Behavioral therapies, such as cognitive-behavioral therapy (CBT) and contingency management, complement pharmacotherapy by addressing psychological triggers and reinforcing abstinence.
Alcohol withdrawal, on the other hand, relies on benzodiazepines as the primary medication. Chlordiazepoxide (Librium) and diazepam (Valium) are commonly used, with dosing tailored to the severity of withdrawal. For mild symptoms, 10–20 mg of chlordiazepoxide every 6 hours may suffice, while severe cases may require up to 100 mg every 6 hours. These medications mitigate the risk of seizures and delirium tremens, a life-threatening complication. Additionally, medications like acamprosate (666 mg three times daily) and disulfiram (250 mg daily) are used post-detoxification to reduce cravings and discourage drinking. Therapies such as motivational interviewing and 12-step programs provide psychological support, helping individuals build coping strategies and maintain sobriety.
A key difference in treatment lies in the timing and duration of medication use. Heroin withdrawal medications are often prescribed long-term, sometimes for years, to support recovery. Alcohol withdrawal medications, however, are typically short-term, focusing on acute symptom management. This distinction underscores the chronic nature of opioid dependence versus the episodic nature of alcohol withdrawal.
Practical tips for both treatments include consistent monitoring and individualized care. For heroin withdrawal, patients should be educated on the risks of overdose if they relapse while on maintenance therapy. For alcohol withdrawal, hydration and nutritional support are critical, as chronic alcohol use often leads to deficiencies. Both conditions benefit from a multidisciplinary approach, involving physicians, therapists, and support groups to address the physical, psychological, and social aspects of addiction.
In summary, while heroin and alcohol withdrawal treatments share the goal of stabilizing the patient and preventing relapse, their methodologies diverge based on the unique challenges each substance presents. Medications and therapies must be carefully selected and tailored to ensure effective and safe recovery.
Alcohol and Viruses: Separating Fact from Fiction in Health Claims
You may want to see also
Explore related products






![]()
Relapse Factors: Common triggers for relapse in heroin and alcohol withdrawal
Heroin and alcohol withdrawal share striking similarities in their relapse triggers, often rooted in the physiological and psychological grip these substances exert on the brain. Both substances hijack the brain’s reward system, creating intense cravings and a heightened sensitivity to stress. For instance, a study published in *Addiction* found that individuals undergoing withdrawal from either heroin or alcohol exhibited similar levels of cortisol, the stress hormone, which is a known predictor of relapse. This biological overlap underscores why certain triggers—stress, environmental cues, and emotional distress—are universal relapse risks for both substances.
Consider the role of environmental cues, a potent trigger for relapse in both heroin and alcohol withdrawal. For someone with a history of heroin use, seeing a needle or visiting a neighborhood where they previously purchased drugs can reignite cravings. Similarly, for someone in alcohol recovery, the sight of a bar, the smell of beer, or even a social gathering where alcohol is present can trigger an overwhelming urge to drink. These cues activate the brain’s conditioned response, making relapse feel almost involuntary. Practical advice? Avoid high-risk environments during early recovery and develop a plan to manage unavoidable exposure, such as attending social events with a sober companion.
Emotional distress is another shared relapse factor, though it manifests differently for heroin and alcohol users. Heroin withdrawal often amplifies feelings of anxiety and depression, while alcohol withdrawal can lead to irritability and mood swings. Both states create a vulnerability to relapse as individuals seek to self-medicate their emotional pain. For example, a 30-year-old heroin user in recovery might relapse after a breakup, while a 45-year-old alcohol-dependent individual might turn to drinking after losing a job. To mitigate this, incorporating therapy, mindfulness practices, or support groups like NA or AA can provide healthier coping mechanisms for emotional turmoil.
Stress, particularly chronic stress, is a universal relapse trigger that demands proactive management. Research in *Psychopharmacology* highlights that stress increases dopamine release in the brain’s reward pathways, mimicking the effects of heroin or alcohol and intensifying cravings. For instance, a heroin user under financial strain or an alcoholic facing family conflict may find themselves at heightened risk. Practical strategies include stress-reduction techniques like exercise, meditation, or even structured routines to minimize unpredictability. Additionally, medications such as naltrexone (for alcohol) or buprenorphine (for heroin) can reduce cravings and provide a buffer against stress-induced relapse.
Finally, social isolation is a less obvious but equally dangerous relapse factor for both heroin and alcohol withdrawal. Recovery often requires distancing oneself from old social circles, but this can lead to loneliness, a known risk factor for relapse. A 25-year-old heroin user or a 50-year-old alcoholic, both isolated from friends and family, may return to substance use to fill the void. Building a new support network—whether through recovery groups, hobbies, or community activities—is essential. For example, joining a local sports team or volunteering can provide structure and social connection without the risk of exposure to triggers.
In addressing relapse factors, the key is specificity and action. Understanding the shared triggers of heroin and alcohol withdrawal allows for targeted interventions, from avoiding environmental cues to managing stress and fostering social connections. Recovery is a process, not a destination, and recognizing these common pitfalls can empower individuals to navigate it more successfully.
Discover Your Next Drink: What's in My Fridge Alcohol App
You may want to see also
Frequently asked questions
Yes, both heroin and alcohol withdrawal share some common symptoms, including anxiety, insomnia, nausea, sweating, and muscle aches. However, the severity and specific symptoms can vary depending on the substance and the individual's level of dependence.
Yes, both withdrawals can be dangerous and potentially life-threatening. Alcohol withdrawal can lead to seizures, delirium tremens (DTs), and cardiovascular complications, while heroin withdrawal, though less likely to be fatal, can cause severe dehydration and complications from pre-existing health conditions.
Yes, medical supervision is highly recommended for both withdrawals. Alcohol withdrawal, in particular, often requires medical intervention due to the risk of severe complications. Heroin withdrawal, while typically not as medically urgent, benefits from professional support to manage symptoms and prevent relapse.
The timelines differ. Alcohol withdrawal symptoms typically begin within 6-24 hours after the last drink and peak within 24-72 hours. Heroin withdrawal symptoms usually start within 6-12 hours after the last dose, peak within 24-48 hours, and can last 5-7 days, though some symptoms may persist longer.
Treatment approaches overlap but are tailored to the substance. Both may include medications (e.g., methadone or buprenorphine for heroin, benzodiazepines for alcohol), hydration, and counseling. However, alcohol withdrawal often requires specific medications to prevent seizures and DTs, while heroin treatment focuses on opioid replacement therapy and managing cravings.