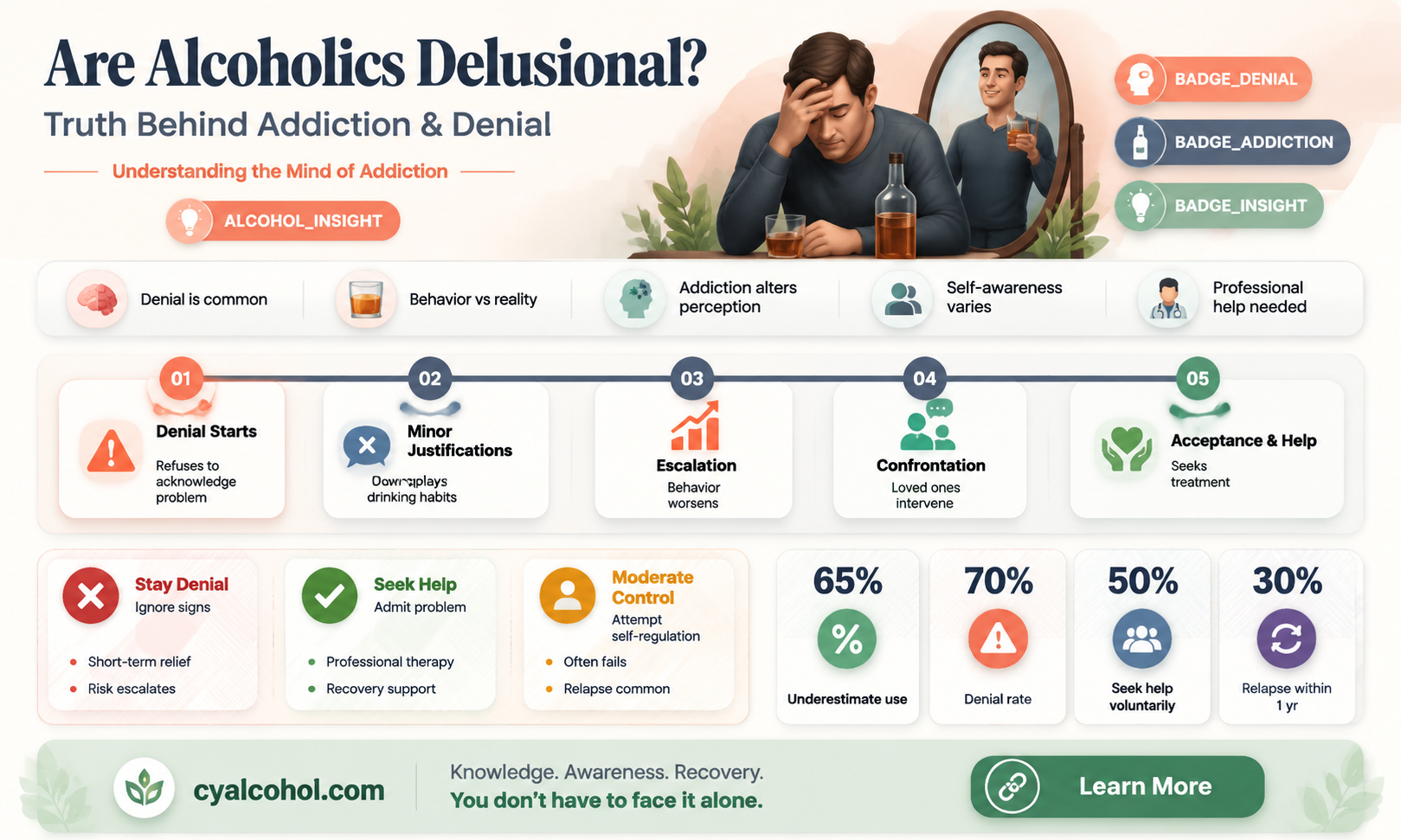
The question of whether alcoholics are delusional is a complex and multifaceted issue that intersects psychology, addiction science, and behavioral studies. Alcoholism, or alcohol use disorder, often distorts an individual's perception of reality, leading to denial about the severity of their drinking, justification of harmful behaviors, and an inflated sense of control over their addiction. These cognitive distortions can resemble delusional thinking, as individuals may cling to false beliefs despite overwhelming evidence to the contrary. However, it is important to distinguish between the temporary cognitive impairments caused by alcohol abuse and clinical delusions, which are persistent, fixed false beliefs characteristic of mental disorders like schizophrenia. While alcoholics may exhibit delusion-like behaviors, their distorted thinking is often rooted in the psychological and physiological effects of addiction rather than a primary psychotic condition, highlighting the need for nuanced understanding and targeted interventions.
Explore related products






What You'll Learn
![]()
Denial of addiction severity
Alcoholics often underestimate the severity of their addiction, a phenomenon deeply rooted in psychological defense mechanisms. This denial is not merely a lack of awareness but a complex interplay of cognitive distortions and emotional coping strategies. For instance, an individual might acknowledge occasional heavy drinking but rationalize it as a stress-relief tool rather than a dependency. Such minimization allows them to maintain a self-image that avoids the stigma of addiction, even as their behavior aligns with clinical criteria for alcoholism.
Consider the case of a 45-year-old professional who consumes 6–8 standard drinks daily but insists it’s “not a problem” because they function well at work. This self-deception often stems from comparing themselves to more visibly impaired individuals, a flawed benchmark that obscures their own deteriorating health. Research shows that 80% of alcoholics exhibit denial behaviors, often dismissing warning signs like blackouts, relationship strain, or declining liver function as temporary or insignificant.
To address this denial, intervention strategies must focus on reframing perception rather than confronting behavior directly. A practical approach involves using objective data, such as blood alcohol level charts or health metrics, to illustrate the cumulative impact of consumption. For example, explaining that 4–5 drinks per day for men (3–4 for women) qualifies as heavy drinking can disrupt the narrative of “moderate” use. Pairing this with a 30-day sobriety challenge can provide tangible evidence of withdrawal symptoms, forcing acknowledgment of physical dependence.
However, caution is necessary when challenging denial, as aggressive confrontation often triggers defensiveness. Instead, employ motivational interviewing techniques, asking open-ended questions like, “How do you think your drinking affects your long-term goals?” This encourages self-reflection without inducing shame. Additionally, involving trusted peers or family members in structured conversations can provide external perspectives that counteract internal rationalizations.
Ultimately, breaking through denial requires patience and a multi-faceted approach. Combining education, self-monitoring tools (e.g., drink-tracking apps), and professional support creates a pathway for acceptance. While denial serves as a protective barrier, dismantling it is the first step toward recovery, enabling individuals to confront the true severity of their addiction and seek appropriate treatment.
Can Alcohol-Based Mouthwash Trigger a False Positive on Breathalyzers?
You may want to see also
Explore related products




$89.59 $127.99


![]()
Belief in controlled drinking ability
Alcoholics often harbor a persistent belief in their ability to control their drinking, a conviction that can seem baffling to outsiders. This belief is not merely a lack of insight but a complex psychological defense mechanism rooted in denial and cognitive dissonance. For instance, an individual might insist they can limit themselves to "just one drink" at social events, despite a history of repeated failures. This self-deception allows them to avoid confronting the reality of their addiction, temporarily alleviating the emotional discomfort associated with admitting powerlessness over alcohol.
Consider the case of a 45-year-old professional who, after multiple DUI arrests and strained relationships, still claims to be able to drink moderately. They might rationalize their behavior by attributing past binges to stress or external circumstances, rather than acknowledging the underlying addiction. This pattern of thinking is not uncommon; studies show that up to 70% of individuals with alcohol use disorder (AUD) exhibit similar beliefs in controlled drinking during early stages of recovery. Such convictions often stem from a desire to maintain a sense of normalcy and autonomy, even when evidence suggests otherwise.
From a practical standpoint, challenging this belief requires a structured approach. Cognitive-behavioral therapy (CBT) is particularly effective, as it helps individuals identify and reframe irrational thoughts about alcohol control. For example, therapists might encourage clients to keep a drinking diary, noting triggers, quantities, and consequences. Over time, this practice can reveal patterns that contradict the notion of controlled drinking. Additionally, setting clear boundaries, such as abstaining from alcohol entirely for 30 days, can provide tangible evidence of the difficulty in moderating intake.
Comparatively, the belief in controlled drinking shares similarities with the "just one more" mentality seen in other addictions, such as gambling or smoking. In each case, the individual underestimates the addictive nature of the behavior, often overestimating their willpower. However, alcohol’s unique societal acceptance complicates matters further. Unlike illicit substances, alcohol is normalized and even glorified in many cultures, making it harder for individuals to recognize their loss of control. This societal backdrop reinforces the delusion, as the alcoholic may point to others who drink without issue as evidence that moderation is possible for them too.
Ultimately, the belief in controlled drinking is a significant barrier to recovery, but it is not insurmountable. By combining self-awareness, professional intervention, and a willingness to confront uncomfortable truths, individuals can dismantle this delusion. Practical steps, such as attending support groups like Alcoholics Anonymous (AA), can provide accountability and perspective. For those hesitant to seek help, starting with small, measurable goals—like reducing intake by 50% weekly—can serve as a reality check. The key lies in recognizing that true control is not about managing alcohol but about choosing to live without it.
Martinis: Alcohol Units in a Vodka Martini
You may want to see also
Explore related products





![]()
Underestimating health consequences
Alcoholics often downplay the severity of their drinking habits, a behavior rooted in cognitive dissonance. This psychological mechanism allows them to reconcile their actions with a positive self-image, despite overwhelming evidence of harm. For instance, a person consuming 5-7 standard drinks daily (well above the recommended limit of 1 drink per day for women and 2 for men) might insist, “I’m not an alcoholic; I just like to unwind.” This denial extends to health risks, where liver damage, cardiovascular issues, and increased cancer risk are brushed aside as “exaggerated” or “unlikely.” Such delusion isn’t merely ignorance—it’s a survival tactic for the ego, enabling continued harmful behavior.
Consider the case of a 45-year-old man who, despite experiencing frequent blackouts and elevated liver enzymes, claims, “My body can handle it.” This statement reflects a dangerous miscalculation of tolerance. Alcohol’s cumulative effects are insidious; cirrhosis, for example, can develop silently over years, with symptoms appearing only after irreversible damage has occurred. Yet, many alcoholics interpret their current lack of severe symptoms as proof of resilience, rather than a warning sign. This cognitive distortion is exacerbated by social normalization of heavy drinking, making it harder to recognize the line between “social drinking” and dependency.
To combat this delusion, practical steps can be taken. First, track alcohol consumption objectively—apps or journals can reveal patterns otherwise obscured by denial. Second, undergo regular health screenings, particularly liver function tests and blood pressure checks, to confront tangible evidence of harm. For those over 40, adding a cancer screening to the routine is critical, as alcohol increases the risk of seven types of cancer, including breast and colon. Third, engage in honest conversations with healthcare providers, who can offer unbiased assessments without judgment. These actions dismantle the delusion by replacing subjective beliefs with objective data.
A comparative analysis highlights the stark contrast between perception and reality. While an alcoholic might believe their drinking is “moderate,” studies show that even 3-4 drinks per day can reduce life expectancy by up to 5 years. This gap between self-perception and scientific fact underscores the depth of delusion. Unlike other addictions, alcohol’s legal status and cultural acceptance make it easier to rationalize excessive use. However, this normalization doesn’t negate its toxicity—ethanol is a carcinogen, and its metabolic byproduct, acetaldehyde, damages DNA. Recognizing these truths is the first step toward breaking the cycle of denial.
Finally, a persuasive argument must be made: underestimating health consequences isn’t just a personal failing—it’s a societal blind spot. Public health campaigns often focus on acute risks like drunk driving, neglecting the chronic dangers of long-term consumption. By reframing the narrative to emphasize cumulative harm, we can challenge the delusion at its core. For instance, visualizing the impact of 10 years of heavy drinking—a 50% increased risk of stroke, a 30% higher chance of dementia—can be more effective than abstract warnings. Ultimately, confronting this delusion requires both individual accountability and systemic education, ensuring that no one remains oblivious to the silent toll of alcohol.
Understanding Alcohol Peak Times Post-Metabolism: Key Insights and Factors
You may want to see also
Explore related products






![]()
Rationalizing harmful behaviors
Alcoholics often engage in a mental gymnastics routine to justify their drinking, a process known as rationalization. This cognitive distortion allows them to maintain a sense of control and normalcy despite the evident harm caused by their addiction. One common tactic is minimizing the severity of their alcohol consumption. For instance, an alcoholic might compare themselves to others who drink more, thinking, "I'm not as bad as John, who finishes a bottle of whiskey daily." This comparison provides a false sense of security, ignoring the fact that any amount of alcohol can be harmful when it leads to dependency and negatively impacts one's life.
Unraveling the Rationalization Process:
The rationalization process can be broken down into several steps. First, the individual identifies a behavior they want to continue, such as drinking alcohol. Then, they search for reasons to justify this behavior, often twisting facts or ignoring evidence. For example, an alcoholic might convince themselves that drinking helps them cope with stress, despite numerous studies showing that alcohol is a depressant and can exacerbate anxiety and depression. This self-deception is a powerful tool, enabling them to temporarily silence the voice of reason.
The Dangers of Self-Deception:
Engaging in this type of self-deception can have severe consequences. It delays the acceptance of a problem, which is the first step towards recovery. According to the National Institute on Alcohol Abuse and Alcoholism, about 90% of adults in the United States who drink excessively report binge drinking, defined as consuming 4 or more drinks for women and 5 or more for men on an occasion. Yet, many of these individuals might rationalize their behavior, believing they can stop anytime, when in reality, their bodies may already be dependent on alcohol. This denial can lead to increased health risks, including liver disease, cardiovascular problems, and a higher susceptibility to certain cancers.
Breaking Free from Rationalization:
To overcome this harmful pattern, one must first recognize these rationalizations for what they are—defensive mechanisms. Keeping a drinking diary can be an eye-opening exercise. Note down every drink, the amount, and the reasons or excuses given for drinking. Over time, patterns will emerge, revealing the frequency and triggers of alcohol consumption. This awareness is crucial in challenging the delusions and taking control. Additionally, seeking support from professionals or support groups can provide the necessary tools to counter these rationalizations and foster a healthier relationship with alcohol or, ideally, abstinence.
In the journey towards recovery, understanding and dismantling these rationalizations is a critical step. It empowers individuals to make informed decisions, free from the chains of self-deception, and encourages a more honest and healthy lifestyle. This process is not about self-blame but about self-awareness and the courage to face one's vulnerabilities.
When to Buy Alcohol: Seasonal Price Drops and Savings Tips
You may want to see also
Explore related products





![]()
Ignoring negative impacts on relationships
Alcoholics often exhibit a pattern of minimizing or outright ignoring the damage their drinking inflicts on personal relationships. This behavior isn’t merely a lack of awareness but a deliberate cognitive shift to protect their addiction. For instance, a 45-year-old man might dismiss his wife’s concerns about his nightly binge drinking (defined as 5+ drinks for men in a session) as her being "overly dramatic," even after repeated arguments and emotional distance. This denial serves as a psychological shield, allowing him to avoid confronting the need for change.
Consider the mechanics of this denial. When confronted with evidence of harm—a missed family event, broken promises, or strained communication—alcoholics frequently reframe the situation. They might blame external factors ("I was stressed at work") or shift responsibility onto others ("You’re the one who can’t handle my drinking"). This cognitive distortion is rooted in the brain’s attempt to reconcile addictive behavior with self-preservation, a phenomenon observed in studies on substance use disorders. Over time, this pattern erodes trust, yet the alcoholic remains insulated from the emotional fallout by their own narrative.
To address this, intervention strategies must focus on breaking through the denial barrier. One practical approach is the CRAFT method (Community Reinforcement and Family Training), which teaches loved ones to reward positive behaviors and set clear boundaries without enabling. For example, instead of arguing about drinking, a partner could say, "I’ll plan a weekend trip if you attend two AA meetings this week." This shifts the focus from blame to actionable steps, bypassing the alcoholic’s tendency to deflect.
However, caution is necessary. Confrontational approaches, like traditional interventions, often backfire by triggering defensiveness. Alcoholics may double down on their delusion, perceiving criticism as an attack rather than a plea for change. A more effective tactic is to highlight specific, observable consequences without judgment. For instance, "I noticed you weren’t at Sarah’s graduation—she was really hurt" is more impactful than "You’re always drunk and missing important moments."
In conclusion, ignoring relationship harm is a survival mechanism for alcoholics, not a character flaw. By understanding the psychological underpinnings and employing strategic communication, loved ones can create pathways to awareness without reinforcing the cycle of denial. The goal isn’t to force admission of guilt but to gently illuminate the disconnect between their actions and their self-perception, one step at a time.
Understanding Alcohol Units: What Does 80 Milligrams Mean?
You may want to see also
Frequently asked questions
Alcoholics may experience delusions, particularly during severe withdrawal (delirium tremens) or prolonged heavy drinking, but not all alcoholics are delusional.
Delusions in alcoholics can result from alcohol-induced brain changes, withdrawal symptoms, or conditions like Wernicke-Korsakoff syndrome, which is linked to thiamine deficiency.
Prolonged alcoholism can cause lasting brain damage, potentially leading to persistent delusional thinking, especially if conditions like Korsakoff syndrome develop.
Signs include persistent false beliefs, paranoia, or hallucinations, often accompanied by confusion, agitation, or memory loss, particularly during withdrawal or heavy use.
Yes, treatment involves addressing alcohol dependence, managing withdrawal safely, and providing medical care for related conditions like thiamine deficiency or mental health disorders.