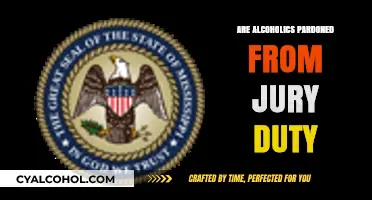
The relationship between alcoholism and vitamin B12 deficiency is a significant concern in the medical community, as chronic alcohol consumption can impair the absorption and utilization of this essential nutrient. Vitamin B12, crucial for nerve function, DNA synthesis, and red blood cell production, is primarily absorbed in the small intestine, a process that relies on intrinsic factor, a protein produced in the stomach. Alcoholics often experience gastrointestinal issues, including inflammation and reduced stomach acid production, which can hinder intrinsic factor secretion and subsequently impair B12 absorption. Additionally, poor dietary choices and malnutrition commonly associated with alcoholism further exacerbate the risk of deficiency. Prolonged B12 deficiency can lead to severe health complications, such as anemia, neurological damage, and cognitive impairment, making it imperative to address this issue in individuals struggling with alcohol addiction. Understanding this link is vital for developing targeted interventions to improve health outcomes for alcoholics.
| Characteristics | Values |
|---|---|
| Prevalence of B12 Deficiency in Alcoholics | High; studies show 20-60% of alcoholics have B12 deficiency |
| Primary Cause of Deficiency | Poor dietary intake, malabsorption due to gastrointestinal damage, and impaired storage in the liver |
| Mechanisms of Deficiency | Reduced gastric acid secretion (needed for B12 absorption), mucosal atrophy, and pancreatic insufficiency |
| Symptoms of B12 Deficiency | Fatigue, weakness, neurological issues (e.g., numbness, tingling), anemia, and cognitive decline |
| Long-Term Risks | Peripheral neuropathy, dementia, megaloblastic anemia, and irreversible nerve damage |
| Diagnostic Methods | Serum B12 levels, methylmalonic acid (MMA), and homocysteine tests |
| Treatment Options | Oral or injectable B12 supplements, improved diet, and alcohol cessation |
| Prevention Strategies | Nutritional counseling, B12 supplementation, and addressing alcohol dependency |
| Association with Other Nutrient Deficiencies | Often concurrent with deficiencies in folate, thiamine, and other B vitamins |
| Impact of Alcohol on B12 Metabolism | Interferes with B12 absorption, transport, and utilization in the body |
Explore related products






What You'll Learn
![]()
B12 absorption issues in alcoholics
Chronic alcohol consumption disrupts the intricate process of vitamin B12 absorption, a vital nutrient for nerve function, DNA synthesis, and red blood cell production. This disruption occurs at multiple stages, creating a cascade of deficiencies. Firstly, alcohol irritates the stomach lining, impairing the production of intrinsic factor, a protein essential for B12 absorption in the small intestine. Without sufficient intrinsic factor, B12 remains unabsorbed, passing through the digestive system unused. Secondly, alcohol damages the mucosal lining of the small intestine itself, further hindering B12 uptake. This dual assault on the digestive system leaves alcoholics particularly vulnerable to B12 deficiency, even if their dietary intake is adequate.
Studies show that up to 80% of alcoholics exhibit some degree of B12 deficiency, with symptoms ranging from fatigue and weakness to neurological complications like numbness, tingling, and cognitive decline.
The consequences of B12 deficiency in alcoholics extend beyond general fatigue. Peripheral neuropathy, characterized by pain, tingling, and weakness in the hands and feet, is a common and debilitating complication. More severe cases can lead to irreversible nerve damage and even dementia. Alcoholics are also at increased risk for megaloblastic anemia, a condition where the body produces abnormally large, immature red blood cells, leading to weakness, pale skin, and shortness of breath.
Recognizing the signs of B12 deficiency is crucial for early intervention. Alcoholics experiencing persistent fatigue, neurological symptoms, or changes in mood should seek medical attention. A simple blood test can diagnose B12 deficiency, and treatment typically involves B12 supplementation, either orally or through injections.
Addressing B12 deficiency in alcoholics requires a multi-pronged approach. While supplementation is essential, addressing the root cause – alcohol consumption – is paramount. Reducing alcohol intake or achieving sobriety is crucial for long-term B12 absorption and overall health. Additionally, dietary modifications can support B12 levels. Incorporating B12-rich foods like meat, poultry, fish, eggs, and dairy products can be beneficial. However, due to the absorption issues caused by alcohol, supplementation may still be necessary.
It's important to note that B12 supplementation should be done under medical supervision. High doses of B12 can mask other deficiencies, and the appropriate dosage and form of supplementation (oral vs. injectable) should be determined by a healthcare professional. By understanding the unique challenges of B12 absorption in alcoholics and implementing a comprehensive treatment plan, individuals can mitigate the devastating consequences of this deficiency and improve their overall health and well-being.
Should Parents Allow Minors to Consume Alcohol? A Debate
You may want to see also
Explore related products






![]()
Alcohol’s impact on B12 metabolism
Chronic alcohol consumption disrupts vitamin B12 metabolism at multiple stages, creating a vicious cycle of deficiency. Alcohol interferes with the stomach's production of intrinsic factor, a protein essential for B12 absorption in the small intestine. Studies show that even moderate drinkers (1-2 drinks per day) can experience a 5-10% reduction in intrinsic factor production, while heavy drinkers may see decreases of up to 50%. This impairment means that even if an alcoholic consumes adequate B12 through diet, their body struggles to utilize it effectively.
Example: A 45-year-old man with a 10-year history of heavy drinking presents with numbness and tingling in his hands and feet. Blood tests reveal a B12 level of 150 pg/mL (normal range: 200-900 pg/mL), despite a diet rich in meat and dairy. His intrinsic factor levels are significantly reduced, directly linking his alcoholism to his B12 deficiency.
Beyond absorption, alcohol wreaks havoc on the liver, the body's primary storage site for B12. Chronic alcohol use leads to liver damage, reducing its capacity to store and release B12 into the bloodstream. This depletion further exacerbates the deficiency, as the body cannot draw upon its reserves. Analysis: Research indicates that alcoholics often have liver stores of B12 that are 30-50% lower than non-drinkers, even when dietary intake is comparable. This highlights the dual impact of alcohol on both absorption and storage mechanisms.
Takeaway: Addressing B12 deficiency in alcoholics requires a two-pronged approach: reducing alcohol intake to restore intrinsic factor production and potentially supplementing with high-dose B12 injections to bypass the damaged absorption pathway and replenish depleted liver stores.
The consequences of B12 deficiency in alcoholics extend far beyond fatigue and weakness. Comparative: While the general population may experience mild symptoms like fatigue and pale skin, alcoholics are at heightened risk for severe neurological complications due to the combined effects of B12 deficiency and alcohol's direct neurotoxicity. Peripheral neuropathy, characterized by numbness, tingling, and pain in the extremities, is particularly common. More alarmingly, untreated B12 deficiency can lead to irreversible spinal cord damage, resulting in difficulty walking and even paralysis.
Practical Tip: Alcoholics experiencing neurological symptoms should seek immediate medical attention. Early diagnosis and treatment with B12 injections can prevent permanent nerve damage.
Effective Strategies to Regulate Alcohol Consumption and Promote Public Health
You may want to see also
Explore related products






![]()
Symptoms of B12 deficiency in alcoholics
Chronic alcohol consumption interferes with vitamin B12 absorption, leading to deficiencies that manifest in distinct symptoms among alcoholics. Unlike the general population, where B12 deficiency might stem from dietary inadequacies or malabsorption issues, alcoholics face a dual challenge: reduced intake of B12-rich foods and impaired absorption due to alcohol-induced damage to the stomach and intestines. This unique interplay exacerbates the risk, making it crucial to recognize the symptoms early.
Neurological Manifestations: The Silent Alarm
Alcoholics with B12 deficiency often experience neurological symptoms that mimic or compound alcohol-related nerve damage. Tingling or numbness in the hands and feet, known as peripheral neuropathy, is a hallmark. Unlike the transient numbness from acute alcohol consumption, this sensation persists and worsens over time. Cognitive changes, such as memory loss, confusion, and difficulty concentrating, may also arise. These symptoms are frequently overlooked, attributed solely to alcohol’s neurotoxic effects, but they signal a deeper nutritional deficit. For instance, a study in the *Journal of Clinical Medicine* highlighted that 40% of alcoholics with B12 deficiency exhibited irreversible nerve damage when diagnosis was delayed beyond six months.
Hematological Red Flags: Beyond Fatigue
Fatigue is a common complaint among alcoholics, often dismissed as a consequence of poor lifestyle choices. However, B12 deficiency triggers megaloblastic anemia, characterized by large, immature red blood cells that fail to transport oxygen efficiently. This results in profound fatigue, weakness, and shortness of breath, even during minimal exertion. Pale or jaundiced skin, a consequence of red blood cell breakdown, may also appear. A simple complete blood count (CBC) can reveal these abnormalities, but clinicians must correlate them with alcohol history to pinpoint B12 deficiency as the root cause.
Gastrointestinal Clues: The Overlooked Link
Alcoholics frequently suffer from gastrointestinal issues, but certain symptoms should raise suspicion of B12 deficiency. Glossitis, or a swollen, smooth tongue, is a telltale sign, often accompanied by mouth ulcers or a burning sensation. Chronic diarrhea or constipation, unrelated to acute alcohol-induced irritation, may also occur due to impaired gut motility from B12 deficiency. These symptoms are easily dismissed as alcohol-related gastritis but warrant investigation, especially if paired with neurological or hematological signs.
Practical Steps for Identification and Management
Early detection hinges on recognizing the interplay between alcohol’s effects and B12 deficiency. Clinicians should screen alcoholics with a serum B12 test, though false negatives can occur due to elevated folate levels masking deficiency. Methylmalonic acid (MMA) and homocysteine levels are more reliable markers. Treatment involves high-dose oral B12 (1000–2000 mcg daily) or intramuscular injections (1000 mcg monthly), coupled with alcohol cessation to restore absorption. For severe neurological symptoms, weekly injections may be necessary for several months. Patients should also incorporate B12-rich foods like fortified cereals, dairy, and eggs, though dietary changes alone are insufficient for alcoholics due to absorption issues.
In summary, B12 deficiency in alcoholics presents a unique clinical picture, blending neurological, hematological, and gastrointestinal symptoms. Awareness of these manifestations, coupled with targeted screening and aggressive supplementation, can prevent irreversible damage and improve outcomes.
DXM and Alcohol Interaction: Potentiation Risks and Safety Concerns
You may want to see also
Explore related products






![]()
Dietary B12 intake in alcoholics
Chronic alcohol consumption disrupts the body's ability to absorb and utilize vitamin B12 effectively. This essential nutrient, crucial for nerve function, DNA synthesis, and red blood cell production, relies on a complex digestive process. Alcohol interferes at multiple stages: it damages the stomach lining, reducing the production of intrinsic factor, a protein essential for B12 absorption in the small intestine. Additionally, alcohol irritates the intestinal lining, further hindering nutrient uptake. Even if an alcoholic consumes adequate B12 through diet, their body may struggle to extract and utilize it, leading to a functional deficiency.
Alcoholics often experience poor dietary habits, further exacerbating their B12 status. B12 is primarily found in animal products like meat, fish, dairy, and eggs. Alcoholics may neglect these food groups due to financial constraints, lack of appetite, or the prioritization of alcohol over nutritious meals. This dietary inadequacy, coupled with impaired absorption, creates a double whammy, significantly increasing the risk of B12 deficiency in this population.
Addressing B12 deficiency in alcoholics requires a multi-pronged approach. Firstly, reducing alcohol intake is paramount. Even moderate decreases can improve gut health and enhance B12 absorption. Secondly, dietary modifications are crucial. Encouraging the consumption of B12-rich foods, such as fortified cereals, nutritional yeast, and B12-fortified plant-based milks, can help bridge the dietary gap. For severe deficiencies, B12 supplementation may be necessary. Oral supplements or injections, under medical supervision, can rapidly replenish B12 stores.
Regular monitoring of B12 levels is essential for alcoholics. Blood tests can detect deficiencies early, allowing for prompt intervention. Healthcare professionals should be vigilant in screening alcoholics for B12 deficiency, as its symptoms, like fatigue, weakness, and neurological issues, can be mistaken for alcohol-related effects. Early diagnosis and treatment are crucial to prevent irreversible nerve damage and other complications associated with B12 deficiency.
Why Ethyl Alcohol is Key to Gram Staining
You may want to see also
Explore related products






![]()
B12 supplementation for alcoholic patients
Chronic alcohol consumption disrupts vitamin B12 absorption, leading to deficiencies in many alcoholic patients. This occurs due to alcohol's interference with intrinsic factor production in the stomach, a protein essential for B12 uptake in the intestines. As a result, even if dietary intake is adequate, alcoholics often struggle to maintain healthy B12 levels.
B12 deficiency can exacerbate the already severe health consequences of alcoholism, contributing to neurological damage, anemia, and cognitive impairment. Supplementation becomes crucial in these cases, not just as a preventative measure but as a therapeutic intervention.
Identifying Deficiency and Initiating Supplementation
Diagnosing B12 deficiency in alcoholics requires a two-pronged approach. Blood tests measuring serum B12 levels are standard, but they can be misleading due to the presence of analogues that don't function properly. Assessing methylmalonic acid (MMA) levels, a more specific marker of B12 deficiency, is often recommended for greater accuracy. Once deficiency is confirmed, supplementation should begin promptly. Oral B12 supplements, typically in the range of 1000-2000 mcg daily, are generally effective. However, in severe cases or when absorption is severely compromised, intramuscular injections of B12 (1000 mcg monthly) may be necessary.
Considerations and Long-Term Management
While supplementation is vital, it's not a standalone solution. Addressing the underlying alcoholism is paramount. Encouraging dietary changes to include B12-rich foods like meat, fish, dairy, and fortified cereals can complement supplementation efforts. Regular monitoring of B12 levels and MMA is essential to ensure the effectiveness of treatment and adjust dosages as needed. Long-term management involves a holistic approach, combining B12 supplementation with alcoholism treatment and nutritional support to promote overall health and prevent further complications.
Do Bugs Despise Alcohol? Unraveling the Truth Behind the Myth
You may want to see also
Frequently asked questions
Yes, alcoholics are at a higher risk of vitamin B12 deficiency due to poor dietary intake, impaired absorption in the gut, and liver dysfunction caused by chronic alcohol consumption.
Alcohol interferes with the absorption of vitamin B12 in the stomach and small intestine, reduces the production of intrinsic factor (necessary for B12 absorption), and damages the liver, which stores B12.
Symptoms include fatigue, weakness, numbness or tingling in the hands and feet, memory problems, anemia, and in severe cases, neurological issues like difficulty walking or balance problems.
Yes, with proper treatment, including B12 supplementation, dietary changes, and reducing alcohol intake, the deficiency can be reversed. However, long-term alcohol abuse may cause permanent damage if not addressed promptly.