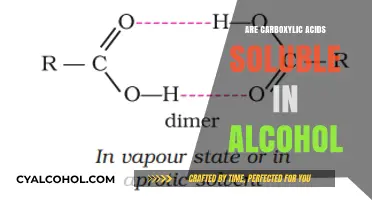
Benzodiazepines (benzos) and alcohol are both central nervous system depressants that can produce similar effects, such as relaxation, sedation, and reduced anxiety, but they are not the same. While alcohol is a legal and widely consumed substance, benzos are prescription medications primarily used to treat anxiety, insomnia, and seizures. Despite their differences, both substances can lead to dependence, tolerance, and dangerous interactions when combined, as they enhance each other's sedative effects, increasing the risk of respiratory depression, overdose, and other serious health complications. Understanding their distinct mechanisms, risks, and potential for harm is crucial for safe use and informed decision-making.
| Characteristics | Values |
|---|---|
| Chemical Class | Benzos: Benzodiazepines (prescription drugs); Alcohol: Ethanol (depressant) |
| Mechanism of Action | Both act on GABA receptors in the brain, enhancing inhibitory effects |
| Effects | Sedation, relaxation, reduced anxiety, impaired coordination, and cognition |
| Medical Use | Benzos: Anxiety, insomnia, seizures; Alcohol: No medical use, but sometimes used socially |
| Addiction Potential | Both are highly addictive and can lead to physical dependence |
| Withdrawal Symptoms | Severe anxiety, insomnia, seizures (benzos); Tremors, hallucinations, seizures (alcohol) |
| Legal Status | Benzos: Prescription-only; Alcohol: Legal for adults in most countries |
| Overdose Risk | Both can cause fatal overdose, especially when combined |
| Long-term Effects | Cognitive impairment, memory issues, liver damage (alcohol), tolerance, and dependence |
| Interaction | Combining benzos and alcohol increases sedation, respiratory depression, and overdose risk |
| Detection | Benzos: Detectable in urine, blood, hair; Alcohol: Detectable in breath, blood, urine |
| Treatment for Dependence | Medical detox, therapy, and support groups for both substances |
| Social Perception | Alcohol is socially accepted; benzos are often stigmatized despite medical use |
Explore related products






What You'll Learn
- Chemical Composition Differences: Benzodiazepines are prescription drugs, while alcohol is a central nervous system depressant
- Effects on the Brain: Both enhance GABA activity, but through different mechanisms and receptors
- Addiction Potential: Both are highly addictive, but withdrawal symptoms and timelines differ significantly
- Health Risks: Alcohol causes liver damage; benzos risk respiratory depression and cognitive impairment
- Interaction Dangers: Combining benzos and alcohol increases sedation, overdose risk, and fatal outcomes
![]()
Chemical Composition Differences: Benzodiazepines are prescription drugs, while alcohol is a central nervous system depressant
Benzodiazepines and alcohol, though both capable of inducing relaxation and sedation, originate from fundamentally different chemical structures and mechanisms of action. Benzodiazepines, such as diazepam (Valium) or alprazolam (Xanax), are synthetic compounds designed to enhance the activity of gamma-aminobutyric acid (GABA), a neurotransmitter that inhibits brain activity. Their molecular structure allows them to bind specifically to benzodiazepine receptors on GABA-A receptors, increasing chloride ion influx and producing a calming effect. Alcohol, on the other hand, is an organic compound (ethanol) that acts as a non-specific central nervous system depressant. It modulates multiple neurotransmitter systems, including GABA and glutamate, but lacks the precise receptor binding seen in benzodiazepines. This distinction in chemical composition underpins their differing therapeutic uses and potential risks.
Consider the practical implications of these differences. Benzodiazepines are prescribed in controlled doses—for example, 0.25 to 2 mg of alprazolam for anxiety—and are intended for short-term use due to their high risk of dependence. Alcohol, however, is self-administered in varying quantities, often without medical oversight, and its effects depend on blood alcohol concentration (BAC). A BAC of 0.08% impairs motor skills, while higher levels can lead to unconsciousness or death. While both substances depress the central nervous system, benzodiazepines act with pharmacological precision, whereas alcohol’s effects are diffuse and unpredictable. This makes benzodiazepines more suitable for targeted medical treatment, such as managing panic disorders or seizures, while alcohol’s use is primarily recreational and carries broader health risks.
A critical takeaway is the danger of combining these substances. Both benzodiazepines and alcohol potentiate each other’s depressant effects, increasing the risk of respiratory depression, coma, or fatal overdose. For instance, mixing 1 mg of lorazepam (Ativan) with even moderate alcohol consumption can dangerously suppress brain function. Medical guidelines explicitly warn against concurrent use, yet accidental or intentional co-ingestion remains a common cause of emergency room visits. Understanding their distinct chemical mechanisms highlights why this combination is particularly hazardous: benzodiazepines’ targeted GABA enhancement, when paired with alcohol’s broad-spectrum depression, creates a synergistic effect that overwhelms the body’s regulatory systems.
To illustrate further, imagine a scenario where a 30-year-old patient takes 10 mg of diazepam for muscle spasms and later consumes two standard drinks (24 grams of ethanol). The diazepam’s half-life of 20–50 hours means it remains active in the system, while alcohol’s rapid absorption exacerbates sedation. This interaction is not merely additive but multiplicative, as both substances compete for metabolic pathways in the liver, prolonging their presence in the bloodstream. Practical advice includes avoiding alcohol entirely while on benzodiazepines and informing healthcare providers of all substance use to prevent such risks. These chemical differences are not just academic—they dictate real-world safety protocols and treatment strategies.
Uninstall Alcohol 120% Easily: Step-by-Step Guide for Complete Removal
You may want to see also
Explore related products






![]()
Effects on the Brain: Both enhance GABA activity, but through different mechanisms and receptors
Benzodiazepines and alcohol, though distinct in origin and use, converge on a shared neurological target: the GABA system. Both substances enhance the activity of gamma-aminobutyric acid (GABA), the brain’s primary inhibitory neurotransmitter, but they achieve this through different mechanisms and receptors. This distinction is critical for understanding their effects, risks, and interactions.
Consider the mechanism of action. Alcohol acts as a non-specific modulator, binding to GABA-A receptors and increasing chloride ion influx, which hyperpolarizes neurons and reduces their excitability. This process underlies alcohol’s sedative and anxiolytic effects. Benzodiazepines, however, are more precise. They bind to specific sites on the GABA-A receptor complex, enhancing the affinity of GABA for its binding site and amplifying its inhibitory effects. For instance, a single dose of diazepam (5–10 mg) can produce sedation comparable to a blood alcohol concentration (BAC) of 0.05–0.10%, but with a more targeted neurological impact.
The receptor specificity of benzodiazepines explains their therapeutic advantages and risks. By acting on particular subunits of the GABA-A receptor, they can alleviate anxiety or induce sleep with fewer peripheral effects compared to alcohol. However, this specificity also contributes to their potential for dependence. Chronic use of benzodiazepines alters receptor sensitivity, leading to tolerance and withdrawal symptoms upon cessation. Alcohol, in contrast, affects a broader range of receptors and ion channels, resulting in more diffuse and unpredictable effects, including cognitive impairment and organ damage at higher doses (e.g., BAC > 0.20%).
Practical implications arise from these differences. Combining benzodiazepines and alcohol is particularly dangerous because both depress the central nervous system, increasing the risk of respiratory failure or overdose. For individuals prescribed benzodiazepines, even moderate alcohol consumption (e.g., 1–2 standard drinks) can potentiate sedation and impair motor function. Conversely, those with alcohol use disorder may experience exacerbated withdrawal symptoms if benzodiazepines are abruptly discontinued. Clinicians often use benzodiazepines to manage alcohol withdrawal precisely because of their GABA-enhancing properties, but this requires careful titration to avoid over-sedation.
In summary, while both substances enhance GABA activity, their distinct mechanisms and receptor interactions dictate their effects and risks. Understanding these differences is essential for safe use, treatment planning, and harm reduction. For example, a patient prescribed alprazolam (0.25–0.5 mg) for anxiety should avoid alcohol entirely, whereas someone in alcohol detoxification may require a tapered benzodiazepine regimen (e.g., chlordiazepoxide 50–100 mg/day) under medical supervision. This nuanced approach ensures therapeutic benefits without compounding dangers.
Waking Up with a Hangover: Do You Still Smell Like Alcohol?
You may want to see also
Explore related products






![]()
Addiction Potential: Both are highly addictive, but withdrawal symptoms and timelines differ significantly
Benzodiazepines and alcohol share a notorious trait: both are highly addictive, yet their withdrawal landscapes are starkly different. This distinction is critical for anyone navigating the complexities of addiction or supporting someone who is. While both substances act on the central nervous system, their mechanisms of dependence and the body’s response to cessation vary widely, demanding tailored approaches to treatment and recovery.
Consider the withdrawal timeline. Alcohol withdrawal can manifest as early as 6 hours after the last drink, with symptoms ranging from mild anxiety and tremors to severe complications like seizures or delirium tremens (DTs), which can be life-threatening. For instance, a heavy drinker (defined as consuming 15 drinks or more per week for men, or 8 or more for women) is at higher risk for DTs, typically peaking 48–72 hours after cessation. In contrast, benzodiazepine withdrawal often begins 1–4 days after stopping short-acting benzos (e.g., Xanax) or 2–7 days for long-acting ones (e.g., Valium). Symptoms include rebound anxiety, insomnia, and in severe cases, seizures, though the risk of DTs is absent. This timeline underscores the need for medical supervision, especially when tapering off benzos, as abrupt discontinuation can exacerbate symptoms.
The severity of withdrawal also hinges on dosage and duration of use. Chronic alcohol use, particularly at levels exceeding 4–5 standard drinks daily, rewires the brain’s GABA receptors, leading to heightened withdrawal intensity. Similarly, benzodiazepines, when used beyond their recommended 2–4 week window, can cause physical dependence, even at therapeutic doses (e.g., 2–4 mg of diazepam daily). For example, a patient prescribed Xanax for panic disorder who takes 3 mg daily for 6 months is at significant risk for withdrawal if the medication is stopped abruptly. This highlights the importance of gradual tapering under medical guidance, reducing the dose by no more than 10% every 1–2 weeks for long-acting benzos.
Practical tips for managing withdrawal differ between the two substances. For alcohol, hydration, a balanced diet, and medications like benzodiazepines (ironically) or anticonvulsants (e.g., carbamazepine) can mitigate symptoms. For benzos, a slow taper is non-negotiable; switching to a long-acting benzo like diazepam allows for more precise dose reductions. Supportive therapies, such as cognitive-behavioral therapy (CBT) or mindfulness-based practices, are invaluable for both, addressing the psychological cravings that often accompany physical withdrawal.
In conclusion, while both benzos and alcohol carry a high addiction potential, their withdrawal profiles demand distinct strategies. Understanding these differences—timelines, symptom severity, and management techniques—empowers individuals and healthcare providers to navigate recovery more effectively. Whether addressing alcohol’s rapid-onset withdrawal or benzos’ protracted symptoms, a tailored, informed approach is key to breaking the cycle of addiction.
Alcohol and COVID-19: Separating Fact from Fiction in the Pandemic
You may want to see also
Explore related products





![[(Benzodiazepine: Abuse & Therapeutic Uses, Pharmacology & Health Effects)] [Author: Armando L. Soto] published on (October, 2012)](https://m.media-amazon.com/images/I/71GvR-tHeWL._AC_UL320_.jpg)
![]()
Health Risks: Alcohol causes liver damage; benzos risk respiratory depression and cognitive impairment
Alcohol and benzodiazepines (benzos) may both be central nervous system depressants, but their health risks diverge sharply. Alcohol is notorious for its cumulative toll on the liver, with chronic consumption leading to conditions like fatty liver disease, cirrhosis, and hepatocellular carcinoma. Even moderate drinking—defined as up to one drink per day for women and two for men—can escalate to liver damage over time, particularly when paired with poor diet or pre-existing conditions. In contrast, benzos pose an immediate threat to respiratory function, especially at high doses or when combined with other depressants like alcohol. A single benzodiazepine dose exceeding 2 mg of lorazepam or 10 mg of diazepam can depress breathing to dangerous levels, particularly in individuals over 65 or those with respiratory conditions like COPD.
While alcohol’s cognitive impairments are often temporary—slurred speech, memory lapses, and slowed reaction times during intoxication—benzos can inflict lasting cognitive damage. Prolonged benzo use, especially beyond 4–6 weeks, has been linked to deficits in executive function, memory consolidation, and psychomotor performance. For instance, older adults prescribed long-term benzodiazepines (e.g., 0.5 mg clonazepam daily) face a 50% higher risk of developing dementia compared to non-users. Conversely, alcohol’s cognitive effects are dose-dependent: a blood alcohol concentration (BAC) of 0.08% impairs judgment and coordination, while chronic abuse can lead to Wernicke-Korsakoff syndrome, a thiamine deficiency causing permanent memory loss.
To mitigate these risks, consider practical strategies tailored to each substance. For alcohol, limit intake to 7 drinks per week for women and 14 for men, with at least 2 alcohol-free days to allow liver recovery. Pair alcohol with food to slow absorption, and avoid mixing it with benzos or other sedatives. For benzodiazepines, adhere strictly to prescribed dosages (e.g., 2–10 mg diazepam daily for anxiety) and taper under medical supervision after short-term use. Never combine benzos with opioids or alcohol, as this synergy increases respiratory depression risk by 300%.
The interplay between alcohol and benzos exacerbates their individual dangers. Even small amounts—say, 2 drinks plus 1 mg of alprazolam—can suppress breathing to life-threatening levels. This combination is particularly perilous for individuals with sleep apnea or obesity, where baseline respiratory function is already compromised. Emergency rooms frequently treat cases of benzo-alcohol overdose, often requiring intubation or naloxone administration to reverse respiratory failure.
Ultimately, while both substances depress the CNS, their health risks demand distinct precautions. Alcohol’s insidious liver damage accumulates silently over years, whereas benzos pose an acute, often immediate threat to respiration and cognition. Awareness of these differences—coupled with strict adherence to dosage guidelines and avoidance of polysubstance use—is critical for minimizing harm. Whether prescribed or recreational, neither substance should be approached casually, as their consequences are neither identical nor reversible.
1950s Alcohol Arrests: Uncovering the Stories Behind the Headlines
You may want to see also
Explore related products






![]()
Interaction Dangers: Combining benzos and alcohol increases sedation, overdose risk, and fatal outcomes
Benzos and alcohol both depress the central nervous system, but their combined effects are far from additive—they’re multiplicative. Alone, a standard dose of a benzodiazepine like diazepam (5–10 mg) or a moderate alcohol intake (1–2 drinks) may produce mild sedation. Together, even these low-to-moderate amounts can trigger profound drowsiness, impaired coordination, and respiratory depression. This isn’t a matter of 1 + 1 = 2; it’s closer to 1 + 1 = 5, with the body’s systems overwhelmed by the dual assault.
Consider the mechanism: both substances enhance the activity of GABA, a neurotransmitter that slows brain function. When combined, they create a synergistic effect, amplifying each other’s depressant properties. For instance, a 20-year-old taking 10 mg of alprazolam (Xanax) alongside three alcoholic drinks might experience sedation equivalent to taking 30 mg of alprazolam alone—a dose that significantly heightens overdose risk. The danger lies in unpredictability; users often underestimate how quickly tolerance shifts when mixing substances, leading to accidental overconsumption.
The overdose risk escalates sharply with this combination. Respiratory depression, a hallmark of both benzos and alcohol, becomes life-threatening when they’re paired. A study in the *Journal of Addiction Medicine* found that 20% of benzodiazepine-related ER visits involved alcohol co-ingestion, with respiratory failure being the most common complication. Practical tip: if you’re prescribed benzos, avoid alcohol entirely. Even a single drink can impair judgment, making it harder to stick to prescribed dosages. For those not on prescription benzos, the advice is equally clear: never mix recreational benzos (e.g., counterfeit Xanax bars) with alcohol, as potency and purity are often unknown.
Fatal outcomes are not rare in this scenario. The CDC reports that benzodiazepines contributed to over 12,000 overdose deaths in 2021, with alcohol involvement in nearly 30% of cases. Age plays a role too; older adults (65+) metabolize both substances more slowly, increasing vulnerability. For example, a 70-year-old taking 5 mg of lorazepam (Ativan) with a glass of wine faces a higher risk of falls or respiratory arrest than a younger individual due to age-related physiological changes.
To mitigate these dangers, follow these steps: first, disclose all substance use to your healthcare provider, including alcohol consumption. Second, if prescribed benzos, use them strictly as directed and store them securely. Third, educate yourself and others about the risks—awareness saves lives. Finally, if you suspect an overdose (symptoms include extreme drowsiness, slowed breathing, or unresponsiveness), call emergency services immediately. Combining benzos and alcohol isn’t just risky; it’s a gamble with fatal stakes.
Where to Buy Alcohol: Liquor or Grocery Store?
You may want to see also
Frequently asked questions
No, benzos (benzodiazepines) and alcohol are not the same. Benzos are prescription medications used to treat anxiety, insomnia, and seizures, while alcohol is a central nervous system depressant commonly consumed as a beverage.
Both benzos and alcohol enhance the effects of GABA, a neurotransmitter that slows down brain activity, but they do so through slightly different mechanisms. Both can cause sedation, relaxation, and impaired coordination.
No, mixing benzos and alcohol is highly dangerous. Combining them increases the risk of severe sedation, respiratory depression, overdose, and even death.
Yes, withdrawal from both benzos and alcohol can cause similar symptoms, including anxiety, insomnia, tremors, and seizures. However, alcohol withdrawal can also lead to delirium tremens (DTs), a life-threatening condition.
Both benzos and alcohol carry a high risk of addiction, but the ease of addiction depends on individual factors like dosage, frequency of use, and personal susceptibility. Prolonged use of either substance can lead to physical and psychological dependence.