The question of whether heavy drinkers are automatically classified as alcoholics is a nuanced and complex issue. While heavy drinking, defined as consuming large amounts of alcohol regularly, is a significant risk factor for developing alcohol use disorder (AUD), not all heavy drinkers meet the clinical criteria for alcoholism. Alcoholism, or AUD, is a chronic condition characterized by an inability to control or stop drinking despite adverse consequences, and it involves physical dependence, withdrawal symptoms, and a negative impact on personal and professional life. Heavy drinkers may exhibit some risky behaviors, but they might still maintain control over their consumption and avoid the severe consequences associated with AUD. Therefore, it is essential to differentiate between heavy drinking and alcoholism, as the latter requires professional diagnosis and treatment, whereas the former may be addressed through lifestyle changes or moderation strategies.
| Characteristics | Values |
|---|---|
| Definition of Heavy Drinking | For men: 15+ drinks/week; For women: 8+ drinks/week (NIAAA guidelines) |
| Alcoholism (AUD) Definition | A chronic relapsing disorder characterized by impaired control over alcohol use, compulsive drinking, and negative emotional state when not drinking (DSM-5). |
| Overlap Between Heavy Drinking and AUD | Heavy drinking is a risk factor for AUD but not all heavy drinkers are alcoholics. |
| Prevalence of AUD Among Heavy Drinkers | ~10-15% of heavy drinkers meet criteria for AUD (based on studies). |
| Key Differences | Heavy drinkers may not experience withdrawal, cravings, or negative life consequences, unlike those with AUD. |
| Physical Health Risks | Both groups face risks like liver disease, cardiovascular issues, and cancer. |
| Psychological Factors | AUD involves dependence, tolerance, and inability to quit despite harm; heavy drinkers may not exhibit these traits. |
| Social and Behavioral Impact | AUD often leads to relationship issues, job loss, and legal problems; heavy drinkers may not experience these. |
| Treatment Needs | AUD requires structured treatment (therapy, medication); heavy drinkers may benefit from moderation strategies. |
| Screening Tools | AUDIT (Alcohol Use Disorders Identification Test) helps differentiate between heavy drinking and AUD. |
| Latest Research (2023) | Studies emphasize that heavy drinking is a spectrum, with AUD being the severe end. |
Explore related products






What You'll Learn
- Defining Heavy Drinking: What constitutes heavy drinking according to health guidelines and medical standards
- Heavy Drinking vs. Alcoholism: Key differences between habitual heavy drinking and clinical alcoholism
- Risk Factors: Factors that may push heavy drinkers into alcoholism, such as genetics or stress
- Physical Health Impact: How heavy drinking affects the body, even without meeting alcoholism criteria
- Behavioral Indicators: Signs that a heavy drinker may be transitioning into alcoholism
![]()
Defining Heavy Drinking: What constitutes heavy drinking according to health guidelines and medical standards
Heavy drinking is not a casual term thrown around in health discussions; it’s a precise definition rooted in medical and scientific standards. According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA), heavy drinking for men is defined as consuming 15 drinks or more per week, while for women, it’s 8 drinks or more per week. These thresholds are not arbitrary—they are based on extensive research linking these quantities to increased health risks, including liver disease, cardiovascular problems, and mental health disorders. Understanding these numbers is the first step in distinguishing between social drinking and patterns that may signal deeper issues.
To put these guidelines into perspective, consider what constitutes a "standard drink." In the U.S., one standard drink is equivalent to 14 grams of pure alcohol, found in 12 ounces of regular beer (5% ABV), 5 ounces of wine (12% ABV), or 1.5 ounces of distilled spirits (40% ABV). For instance, a man who consumes two beers (24 ounces) and a shot of whiskey (1.5 ounces) in a day has already exceeded the daily recommended limit for moderate drinking. Tracking intake in these units can help individuals assess whether their habits align with heavy drinking criteria.
Age and health status further complicate the definition of heavy drinking. For individuals over 65, the NIAAA recommends lower limits due to age-related changes in metabolism and increased sensitivity to alcohol. Older adults should limit themselves to 7 drinks per week, regardless of gender. Similarly, individuals with pre-existing health conditions, such as liver disease or diabetes, may need to abstain entirely or adhere to stricter limits. These adjustments highlight the importance of personalized guidelines rather than a one-size-fits-all approach.
While heavy drinking does not automatically equate to alcoholism, it is a significant risk factor. The line between heavy drinking and alcohol use disorder (AUD) is often blurred, but key distinctions exist. Heavy drinkers may consume large quantities without experiencing dependence, whereas individuals with AUD struggle with cravings, withdrawal symptoms, and an inability to control their drinking. Recognizing the difference is crucial for seeking appropriate intervention—whether it’s moderating intake or pursuing treatment for addiction.
Practical steps can help individuals evaluate and modify their drinking habits. Keeping a drinking diary, setting specific limits, and incorporating alcohol-free days are effective strategies. For those concerned about their consumption, consulting a healthcare provider can provide clarity and tailored advice. Ultimately, understanding what constitutes heavy drinking is not about judgment but about informed decision-making to safeguard long-term health.
Does Alcohol Have Fuzz? Unraveling the Myth Behind the Texture
You may want to see also
Explore related products






![]()
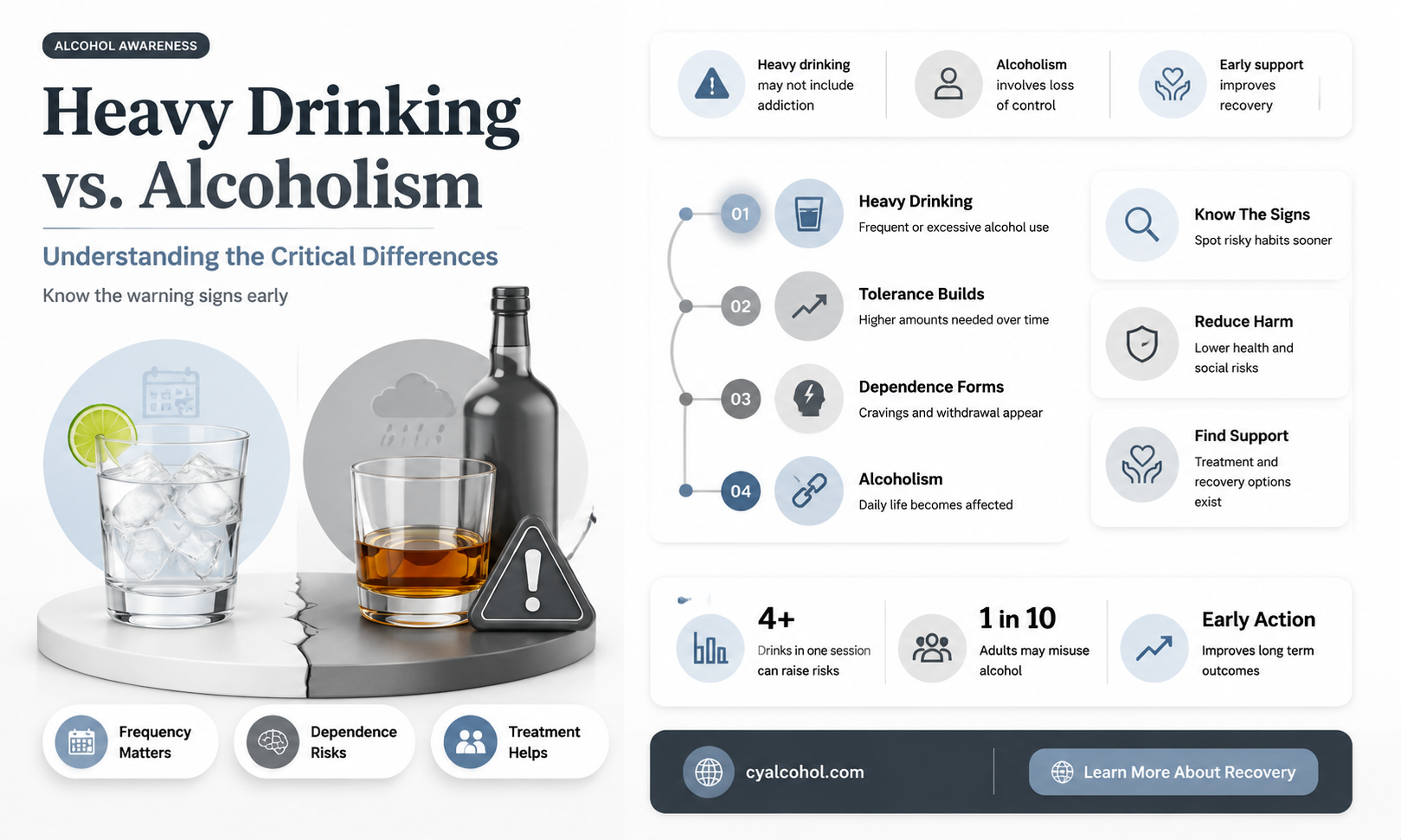
Heavy Drinking vs. Alcoholism: Key differences between habitual heavy drinking and clinical alcoholism
Heavy drinking and alcoholism are often conflated, but they are distinct phenomena with critical differences. According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA), heavy drinking is defined as consuming 15 drinks or more per week for men and 8 drinks or more per week for women. In contrast, alcoholism, or alcohol use disorder (AUD), is a chronic medical condition characterized by an inability to control or stop drinking despite adverse consequences. Understanding these definitions is the first step in distinguishing between a habit and a disorder.
Consider the case of a 35-year-old professional who regularly consumes 12 drinks per week, primarily during social events. This individual meets the criteria for heavy drinking but does not exhibit signs of AUD, such as withdrawal symptoms, tolerance, or failed attempts to cut down. Here, the key difference lies in control. Heavy drinkers may consume large quantities but can often set limits, whereas individuals with AUD struggle with compulsive use, even when it harms their health, relationships, or career. For instance, a heavy drinker might skip alcohol during a busy workweek, while someone with AUD would find this nearly impossible without experiencing cravings or physical symptoms.
From a clinical perspective, diagnosing AUD involves assessing 11 criteria outlined in the DSM-5, including drinking more than intended, unsuccessful efforts to quit, and continued use despite social or interpersonal problems. Heavy drinking, however, is a behavioral pattern that does not necessarily involve these markers. For example, a college student binge drinking on weekends (5+ drinks in 2 hours for men, 4+ for women) may be a heavy drinker but not an alcoholic if they lack dependence or negative life impacts. Practical tips for self-assessment include tracking drinking patterns, noting cravings, and evaluating whether alcohol interferes with daily responsibilities.
Age and context also play a role. Young adults may engage in heavy drinking due to social norms but outgrow the behavior, while older individuals might develop AUD after years of gradual escalation. For those concerned about their drinking, the NIAAA recommends limiting intake to 4 drinks per day for men and 3 for women on any single day. If cutting back feels impossible, it may signal AUD, warranting professional intervention. Ultimately, while heavy drinking is a risk factor for alcoholism, not all heavy drinkers are alcoholics—the distinction hinges on control, consequences, and clinical criteria.
Alcohol Newspaper Nail Art: A Simple Guide
You may want to see also
Explore related products






![]()
Risk Factors: Factors that may push heavy drinkers into alcoholism, such as genetics or stress
Heavy drinking doesn’t automatically equate to alcoholism, but certain risk factors can tip the scale. Genetics play a significant role; individuals with a family history of alcohol use disorder (AUD) are four times more likely to develop it themselves. This isn’t about destiny—it’s about predisposition. Specific genes, like those affecting dopamine receptors or alcohol metabolism, can heighten sensitivity to alcohol’s effects or reduce its aversive qualities, making moderation harder. If your family tree includes AUD, consider this a red flag, not a sentence, and monitor your drinking habits closely.
Stress acts as a silent accelerant, pushing heavy drinkers closer to alcoholism. Chronic stress triggers the brain’s reward system, making alcohol a quick escape from anxiety or overwhelm. Studies show that individuals under prolonged stress are twice as likely to escalate from heavy drinking to dependence. For example, a 40-hour workweek coupled with caregiving responsibilities can create a perfect storm for nightly drinking to "unwind." To break this cycle, replace alcohol with stress-reducing alternatives like mindfulness, exercise, or therapy. Even 10 minutes of deep breathing daily can rewire the brain’s response to stress.
Environmental factors, like social circles or accessibility, often fly under the radar but are equally potent. Heavy drinkers in environments where alcohol is normalized—think corporate cultures with frequent happy hours or peer groups centered around drinking—face constant pressure to consume. Proximity matters too; living within a mile of multiple liquor stores increases drinking frequency by 20%. To mitigate this, consciously curate your surroundings. Join non-drinking social groups, stock your fridge with non-alcoholic alternatives, and set clear boundaries with peers who encourage excessive consumption.
Age and developmental stages introduce unique vulnerabilities. Young adults aged 18–25, whose brains are still developing, are more susceptible to alcohol’s neurotoxic effects, increasing the risk of dependence. Conversely, older adults may turn to alcohol to cope with isolation or health issues, with 1 in 5 seniors binge drinking at least once a month. Tailored interventions are key: college students benefit from campus programs promoting healthy habits, while seniors may need support addressing underlying loneliness or pain. Regardless of age, early intervention—like tracking drinks via apps or setting drink limits—can prevent progression to AUD.
Finally, co-occurring mental health disorders act as a double-edged sword. Conditions like depression, anxiety, or PTSD often coexist with heavy drinking, as alcohol temporarily alleviates symptoms. However, this self-medication worsens the underlying disorder over time, creating a vicious cycle. For instance, someone with untreated anxiety might drink to calm nerves but experience heightened anxiety the next day, fueling further drinking. Integrated treatment—addressing both mental health and alcohol use simultaneously—is critical. Cognitive-behavioral therapy (CBT) paired with medication management has shown a 60% success rate in reducing alcohol dependence in dual-diagnosis cases. Recognize the interplay and seek holistic care to disrupt the cycle.
Alcohol and Cialis: Understanding the Risks and Interactions
You may want to see also
Explore related products






![]()
Physical Health Impact: How heavy drinking affects the body, even without meeting alcoholism criteria
Heavy drinking, even if it doesn’t meet the clinical criteria for alcoholism, takes a relentless toll on the body. The liver, often the first casualty, struggles to metabolize excessive alcohol, leading to fatty liver disease, inflammation, and eventually cirrhosis. For context, consuming more than 30 grams of alcohol (roughly 2 standard drinks) daily for men, or 20 grams for women, significantly elevates this risk over time. Unlike alcoholism, which involves dependency and loss of control, heavy drinking is defined by quantity and frequency—yet the physical consequences overlap dangerously.
Consider the cardiovascular system, which suffers silently under the weight of consistent alcohol intake. Blood pressure rises, heart muscles weaken, and the risk of stroke or irregular heartbeat (atrial fibrillation) climbs. A 2020 study in *The Lancet* found that even moderate drinkers (14–21 drinks weekly) had a 1.3 times higher risk of hypertension compared to non-drinkers. Heavy drinkers, often consuming 4–5 times this amount, face exponentially greater dangers. The irony? Many heavy drinkers don’t recognize these risks because they lack the behavioral markers of alcoholism, such as withdrawal symptoms or failed attempts to quit.
The digestive system also pays a steep price. Chronic heavy drinking irritates the stomach lining, causing gastritis, ulcers, and malnutrition as alcohol interferes with nutrient absorption. For instance, thiamine deficiency, common in heavy drinkers, can lead to Wernicke-Korsakoff syndrome, a debilitating neurological disorder. Meanwhile, the pancreas, overwhelmed by toxins, may develop pancreatitis—a painful, life-threatening condition. These issues often emerge long before psychological dependence sets in, highlighting the body’s vulnerability to sheer volume over time.
Even the immune system falters under heavy drinking’s assault. Regularly exceeding recommended limits (up to 1 drink/day for women, 2 for men) weakens the body’s ability to fight infections, from common colds to pneumonia. A 2015 study in *Alcohol Research* showed that heavy drinkers are more susceptible to tuberculosis and respiratory infections due to impaired immune responses. This physical deterioration occurs regardless of whether the drinker exhibits the psychological or social hallmarks of alcoholism, underscoring the misconception that harm requires addiction.
Practical steps can mitigate these risks, even for those not ready to quit entirely. Limiting intake to below recommended thresholds, incorporating alcohol-free days, and pairing drinks with food to slow absorption are simple yet effective strategies. Regular health screenings, particularly liver function tests and blood pressure checks, can catch early signs of damage. The takeaway? Heavy drinking’s physical toll is undeniable and often irreversible—a stark reminder that the body counts every drink, whether addiction is present or not.
Alcohol's Impact: Does Drinking Raise Your Lipid Levels?
You may want to see also
Explore related products






![]()
Behavioral Indicators: Signs that a heavy drinker may be transitioning into alcoholism
Heavy drinking, often defined as consuming 8 or more drinks per week for women and 15 or more for men, doesn’t automatically equate to alcoholism. However, the line between the two can blur when behavioral changes signal a shift from habit to dependency. One of the earliest indicators is increased tolerance, where the individual requires larger amounts of alcohol to achieve the same effect. For instance, someone who once felt intoxicated after 2 drinks now needs 4 or 5. This isn’t merely a sign of a "strong stomach" but a physiological adaptation that often precedes addiction.
Another critical behavioral red flag is withdrawal from social or professional obligations. Heavy drinkers transitioning into alcoholism may start skipping work, ignoring family commitments, or abandoning hobbies they once enjoyed. This withdrawal is often accompanied by irritability or restlessness when alcohol is unavailable. For example, a person who cancels plans with friends repeatedly because they’re "too tired" might actually be prioritizing drinking over social interaction. Observing these patterns requires attention to consistency—occasional cancellations are normal, but frequent, alcohol-related excuses are not.
Secretive drinking is a third indicator that often emerges as heavy drinking evolves into alcoholism. Individuals may hide bottles, lie about consumption, or drink alone to avoid judgment. This behavior reflects a growing awareness of their problematic relationship with alcohol, even if they deny it verbally. For instance, someone might claim they only had "a couple of beers" while disposing of multiple empty cans discreetly. Such actions suggest a loss of control, a hallmark of addiction.
Finally, failed attempts to cut back are a definitive sign of progression from heavy drinking to alcoholism. If a person repeatedly tries to reduce their intake but finds themselves unable to do so, it indicates a psychological or physical dependency. Practical steps to identify this include setting clear limits (e.g., "I’ll only drink on weekends") and monitoring adherence. Persistent failure despite genuine effort warrants professional intervention, as it highlights the inability to self-regulate alcohol consumption.
In summary, behavioral indicators like increased tolerance, social withdrawal, secretive drinking, and failed attempts to cut back serve as warning signs that heavy drinking may be transitioning into alcoholism. Recognizing these patterns early allows for timely intervention, whether through self-reflection, support systems, or professional help. The key is to act before the line between habit and addiction becomes irreversible.
Jello Shots: Balancing Sweetness and Alcohol Flavor - What to Expect
You may want to see also
Frequently asked questions
No, not all heavy drinkers are alcoholics. Heavy drinking refers to consuming large amounts of alcohol, but alcoholism (or alcohol use disorder) involves a physical and psychological dependence on alcohol, along with a loss of control over drinking.
Look for signs such as inability to stop drinking once started, withdrawal symptoms when not drinking, neglecting responsibilities, and continued drinking despite negative consequences. These indicate alcoholism rather than just heavy drinking.
Yes, some heavy drinkers can consume large amounts without developing a physical or psychological dependence. However, the risk of developing alcoholism increases with heavy and frequent drinking.
Not always, but heavy drinking significantly raises the risk of developing alcoholism. Factors like genetics, environment, and mental health also play a role in whether someone progresses to alcohol dependence.
Some heavy drinkers can reduce or quit drinking on their own, but those with alcoholism often need professional help due to the physical and psychological challenges of withdrawal and recovery.