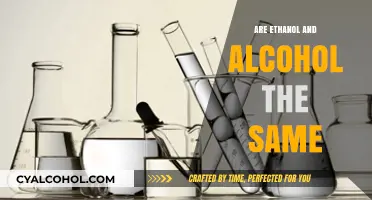
Alcohol withdrawal is a complex and potentially severe condition that occurs when individuals abruptly reduce or cease heavy and prolonged alcohol consumption. One of the lesser-known but significant symptoms of this process is the occurrence of hallucinations, which can manifest as visual, auditory, or tactile experiences that are not based in reality. These hallucinations are often distressing and can significantly impact an individual's mental state, raising questions about their prevalence and underlying causes. Understanding whether hallucinations are a common symptom of alcohol withdrawal is crucial for healthcare professionals and those affected, as it highlights the need for proper medical supervision and support during detoxification to ensure safety and effective management of withdrawal symptoms.
| Characteristics | Values |
|---|---|
| Prevalence | Hallucinations occur in approximately 10-20% of individuals with alcohol withdrawal syndrome. |
| Type of Hallucinations | Typically auditory (hearing voices or sounds), but can also be visual or tactile. |
| Onset Time | Usually begin 12-24 hours after the last drink, peaking at 24-48 hours. |
| Duration | Last 1-3 days, but can persist longer in severe cases. |
| Associated Condition | Often linked to delirium tremens (DTs), a severe form of alcohol withdrawal. |
| Risk Factors | Heavy, prolonged alcohol use; prior withdrawal episodes; co-occurring medical or psychiatric conditions. |
| Differential Diagnosis | Must be distinguished from other causes of hallucinations (e.g., schizophrenia, drug use, or medical conditions). |
| Treatment | Benzodiazepines (e.g., diazepam, lorazepam) are the first-line treatment to manage symptoms and prevent progression to DTs. |
| Prognosis | Generally resolves with appropriate treatment, but untreated cases can lead to complications or death. |
| Prevention | Gradual reduction of alcohol intake under medical supervision can reduce the risk of severe withdrawal symptoms. |
Explore related products






What You'll Learn
![]()
Prevalence of Hallucinations in Alcohol Withdrawal
Alcohol withdrawal hallucinations typically occur within 12 to 24 hours after the last drink, affecting approximately 20% of individuals undergoing severe withdrawal. These visual, auditory, or tactile hallucinations are a hallmark of alcohol withdrawal syndrome (AWS) and often signify progression to a more dangerous phase. Unlike the hallucinations associated with conditions like schizophrenia, which are persistent and complex, AWS-related hallucinations are usually transient and simple—such as seeing insects crawling on walls or hearing indistinct voices. This distinction is critical for clinicians to accurately diagnose and manage symptoms before they escalate to life-threatening complications like seizures or delirium tremens.
The prevalence of these hallucinations is closely tied to the duration and intensity of alcohol consumption. Chronic heavy drinkers—defined as consuming more than 15 drinks per week for men or 8 for women—are at highest risk. For context, a "drink" is standardized as 14 grams of pure alcohol (e.g., 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of distilled spirits). Individuals with a history of multiple withdrawal episodes face compounded risk due to kindling, a phenomenon where the brain becomes increasingly sensitive to withdrawal triggers, lowering the threshold for hallucinations and other severe symptoms.
From a clinical perspective, managing these hallucinations requires a dual approach: pharmacological intervention and environmental control. Benzodiazepines, such as diazepam or lorazepam, are first-line treatments to stabilize GABA receptors disrupted by chronic alcohol use. Dosing is tailored to symptom severity, often starting with 10–20 mg of diazepam every 1–2 hours until symptoms subside. Concurrently, patients should be placed in a calm, well-lit environment with minimal sensory stimuli to reduce the likelihood of hallucination triggers. Family members or caregivers must be instructed to avoid confrontation and instead provide gentle reassurance during episodes.
A comparative analysis of AWS hallucinations with those from other substances, like cocaine or opioids, reveals key differences. While stimulant-induced hallucinations often involve paranoia or persecutory themes, alcohol withdrawal hallucinations tend to be neutral or mildly distressing. This distinction influences treatment strategies; for instance, antipsychotics are rarely needed for AWS unless agitation co-occurs. However, the transient nature of these hallucinations does not diminish their clinical significance—they serve as a red flag for potential progression to delirium tremens, which carries a 5–15% mortality rate if untreated.
In practical terms, individuals at risk should monitor withdrawal symptoms closely and seek medical attention if hallucinations occur. Over-the-counter sleep aids or herbal remedies are ineffective and potentially dangerous in this context. Instead, a tapering schedule under medical supervision, combined with hydration and electrolyte balance, can mitigate risks. For those in recovery, understanding the prevalence and triggers of these hallucinations empowers proactive management, reducing the likelihood of relapse during the vulnerable withdrawal phase.
Does Alcohol Break Keto? A Guide to Drinking on Ketosis
You may want to see also
Explore related products





![]()
Types of Hallucinations Experienced During Withdrawal
Alcohol withdrawal hallucinations typically manifest within 12 to 24 hours after the last drink, peaking in intensity between 24 and 48 hours. These are not the same as the more severe delirium tremens (DTs), which involve confusion and fever. Instead, they are distinct perceptual disturbances that can be categorized into several types, each with its own characteristics and implications for management.
Visual Hallucinations are among the most common during alcohol withdrawal. Individuals may see objects, people, or patterns that are not present. These hallucinations often involve simple shapes or moving dots but can escalate to more complex scenes. For instance, a person might perceive insects crawling on the walls or shadows moving independently. Unlike the hallucinations associated with schizophrenia, these are typically recognized as unreal by the individual, though they can still cause significant distress. Management often involves a quiet, dimly lit environment to reduce sensory overload, along with medications like benzodiazepines to stabilize the nervous system.
Auditory Hallucinations, though less frequent, can also occur. These involve hearing sounds or voices that do not exist. Unlike visual hallucinations, auditory ones may be more disturbing because they can mimic real conversations or commands. For example, a person might hear whispers or a voice urging them to take action. These hallucinations require careful monitoring, as they can lead to unsafe behaviors. Cognitive-behavioral techniques, such as grounding exercises, can help individuals differentiate between real and imagined sounds.
Tactile Hallucinations involve the sensation of touch without a physical stimulus. Individuals might feel as though insects are crawling on their skin or experience burning or itching sensations. These hallucinations can be particularly distressing and may lead to self-injury, such as scratching or picking at the skin. Antihistamines or topical treatments can provide temporary relief, but the primary focus should be on addressing the underlying withdrawal symptoms through medical intervention.
Olfactory and Gustatory Hallucinations, while rare, involve smelling or tasting things that are not present. For example, a person might perceive a foul odor or a metallic taste in their mouth. These hallucinations are often fleeting but can contribute to nausea or aversion to food and drink, complicating hydration and nutrition during withdrawal. Encouraging small, frequent sips of water and bland, easily digestible foods can help mitigate these effects.
Understanding the types of hallucinations experienced during alcohol withdrawal is crucial for both individuals and caregivers. Early recognition allows for prompt intervention, reducing the risk of complications. While these hallucinations are typically short-lived, lasting from a few hours to a few days, they signal a critical phase of withdrawal that requires medical supervision. Combining pharmacological treatments with environmental modifications and psychological support can significantly improve outcomes, ensuring a safer and more comfortable detoxification process.
Alcoholics in the US: Who Are They?
You may want to see also
Explore related products





![]()
Risk Factors for Hallucinations in Withdrawal
Alcohol withdrawal hallucinations are not a universal experience, but certain individuals face a heightened risk. Understanding these risk factors is crucial for early intervention and prevention. One of the most significant predictors is the severity and duration of alcohol dependence. Chronic heavy drinkers, defined as consuming more than 15 drinks per week for men or 8 drinks per week for women, are particularly vulnerable. The body’s neurochemical balance becomes disrupted over time, leading to a higher likelihood of hallucinations during withdrawal. For instance, individuals with a history of consuming 4-5 standard drinks daily for several years may experience more intense withdrawal symptoms, including visual or auditory hallucinations, compared to moderate drinkers.
Another critical risk factor is the abrupt cessation of alcohol intake. Tapering off alcohol consumption gradually, rather than quitting cold turkey, can significantly reduce the risk of hallucinations. Medical professionals often recommend a structured tapering plan, reducing daily intake by 10-20% every few days, under supervision. This approach allows the brain to adjust slowly, minimizing the shock to the central nervous system. Ignoring this advice and abruptly stopping after prolonged heavy use can trigger severe withdrawal symptoms, including hallucinations, within 12-48 hours of the last drink.
Age and overall health also play a role in the likelihood of experiencing hallucinations during withdrawal. Older adults, particularly those over 60, are at increased risk due to age-related changes in metabolism and brain function. Additionally, individuals with pre-existing mental health conditions, such as schizophrenia or bipolar disorder, are more susceptible. For example, a 65-year-old with a 20-year history of heavy drinking and a diagnosis of depression is far more likely to experience hallucinations during withdrawal than a younger, otherwise healthy individual with a shorter history of alcohol use.
Environmental and genetic factors further contribute to the risk profile. A family history of alcoholism or substance abuse disorders increases susceptibility, as does exposure to high-stress environments. Stress exacerbates withdrawal symptoms, making hallucinations more probable. Practical steps to mitigate this include creating a calm, supportive environment during detoxification and incorporating stress-reduction techniques like mindfulness or meditation. For those with a genetic predisposition, early intervention and monitoring are essential, as the risk of severe withdrawal symptoms, including hallucinations, is significantly elevated.
Finally, the presence of co-occurring substance use disorders amplifies the risk. Individuals who use alcohol alongside other depressants, such as benzodiazepines, or stimulants, like cocaine, face a compounded risk of severe withdrawal symptoms. Polydrug use complicates the detoxification process, often leading to more unpredictable and intense symptoms, including hallucinations. A comprehensive assessment of all substances used is critical for accurate risk evaluation and tailored treatment planning. Addressing these risk factors proactively can significantly reduce the likelihood of hallucinations during alcohol withdrawal, improving safety and outcomes.
Alcohol and Metabolism: Does Drinking Boost or Slow Your Burn?
You may want to see also
Explore related products






![]()
Duration and Severity of Withdrawal Hallucinations
Alcohol withdrawal hallucinations typically emerge within 12 to 24 hours after the last drink, marking a critical phase in the withdrawal timeline. These hallucinations, often visual or auditory, can persist for up to 48 hours, though individual experiences vary based on factors like the duration and intensity of alcohol use. For heavy drinkers, defined as consuming more than 15 drinks per week for men or 8 for women, the onset may be quicker and the duration longer. Understanding this window is crucial for caregivers and individuals undergoing withdrawal, as it helps in anticipating and managing symptoms effectively.
The severity of withdrawal hallucinations is closely tied to the body’s dependence on alcohol and the abruptness of cessation. Mild hallucinations, such as fleeting shadows or indistinct sounds, are more common in moderate cases. Severe hallucinations, however, can involve vivid, distressing visions or conversations with imaginary entities, often accompanied by confusion and agitation. These severe episodes are more likely in individuals with a history of prolonged, heavy drinking or those with co-occurring mental health disorders. Monitoring for signs of progression to delirium tremens (DTs), a life-threatening condition, is essential during this period.
Managing the duration and severity of withdrawal hallucinations requires a multi-faceted approach. Medications like benzodiazepines can alleviate symptoms by stabilizing brain chemistry, but they must be administered under medical supervision to avoid dependency. Hydration and nutritional support, particularly replenishing electrolytes and vitamins like thiamine, can aid recovery. For those at high risk, inpatient treatment is recommended, as it provides continuous monitoring and access to emergency interventions if hallucinations escalate.
Practical tips for individuals experiencing withdrawal include maintaining a calm environment to minimize sensory overload, avoiding caffeine and other stimulants, and establishing a routine to reduce anxiety. Family members or caregivers should remain vigilant for signs of worsening symptoms, such as increased heart rate, fever, or unresponsiveness, which may indicate the need for immediate medical attention. Early intervention not only shortens the duration of hallucinations but also reduces the risk of complications.
In summary, withdrawal hallucinations are a time-sensitive and variable aspect of alcohol cessation, influenced by factors like consumption patterns and overall health. Recognizing their typical duration and potential severity allows for proactive management, ensuring safer and more effective recovery. Whether through medical intervention, environmental adjustments, or supportive care, addressing these symptoms promptly can significantly improve outcomes for those navigating alcohol withdrawal.
Addressing Alcohol Abuse in Northern Ireland: Strategies and Challenges
You may want to see also
Explore related products



![Delirium: Photo of Gioia [4K Ultra HD + Blu-ray Set]](https://m.media-amazon.com/images/I/712-8+HrBCL._AC_UL320_.jpg)


![]()
Treatment Options for Hallucinations in Alcohol Withdrawal
Hallucinations during alcohol withdrawal are a severe symptom of delirium tremens (DTs), occurring in approximately 5% of cases. These visual, auditory, or tactile distortions demand immediate medical intervention to prevent complications like seizures or cardiovascular collapse. Treatment protocols prioritize stabilization, symptom management, and long-term recovery strategies.
Pharmacological Interventions: The First Line of Defense
Benzodiazepines remain the cornerstone of treatment, with dosing tailored to symptom severity. For mild-to-moderate agitation, oral diazepam (10–20 mg every 1–2 hours) or lorazepam (2–4 mg every 1–2 hours) is initiated, titrated until symptoms subside. In severe cases or when oral administration is impossible, intravenous lorazepam (1–2 mg repeated every 10–15 minutes) or diazepam (5–10 mg repeated every 5–10 minutes) is used. Antipsychotics like haloperidol (5–10 mg IM/IV) may be added for refractory hallucinations, but only under close monitoring due to risks of lowering seizure thresholds.
Supportive Care: Stabilizing the Body’s Systems
Concurrently, electrolyte imbalances (e.g., hypomagnesemia, hypokalemia) and dehydration are corrected via intravenous fluids and electrolyte replacement. Thiamine (100 mg IV/IM daily) is administered to prevent Wernicke’s encephalopathy, a life-threatening complication. Vital signs are continuously monitored, with ICU admission reserved for patients with tachycardia (>120 bpm), hypertension (systolic >180 mmHg), or hyperthermia (>38°C).
Psychosocial and Behavioral Strategies: Beyond Medication
Once acute symptoms stabilize, cognitive-behavioral therapy (CBT) and motivational interviewing address underlying triggers for alcohol use. Inpatient rehab programs offer structured environments, while peer support groups (e.g., Alcoholics Anonymous) provide ongoing accountability. For patients with co-occurring mental health disorders, integrated treatment plans combining medication (e.g., naltrexone 50 mg daily) and psychotherapy improve long-term outcomes.
Preventive Measures: Reducing Future Risks
Outpatient management focuses on relapse prevention. Disulfiram (250 mg daily) deters drinking by inducing aversive reactions, while acamprosate (666 mg TID) reduces cravings. Lifestyle modifications—such as limiting caffeine, establishing sleep hygiene, and avoiding triggers—complement pharmacotherapy. Regular follow-ups with addiction specialists ensure adherence and early intervention for emerging symptoms.
Cautions and Considerations: Balancing Risks and Benefits
Benzodiazepine use requires caution in elderly patients (>65 years) due to increased fall risks and cognitive impairment. Pregnant individuals should avoid disulfiram, opting instead for behavioral interventions. All patients must be educated on the dangers of abrupt alcohol cessation without medical supervision, as self-managed withdrawal increases the risk of DTs by 30–40%.
This multi-faceted approach—combining pharmacology, supportive care, and psychosocial strategies—maximizes recovery while minimizing complications from alcohol withdrawal hallucinations.
Exploring Fort Worth Zoo: Alcohol Availability and Family-Friendly Fun
You may want to see also
Frequently asked questions
Yes, hallucinations can occur during alcohol withdrawal, particularly in severe cases. They are most commonly associated with a condition called delirium tremens (DTs), which affects about 5% of individuals withdrawing from alcohol.
The most common type of hallucinations during alcohol withdrawal are visual hallucinations, where individuals see things that are not there. These hallucinations are often vivid and can be distressing, though auditory or tactile hallucinations may also occur.
Hallucinations typically appear within 12 to 48 hours after the last drink and can last for 1 to 3 days. They are a sign of severe withdrawal and require immediate medical attention to prevent complications like delirium tremens.













![Delirium [Region Free]](https://m.media-amazon.com/images/I/71VlmmK79HL._AC_UL320_.jpg)